
From the 1Department of Physical and Rehabilitation Medicine, Hacettepe University Medical School, Ankara, Turkey, 2Department of the ISPRM special interest group on sarcopenia Physical Medicine, Rehabilitation and Sports Medicine, and Department of Physiology, University of Puerto Rico, School of Medicine, San Juan, PR, USA, 3Department of Physical and Rehabilitation Medicine, Dr Ayten Bozkaya Spastic Children Hospital and Rehabilitation Center, Bursa, Turkey, 4Physical and Rehabilitation Medicine Unit, Luigi Sacco University Hospital, ASST Fatebenefratelli-Sacco, Milan, Italy, 5Department of Physical and Rehabilitation Medicine, Türkmenbaşı Medical Center Adana, Turkey, 6Department of Physical Medicine and Rehabilitation, National Taiwan University Hospital, Bei-Hu Branch, Taipei, Taiwan, 7Department of Rehabilitation Medicine, University of West Attica, Athens, Greece, 8Department of Physical and Rehabilitation Medicine, Sigmund Freud Private University, Karl Landsteiner Institute of Remobilization and Functional Health, Vienna, Austria, 9Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Gyeonggi, South Korea, 10New England Geriatric Research Education and Clinical Center, VA Boston Healthcare System, Boston, MA, USA, 11Department of Physical Medicine and Rehabilitation, Harvard Medical School, Boston, MA, USA, 12Spaulding Rehabilitation Hospital, Boston, MA, USA and 13Istituti Clinici Scientifici Maugeri, IRCCS, Physical and Rehabilitation Medicine Unit Institute of Tradate, Tradate (VA), Italy. *ISPRM special interest group on sarcopenia
Sarcopenia is an important public health problem, characterized by age-related loss of muscle mass and muscle function. It is a precursor of physical frailty, mobility limitation, and premature death. Muscle loss is mainly due to the loss of type II muscle fibres, and progressive loss of motor neurones is thought to be the primary underlying factor. Anterior thigh muscles undergo atrophy earlier, and the loss of anterior thigh muscle function may therefore be an antecedent finding. The aim of this review is to provide an in-depth (and holistic) neuromusculoskeletal approach to sarcopenia. In addition, under the umbrella of the International Society of Physical and Rehabilitation Medicine (ISPRM), a novel diagnostic algorithm is proposed, developed with the consensus of experts in the special interest group on sarcopenia (ISarcoPRM). The advantages of this algorithm over the others are: special caution concerning disorders related to the renin-angiotensin system at the case finding stage; emphasis on anterior thigh muscle mass and function loss; incorporation of ultrasound for the first time to measure the anterior thigh muscle; and addition of a chair stand test as a power/performance test to assess anterior thigh muscle function. Refining and testing the algorithm remains a priority for future research.
Key words: ultrasound; quadriceps; muscle; Sonographic Thigh Adjustment Ratio; function; frailty; International Society of Physical and Rehabilitation Medicine.
Accepted May 31, 2021; Epub head of print Jun 14, 2021
J Rehabil Med 2021; 53: jrm00209
Correspondence address: Murat Kara, Hacettepe Üniversitesi Tıp Fakültesi Hastaneleri, Zemin Kat FTR AD, Sıhhiye, Ankara, Turkey. E-mail: mkaraftr@yahoo.com
Doi: 10.2340/16501977-2851
Sarcopenia is an important public health problem, characterized by age-related loss of muscle mass and muscle function. The diagnostic recommendations published to date have addressed total or appendicular muscle mass. However, under the umbrella of the International Society of Physical and Rehabilitation Medicine (ISPRM), experts in the special interest group on sarcopenia (ISarcoPRM) developed a new algorithm, based on regional measurements and functional evaluations of the anterior thigh muscle, which is the most commonly and initially affected condition in sarcopenia. Unlike other suggestions, diseases associated with the renin-angiotensin system are emphasized in this algorithm, and ultrasound has been used for measurement of anterior thigh muscle mass.
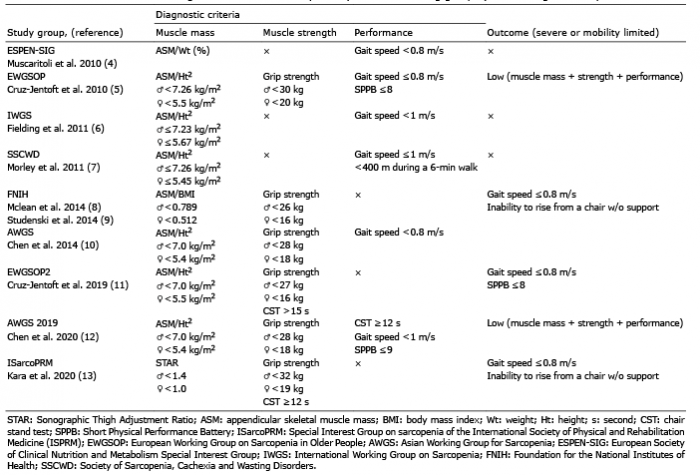
In 1989, Rosenberg first suggested the term “sarcopenia”’ (from the Greek sarx for flesh and penia for loss) to define the age-related loss of muscle mass (1). However, with increasing interest in sarcopenia in the last 2 decades (2), its definition has evolved to “age-related loss of muscle mass and muscle function”. Although sarcopenia was accepted as a disease in the International Classification of Disease – 10th Revision – Clinical Modification in 2016 (3), it still has no universally agreed clinical definition or diagnostic criteria (Table I) (4–13). Of note, the lack of consensus for identifying sarcopenia prevents estimation of the accurate prevalence, prognosis, and effectiveness of interventions. According to various working groups, the prevalence of sarcopenia ranges from approximately 10% to 40% due to different methodology, diagnostic criteria, ethnicity, and selected populations (14).
Table I. Former and ISarcoPRM diagnostic criteria for sarcopenia by different working groups (in chronological order)
Sarcopenia is an important public health problem, since it is a precursor of physical frailty, mobility limitation, and premature death (15). By the eighth decade of life, muscle loss is approximately 30% of peak values, mainly due to loss of and atrophy of type II muscle fibres (16, 17). Age-related loss of muscle mass is thought to be largely due to progressive loss of motor neurones (up to 50% of the motor units) by the eighth decade (18, 19). Therefore, muscle function declines progressively, as the loss of motor neurones is not sufficiently compensated by reinnervation of muscle fibres by the remaining motor neurones (19).
To define muscle loss, appendicular skeletal muscle mass (ASM), measured by dual X-ray absorptiometry (DXA) is generally being used. Analogous to the body mass index (BMI), the ASM is usually divided by height squared, and rarely by weight or BMI. Adjusted values of < 2 standard deviations (SDs) of the healthy young adults are currently considered in the diagnosis (20). Herein, measuring the appendicular (rather than the regional) muscle mass may be misleading, since muscle loss is not uniform throughout the body (21, 22). It is noteworthy that anterior thigh muscles undergo atrophy earlier with ageing, and this issue is paramount for the prevention of impairments and interventions (13, 23–25). Hence, in the earlier stages, the loss of anterior thigh muscle function (e.g. mobility, sitting to standing, climbing stairs) may precede those of the other sites. In addition, assessment of ASM loss may not suffice for prompt interpretation, since normal or even compensatory muscle hypertrophy may develop in the upper limbs, balancing the muscle loss in the anterior thigh (26). As such, subjects may not be diagnosed as sarcopenic, and therefore early rehabilitative interventions might be delayed.
Of particular importance for the present discussion is the fact that physical activity/performance depends on the coordinated integration of the central nervous system (CNS), peripheral nervous and musculoskeletal systems. Herein, for musculoskeletal physicians who focus on activity/mobility limitations and participation restrictions among older adults, it is crucial to understand the biological mechanisms underlying the impairments linked to muscle mass and function. Ever since the term sarcopenia was first defined (1), the eventual muscle dysfunction that is associated with disability, as well as other personal, social, and economic burdens, has been identified as potentially modifiable (27).
Although measurement of muscle mass is advocated as a core component in diagnosing sarcopenia, the clinical definitions of muscle dysfunction (i.e. muscle strength and power) and pertinent outcomes (poor performance or mobility limitation) remain debatable. To clarify a path forward for rehabilitative care providers, the following questions should be answered:
In order to answer these questions, physicians must have sufficient knowledge about age-related functional and structural impairments in the neuromuscular system, and an understanding of the methods and techniques used to evaluate muscle mass, muscle function and physical activity. Furthermore, the fundamentals of neuromotor control and biomechanics must also be known for a better understanding of the role of cognition and muscle mechanics during ADL (Fig. 1). It is also essential to understand the measurement of muscle function and mobility, using muscle strength and physical performance tests, and how these tests are impacted by sarcopenia as well as other important biopsychosocial factors.
Accordingly, the aims of this review article are: to briefly discuss sarcopenia conceptually within the biopsychosocial model of the World Health Organization’s (WHO’s) International Classification of Functioning, Disability and Health (ICF) (28); to review physical activity and pathophysiology of sarcopenia mechanistically from a biomechanical and biologic perspective; and, under the umbrella of the International Society of Physical and Rehabilitation Medicine (ISPRM), to propose a new consensus definition and a novel diagnostic algorithm with the agreement of experts in the special interest group on sarcopenia (ISarcoPRM) (2).
Fig. 1. Skeletal, muscular and nervous systems: a unique anatomo-functional unit. Complex interactions between the neuromotor control by the nervous system, the anatomical/histological features of the muscular and bony tissues, and the continuous feedbacks among them are the keys to generate all the body movements.
The ICF provides standard operational definitions of health and health-related conditions (28). It divides components of health and function into a hierarchically wider perspective of the body (body functions and structures), individual (conduct of functional activities), and society (participation in a life situation or role) (29). While “functioning” is a positive umbrella term encompassing body functions and structures, activities and participation; “disability” includes the negative umbrella term for impairments (of body functions and structures), limitations (on activity) and restrictions (to participation) that may occur in the presence of a health condition. With ageing, impairments of multiple body structures and functions (e.g. neuromusculoskeletal, cardiovascular, respiratory, metabolic, mental, sensory) lead to activity/mobility limitation and participation restriction. Importantly, disability resulting from these multiple body system deficits can further compromise muscle function and physical activity (30) in addition to causing adverse health outcomes and mortality (31, 32).
On the other hand, physical activity is a powerful factor in the prevention and treatment of many health conditions in older adults (33). Physical functioning is a multidimensional concept including mobility (lower extremity function), dexterity (upper extremity function), axial ability, and ability to perform instrumental ADL (34). Mobility is defined as body movement in ADL, with subdomains of rolling over, sitting, standing, and walking (28). It can usually be measured objectively with physical performance tests. Physical performance represents the product of integration of specific body systems that collectively contribute to complex activities (i.e. short/long distance walking, chair standing, stair climbing), and is impacted by behavioural (self-efficacy, motivation, social engagement etc.) as well as other health-related factors (e.g. pain, fatigue) (29).
According to the ICF of the WHO, body structures are anatomical parts of the body, such as organs, limbs and their components, and impairments are problems in body function or structure as a significant deviation or loss. In this regard, the authors have reported some cut-off values (significant deviation from the healthy young adult population) to diagnose the loss of muscle mass and muscle function, i.e. to confirm sarcopenia. Since the anterior thigh is the most commonly and initially involved compartment affected in ageing, measuring its muscle mass and function could provide more prompt information about sarcopenia (i.e. an impairment in body structure/function). Sarcopenic patients have significant neural and muscular impairments, leading to performance problems and activity/mobility limitations in ADL, which can also be associated with many comorbid diseases.
The capacity of a muscle to generate energy is related to its functional parameters (i.e. excursion, force, contraction velocity, and fatigability), which, in turn, correlate with their structural and architectural properties, i.e. fibre type and length, physiological cross-sectional area (pCSA) and pennation angle (35). While muscle excursion is directly proportional to the length of the muscle fibre (or fascicle), it is inversely proportional to the pennation angle. Muscle actions can be classified into isometric, dynamic concentric or eccentric types. The magnitude of the force produced by a muscle is proportional to its pCSA during isometric contractions, and to pCSA and fascicle length during dynamic contractions. Contraction velocity is related to the fibre length/type composition, as well as to the viscoelastic properties of the muscle-tendon unit. Muscles with longer fibres and a higher ratio of type II to type I fibres contract faster than the others. Fatigability of a muscle is also determined by its fibre type and oxidative capacity (35).
At the joint level, forces cause a rotational effect, which is the product of net force and moment arm. The amount of rotational motion around the joint is proportional to muscle excursion and the moment arm of the muscles. Total energy during a motion is defined as work. Muscles producing greater excursion and force can produce more energy and work (36, 37). Total work done by a task-specific group of muscles is calculated as the change in the body’s energy, which can be estimated by subtracting the potential energy of the stationary body at the beginning and end of motion (38).
Another parameter is contraction velocity, which is related to the fibre length and type composition. Muscles rich in type II fibres and with long fascicles contract faster than the others. Likewise, even with the same CSA, they can also move the body segments faster (35). Hereby, understanding the advantage of higher velocity for some physical activities would be the main concern. Work (W) is defined as the product of force (F) and displacement (X), and the amount of work per time (W/t) or the product of velocity (V) and force (F×V) is known as “power”. Similarly, another important parameter would be “muscle endurance function”, which is defined as the capability of maintaining a certain level of force over time. It is directly related to the type of muscle fibres and their aerobic capacity (35). Easily fatigued muscles cannot maintain a required force or physical activity as well as muscles resistant to fatigue. Therefore, power-generating capacity and fatigability of task-specific muscles determine the ability to perform a variety of physical activities and the time duration in which that particular activity can be performed (39).
In addition to the above discussion of skeletal muscles, physical activity is also under the strict control of the CNS. The CNS regulates the activation of muscle groups and complex tasks processed in a manner that is well-timed, smooth, and efficient with respect to the intended goal. For example, executive brain functions, also including a set of cognitive processes, are essential to plan, initiate, execute and monitor goal-directed movements and behaviour (40). In other words, age-related nervous system impairments can cause an activity limitation by affecting the optimal activation, function and energy generating capacity of muscles (41). Overall, when evaluating older adults for sarcopenia, a detailed knowledge of the neuromotor control patterns in normal and pathological conditions is crucial. In particular, this is necessary for the correct administration and interpretation of power and performance tests, as well as for optimal exercise prescription to increase strength, power, endurance, flexibility and coordination (42, 43).
Skeletal muscle is the largest organ in the body, comprising approximately 40% of total body weight. The preservation of muscle mass is determined by the balance between the rates of protein synthesis and proteolysis. Some of the negative regulators of muscle mass include endosome-lysosome, Ca2+-dependent, caspase-dependent, ubiquitin/proteasome-dependent. Positive regulators, on the other hand, include growth hormone, insulin-like growth factor 1 (IGF-1), insulin, and testosterone (44). With ageing, a disruption of the balance between the anabolic and catabolic processes leads to loss of muscle mass and function, i.e. sarcopenia (45). Multiple factors are associated with the development of sarcopenia, including genetic predisposition, inactivity, age-related increase in proinflammatory cytokines (e.g. interleukin 1 and interleukin 6), malnutrition, reductions in hormones (e.g. oestrogens, androgens, growth hormone, and vitamin D), mitochondrial dysfunction, metabolic disorders, insulin resistance and lipodystrophy (46). In addition, new and increasing evidence also shows overactivity of the renin-angiotensin system (RAS) in the pathogenesis of obesity, insulin resistance and several other conditions contributing to skeletal muscle atrophy (47).
Molecular, cellular and hormonal factors
One of the most important regulators of protein synthesis is the level of insulin/IGF-1, which modulates the phosphatidylinositol-3-kinases/Akt/mammalian target of rapamycin pathway. Activation of this pathway stimulates protein synthesis and inhibits proteolysis via the suppression of forkhead box O (FOXO) transcription factors, which control the expression of atrophy-related genes (48). Growth hormone affects the muscle via IGF-1 synthesis and suppression of cytokine signalling 3 expression (49). Testosterone increases intracellular Ca2+ concentration and increases IGF-1 expression leading to muscle fibre growth (50).
Previous studies demonstrate that muscle atrophy can develop due to the activation of protein degradation by both the ubiquitin-proteasome system and autophagy (48). The activation of FOXO3 alone is enough to trigger proteolysis via the ubiquitin-proteasome system and autophagy, and several other transcription factors, including glucocorticoid receptors and nuclear factor kappa B, are important in causing muscle atrophy. Therefore, their inhibition can decrease or block the muscle atrophy (45, 51). In addition, members of the transforming growth factor-beta (TGF-β) family suppress myogenic differentiation. Among these, myostatin (produced by skeletal myocytes) inhibits the mammalian target of rapamycin pathway and activates FOXO1-related muscle atrophy, which primarily affects fast-twitch (type II) fibres (45, 51).
All of these cellular and molecular mechanisms together cause a reduction in muscle size (especially of type II fibres) and a type II to type I fibre shift (51). Although it is assumed that type I fibres are protected from atrophy by the peroxisome proliferator-activated receptor-gamma coactivator 1-α (52), it has been reported that the number of type I fibres in pectoralis minor muscle decreased after 60 years of age. However, the size of type I fibres was increased (compensatory hypertrophy), maintaining the total volume of type I fibres with ageing (53). Type II fibres are negatively affected by TGF-β and nuclear factor kappa B. Moreover, loss of mitochondria due to damage, apoptosis and turnover disruption reduces their quantity and quality with ageing (52). Ultimately, these changes lead to the decline of intrinsic force-generating capacity (maximal strength and power) and increase in fatigability of skeletal muscles (46). In addition to the altered myofibre metabolism; mitochondrial dysfunction, adipocyte infiltration, and altered satellite cell properties (reduction in their number and/or activation) are seen, especially in type II fibres (54). Thus, the regenerative capacity of old muscles is also decreased.
Renin-angiotensin system
The RAS has an important role in the regulation of various biological functions, including skeletal muscle metabolism. In recent years, however, more attention has been focused on the non-classical pathway, which acts contrary to the classical pathway with regards to the peripheral blood flow, insulin resistance, and skeletal muscle metabolism (55). In classical RAS axis-related disorders, loss of muscle mass and function can be seen. For instance, hypertension was found to be correlated with slow gait speed at baseline and higher annual decline after a 2-year follow-up (56). A cross-sectional study (n = 2431) has found that angiotensin-converting enzyme inhibitor (ACEI) users have larger lower limb muscle mass (57). Another 3-year longitudinal study has shown that continuous use of ACEIs plays a preventive role in the decline of knee extension strength and gait speed (58).
The classical RAS overactivity was recently identified as an important contributor to the pathogenesis of sarcopenia (51, 55). Angiotensinogen is produced in the liver and then converted to angiotensin I (Ang I) by renin. Thereafter, Ang I is transformed into Ang II by ACE. Ang II binds to its receptors and causes insulin resistance, and muscle atrophy and fibrosis. On the other hand, in the non-classical pathway, Ang (1–7) is synthesized from Ang I and/or Ang II by ACE2 and neutral endopeptidase, respectively. Ang (1–7) acts via the Mas receptor, and ACE2 and the Ang (1–7)/Mas receptor interaction are negative modulators for the classical pathway (55). When the classical pathway is activated, there is increased accumulation of intracellular reactive oxygen species (and protein degradation (via activation of major proteolytic systems including ubiquitin-proteasome system, caspase-3, calpain), and inhibition of IGF-1 signalling and downregulation of protein synthesis. These changes result in myonuclear apoptosis, mitochondrial dysfunction, and enhancement of the oxidative stress with eventual muscle atrophy (55, 59). Conversely, if the non-classical pathway is activated, protein synthesis is enhanced, and apoptosis and protein degradation are inhibited with the predominance of anabolic mechanisms (55, 59).
Skeletal muscle fibrosis is another pathological condition, which can be seen after injury, with ageing, and in conditions such as myopathies. The classical RAS pathway induces fibrosis by increasing the extracellular matrix proteins, enhancing TGF-β, and producing connective tissue growth factor. On the other hand, in the non-classical pathway, Ang (1–7) acts as an antagonist to Ang II and exerts an antifibrotic effect (55, 60). Finally, skeletal muscles play an important role in the regulation of blood glucose by modulating insulin resistance. While the classical pathway increases activation of reactive oxygen species and decreases Glut-4 transportation, the non-classical pathway increases insulin sensitivity (55).
The RAS overactivity is reported to contribute to the pathogenesis of Alzheimer’s disease, where activation of brain Ang II adversely affects cognitive function (61). The increase in ACE activity and Ang II levels causes vasoconstriction, accumulation of amyloid-β and tau, and a reduction in the acetylcholine release, which are related to dementia (62). In addition, Ang II levels are found to be associated with smaller cortical and hippocampal volumes (62). Moreover, RAS inhibition attenuates cognitive impairment through the reduction of amyloid deposition (63). Herewith, improving cognitive function by inhibiting RAS overactivity in clinical practice is controversial (64).
In light of the aforementioned data, it is paramount to consider RAS-related disorders (Table SI) (65–79) in the diagnosis and management of sarcopenia (80). The association between sarcopenia and hypertension also needs to be better understood (81). Among 99 variables, age, systolic arterial hypertension, mini-nutritional assessment, number of chronic diseases, and blood sodium level were found to be independent determinants of sarcopenia (82). A recent systematic review and meta-analysis demonstrates that the presence of hypertension is more common in sarcopenic than non-sarcopenic patients (odds ratio (OR) 1.29 (95% confidence interval (95% CI) 1.00–1.67)) (83). In addition, a cross-sectional preliminary study by Ata et al. (84) found that the presence of hypertension seemed to independently predict the risk of sarcopenia in older adults (OR 6.5 (95% CI: 2.4–17.8)); and that among many antihypertensive drugs, ACEIs seemed to have favourable effects on both hypertension and sarcopenia. Hypertension is thought to affect the skeletal muscles directly and also via its impact on neuromotor control and cognition (85). To this end, RAS overactivity appears to be important in the pathogenesis of sarcopenia (86).
Similarly, sarcopenia together with obesity (i.e. sarcopenic obesity) has more deleterious effects, not only on body composition, but also on cardiovascular morbidities, as well as in other physiological systems. In this sense, it has been reported that obesity and sarcopenia act synergistically to increase the risk of disability (87). Needless to say, body size affects the measurements of sarcopenia, and obese subjects undoubtedly need powerful anterior thigh muscles to carry their extra weight, especially during chair standing and climbing stairs.
The definition and diagnostic evaluation of sarcopenia continue to be a topic of discussion. Although working groups generally suggest adjusted ASM measurements of muscle mass by DXA, ISarcoPRM suggests the potential benefits of a new approach using adjusted anterior thigh muscle measurements (instead of ASM) for early assessment and prompt diagnosis of low muscle mass and confirmation of sarcopenia (Table I). Furthermore, debates exist on whether poor performance on functional tests (i.e. mobility limitation) should be included as a part of sarcopenia diagnosis or rather as clinically relevant outcome. It has been suggested that gait speed ≤0.8 m/s or inability to rise from a chair without support should be a primary outcome (i.e. mobility limitation), not part of the diagnostic criteria (9). This outcome was used as validation to determine the cut-off point values for grip strength, and identified low and intermediate cut-off points as 26 vs 16 kg with a mobility limitation of 40% vs 51%, and 32 vs 20 kg with a mobility limitation of 21% vs 36% in males and females, respectively.
Recently, the European Working Group on Sarcopenia in Older People (EWGSOP2) (11) also used poor mobility performance as a measure of severity, and, in contrast to their original recommendation, they lowered grip strength cut-off values from 2 SD (30 vs 20 kg) (5) to 2.5 SD (27 vs 16 kg) in males and females, respectively. Although we agree with both groups that mobility limitation should be considered as a measure of outcome/severity; we believe that cut-off values for grip strength should be determined consistently i.e. as 2 SD, similar to muscle mass measurements (Table II) (9, 13, 43, 88–99). Otherwise, using stringent cut-off values for a more “conservative” diagnosis (with high specificity, but low sensitivity) can inevitably result in missing the diagnosis in “real” sarcopenic patients, who should be managed earlier in the course of their care.
A variety of screening tests are proposed for sarcopenia, which is diagnosed according to ASM measurements (11, 12, 100, 101). Case finding may start when a patient reports symptoms or signs of sarcopenia (i.e. falling, weakness, slow gait speed, difficulty rising from a chair or climbing stairs). In such cases, further testing (i.e. measure of calf circumference and/or a self-reported SARC-F questionnaire (Strength, Assistance with walking, Rise from a chair, Climb stairs, and Falls) has been suggested (100). However, characterized by low-to-moderate sensitivity and high specificity, these tests will mostly detect severe and late cases with mobility limitation, for whom earlier treatment may be effective (11, 12). Therefore, in order to better identify sarcopenic patients in an earlier and more reversible period, ISarcoPRM suggests screening all older adults and adults who have chronic comorbid diseases, such as obesity, metabolic syndrome, and RAS-related disorders (Table SI), including uncontrolled hypertension or those using antihypertensive drugs (other than ACEI) (57, 58). In this regard, chair stand test (CST) and grip strength may be simple and useful tools for screening sarcopenia (102).
It is not clear that age-related muscle loss can be detected accurately with DXA (103). Longitudinal studies have shown that muscle strength and performance tests predict adverse outcomes (falls, mobility limitation, hip fractures, and mortality) and that DXA has no additional value (104–106). Authors have suggested alternative technologies to measure muscle mass (105). Herein, we strongly believe that the lack of predictive value of DXA results regarding the clinical outcome can be attributed to the fact that age-related muscle loss is more evident in the anterior thigh than in the other muscles in general. In other words, not taking the regional muscle measurements into account would result in inaccuracy (13, 19).
The anterior thigh muscles, which are fundamental to mobility skills, are more commonly and severely affected in sarcopenia. Frontera et al. (107) found a 24–30% loss in knee extensor strength and 16% loss in quadriceps muscle (CSA) over a 12-year duration. Another 5-year longitudinal study in older adults (n = 1,678) revealed approximately 15% loss of knee extensor strength and approximately 4% loss of thigh muscle CSA, whereby the decrease in muscle strength was 2–5 times greater than the loss of muscle CSA (108). In addition, calf and thigh muscle CSA (but not muscle mass measured by DXA) were found to be correlated with poor outcomes (i.e. mobility limitation and mortality, respectively) (109, 110). Moreover, recent cross-sectional studies report that muscle power/strength and performance tests are better correlated with anterior thigh muscle measurements (CSA and thickness) than total muscle mass measurements (13, 111).
Anterior thigh muscle measurements (i.e. volume, CSA, or thickness) may be more valuable than ASM in the (early) diagnosis of sarcopenia (112). Herein, although MRI and CT may be better than US for regional measurements; both techniques are not feasible for widespread clinical practice. In contrast, US measurements can be an easy, quick, safe, portable alternative that is valid (intraclass correlation coefficient (ICC) 0.92–0.99) and reliable (ICC 0.88–0.97), especially for measuring anterior thigh muscle thickness (113, 114).
A cross-sectional study of 1,030 subjects aged 20–102 years evaluated grip strength, knee extension strength, leg extension power, and calf muscle CSA, and reported that the gradient of decline during ageing was highest for power, moderate for strength, and less evident for muscle CSA (115). For instance, compared with subjects in their 20s, leg extension power of individuals aged >85 years was lower by 75%, strength by 40–50%, and muscle CSA by only 20%. It is also important to note the significant dissociation between muscle CSA and its function with ageing, which is related to CNS and muscle fibre specific changes. Besides the age-related motor unit loss, fast-to-slow muscle fibre shift, and fibre atrophy (largely due to progressive loss of motoneurones and muscle fibres). Qualitative changes at the muscle fibre level and loss of contractile proteins may also have significant effects on muscle function (19). Although leg strength is strongly correlated with leg power (r = 0.89), leg power had more impact than leg strength on all physical performance tests (115). In fact, using a curvilinear model, leg power generally predicted up to 50% of the variance in performance tests including habitual gait speed (29%), stair climb time (37%) and maximal gait speed (50%) (116). Therefore, given the early decline in leg power with ageing, lower extremity strength/power tests (e.g. CST, stair climb test or maximal gait speed) can be used to identify an impaired muscle function at an early period.
Muscle strength and performance tests have higher correlations with morbidity and mortality than muscle mass measurements (117). This is particularly true for the commonly used tests, such as grip strength, CST, and gait speed (105). Grip strength is a simple, easy, and inexpensive screening tool, and a powerful predictor of future morbidity and mortality in young, middle-aged and older adults (118). Although it is useful for screening sarcopenia, grip strength alone (i.e. without CST) can misclassify individuals, as it explains approximately 40% of the variance in lower extremity muscle strength (119). Herewith, evaluating the lower extremity muscle strength is critical, as it is a superior and more convenient indicator of balance, walking, and other mobility-based activities. In addition, subjects with weak lower limb muscles tend to compensate for their ADL performance by using upper limb and trunk muscles, which may help maintain their upper limb muscle mass and strength. In this context, measuring and maintaining the anterior thigh muscle strength would be the primary target to preserve mobility (120). As the lower limb muscle strength is reduced earlier (and to a larger extent) than the upper limb muscle strength (21), tools such as CST and/or stair climb test seem to be a suitable proxy for evaluating the lower limb function as well as strength/power in ageing adults.
The ability to stand up from a sitting position is critical for functional independence and quality of life in general. Rising from a seated position is one of the difficult physical activities in daily life, as it requires movement of body weight against gravity. Loss of muscle mass and function will impact this transfer more than walking. The CST measures the time for an individual to stand up and sit down as quickly as possible 5 times, starting from a seated position without using the arms. As it requires strength and power, it can be a convenient test for mobility. Of note, muscle power is the most reliable measure of muscle function, and is more strongly related to performance than is strength in older adults (38). Furthermore, with ageing, power declines at a faster rate than strength (121). Therefore, a strength/power test, such as CST, seems to be useful for early recognition of sarcopenia.
Although several authors used CST to assess muscle strength, it is actually an integrative task reliant on muscle power and influenced by multiple physiological and psychological processes. It is a specific task rather than a proxy measure of lower limb muscle strength (122). Age-related decline in muscle mass and function can contribute to the loss of ability to rise from a seated position. However, lower limb muscle strength loss is not the only modifier of CST performance in older adults, as it is evident from the fact that lower limb strength parameters explain only half of the variance of CST (123). Leg speed, leg power, endurance, posture, the presence of pain, and psychological factors may also explain the variability in the performance of CST (123).
The Short Physical Performance Battery (SPPB), a valid and reliable measure of lower extremity function, is predictive for disability and mortality (124). It is a composite score (0–12) of gait speed, standing balance, and CST. While higher scores indicate better mobility, a total SPPB score ≤ 9 indicates limited mobility (124). Of the 3 SPPB components, the steepest gradient of risk for disability is seen for gait speed (125, 126). As gait speed alone is easy to measure and nearly as good a predictor of disability outcomes as the full battery (30), it may be clinically expedient to focus on gait speed alone. Several authors have suggested that gait speed > 1.0 m/s is related to healthier ageing, and < 0.6 m/s increases the likelihood of poor health and function (127). Others have advocated a more inclusive cut-point value of ≤ 0.8 m/s to define mobility limitation (Table II). Interestingly, older adults with multiple chronic conditions ranked maintaining independence as the most important health-related outcome (76%), followed by staying alive (11%), pain relief (7%) and symptom relief (6%) (128).
It is important to note that performance tests are done with proper stabilization and movements of the body parts around the joints where skeletal muscles are the main producers of forces required to achieve those functional tasks. The magnitude and temporal parameters of forces are initiated and controlled by the CNS. This is why we argued that age-related CNS (including cognitive) dysfunction has significant negative effects on the force-generating capacity of skeletal muscles and the performance of motor or mobility tests (2). Also, there is considerable evidence identifying a relationship between physical and cognitive impairments in older adults (129–133). A recent meta-analysis showed positive and moderate correlations between decrease in grip strength and decline in cognitive function (129). Furthermore, longitudinal studies reported that low grip strength and slow gait speed values at baseline predict future cognitive impairments (132, 133). Brain changes concerning the age-related cognitive impairment include white matter hyperintensity, shrinking of the hippocampus, smaller cortical surface area, more cortical thinning, and inadequate motor coordination (134).
Table II. Commonly used and suggested cut-off values in the diagnosis of sarcopenia by different working groups
As anterior thigh muscles are involved early with ageing, using cut-off values for anterior thigh muscle measurements could provide more prompt information about muscle loss, i.e. an impairment in body structure. A well-known example of this approach is the measurement of bone mineral density (BMD) at regional sites (e.g. femoral neck and spine) for the diagnosis and definition of osteoporosis. As hip BMD is the most reliable parameter for hip fracture risk, and as spinal BMD should be used for monitoring the treatment of osteoporosis (135), femoral neck and/or spine BMD values ≤ 2.5 SD of the mean of young adult population is taken into consideration for the diagnosis of osteoporosis. Making an analogy for sarcopenia, as lower extremity function (i.e. mobility) is important for adverse outcomes in the elderly, and as anterior thigh muscle is more severely and preferentially affected with ageing, knee extensor strength testing together with anterior thigh muscle measurements could be used for accurate diagnosis of sarcopenia (13, 136–138). Likewise, a significant loss of muscle mass and muscle strength (i.e. < 2 SD of the mean of young adult population) should be used concerning the diagnosis of sarcopenia. However, such an approach is currently not included in any of the ongoing consensus or discussions for sarcopenia.
Some studies have used anterior thigh muscle thickness, or anterior to posterior ratio to detect the loss of anterior thigh muscle (112). However, muscle measurements of a subject differ according to age, sex, weight and height. Therefore, adjusted regional muscle mass measurements should be used. In this regard, thigh muscle CSA has been adjusted by body weight, since it has a higher correlation with body weight (r = 0.73 in males, r = 0.66 in females) than height (r = 0.32, r = 0.21, respectively) (139). In addition, sarcopenia is defined as the ratio of thigh muscle CSA/body weight being < 2 SD values of the young population (Table II) (88). Although it seems reasonable, as stated above, the use of whole (not only anterior) thigh muscle CSA may lead to misinterpretation as anterior thigh muscles are affected more severely.
We propose adjusting anterior thigh muscle thickness for BMI because of the correlation between these 2 variables in healthy young adults (r = 0.500 in males, r = 0.447 in females). This adjustment using BMI and a Sonographic Thigh Adjustment Ratio (STAR) is already suggested for the diagnosis of sarcopenia (Table II) (13). Another commonly used muscle for the evaluation and diagnosis of sarcopenia is the psoas major (140). Its CSA was found to be positively correlated with weight (r = 0.365) (141). However, it is commonly, and in our opinion erroneously, adjusted by height squared and values < 2 SD of the healthy young adults were considered as low muscle mass (142, 143).
We also suggest that grip strength cut-off values should be < 2 SD of a healthy young population. Different cut-off values for CST, predicting a gait speed of < 0.8 or < 1 m/s, have also been reported (Table I). Different cut-off values have also been published as regards timed up and go test, gait speed, SPPB and 400-m walk test, as shown in Table II. All of these tests can be performed in clinical practice to predict sarcopenia-related adverse outcomes. Herewith, while the SPPB and 400-m walk tests predict mortality (98), due to their long duration or requirement for extra space (e.g. corridor longer than 20 m), these tests are more often used in research than in daily clinical practice.
Finally, although ISarcoPRM recommends certain cut-off values (especially for STAR), it will undoubtedly be more appropriate to use validated cut-off values once different countries establish their national normative data together with the relevant predictive values for morbidity and mortality, which is a high priority for future longitudinal research.
The ISarcoPRM suggests screening all older adults and adults with RAS-related disorders. To identify low muscle function, ISarcoPRM proposes the use of ≥ 12 s for CST, and < 32 kg (males) and < 19 kg (females) for grip strength as the relevant cut-off values (Table II) (Fig. 2). Once low muscle function (assessed by CST or grip strength) is detected, with the diagnosis of “probable sarcopenia”, we suggest using STAR to explore significant loss of muscle mass (< 1.0 for females and
If the person has normal STAR values (i.e. muscle strength or function loss alone), the scenario can be defined as “dynapenia”, and other causes affecting the neuromotor control (e.g. cognitive impairment, polyneuropathy, movement/balance disorder, depression) should be investigated (119). Lastly, ISarcoPRM suggests to define “’severe sarcopenia” in the presence of a mobility limitation, i.e. gait speed ≤ 0.8m/s and/or inability to rise from a chair without support (9). Needless to say, these older subjects are prone to eventually develop decline in physical and cognitive functioning, as such multidisciplinary diagnostic/therapeutic management would always remain as the prerequisite.
The differences between this proposed algorithm and others are:
Herein, several limitations must be acknowledged. This is a conceptual model that is supported by scientific evidence, but that has not been tested in the research laboratory or in the clinic. Therefore, it is important to conduct more research about the individual components of the algorithm and to validate the proposed approach. The presence of other health conditions must be evaluated, and the application of the model to persons with some comorbidities (e.g. knee surgery, peripheral nerve injury or severe arthritis) must be done with caution. The presence of any of these conditions may result in regional loss of muscle mass and concomitant muscle dysfunction. It may be possible to use the contralateral anterior thigh or psoas muscle measurements in such clinical scenarios. Another limitation is related to the lack of access or insufficient training to perform optimal ultrasonographic muscle mass measurements.
Fig. 2. ISarcoPRM diagnostic algorithm for sarcopenia. ISarcoPRM suggests to screen all older adults and adults with renin-angiotensin system (RAS)-related disorders by using ≥ 12 s for chair stand test (CST), and < 32 kg (males) and < 19 kg (females) for grip strength, < 1.0 (females) and < 1.4 (males) for sonographic anterior thigh ratio (Sonographic Thigh Adjustment Ratio; STAR) values. In the presence of sarcopenia, gait speed ≤0.8m/s and/or inability to rise from a chair without support is diagnosed as “severe sarcopenia”. *If any of the 2 tests (initially performed) is normal, it is suggested that the other test should be performed as well. If any of the 2 tests (initially performed) is abnormal, it is sufficient to proceed in the “low” direction. £Cognitive impairment, polyneuropathies, movement/balance disorders, depression or motivational problems etc. B: bone; M: muscle; F; subcutaneous fat tissue.
An important aim of our proposal is to promote further discussion about the evaluation and diagnosis of sarcopenia from a point of view that fits better in a musculoskeletal/rehabilitation medicine perspective. It is important to better understand the relationship between sarcopenia and function. The proposed novel framework has scientific support in the literature, but immediately suggests several lines of research. A sound and comprehensive algorithm will help us to define the incidence and prevalence of this condition. The study of RAS-related disorders can contribute to a better understanding of the basic pathogenesis of sarcopenia. Refining and testing the algorithm for its applicability as a tool to monitor progress and changes over time is also a priority for future research. In addition, the development of therapeutic and rehabilitative interventions, based on the pathophysiology discussed above, is required.
The authors have no conflict of interests to declare.


 Click to show fullsize
Click to show fullsize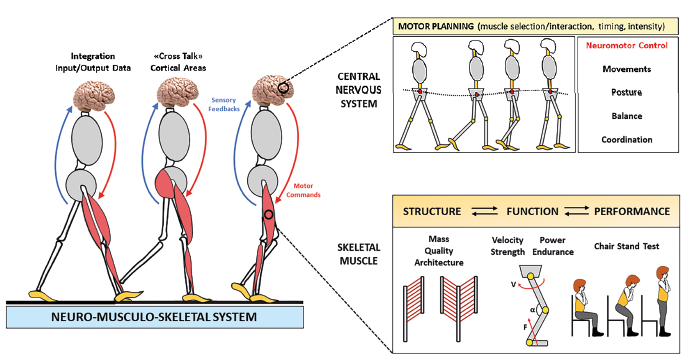 Click to show fullsize
Click to show fullsize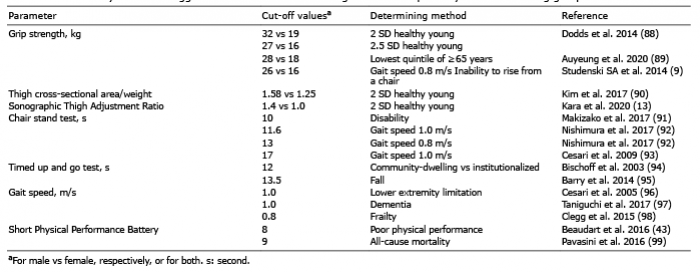 Click to show fullsize
Click to show fullsize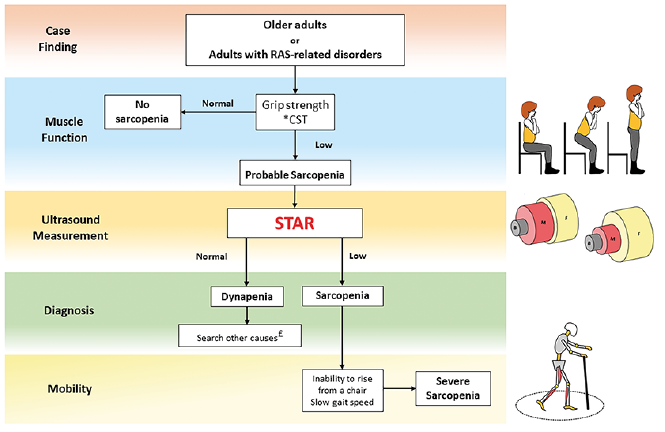 Click to show fullsize
Click to show fullsize