
From the 1Department of Physical Medicine and Rehabilitation, Geriatric Health Services Facility, Caretown Yuyu, Medical Corporation Meikeikai, Saitama, 2Department of Rehabilitation Medicine, Tokyo Medical and Dental University Graduate School, Tokyo, 3Faculty of Symbiotic Systems Science, Fukushima University, Fukushima, 4Graduate School of Health and Social Services, Saitama Prefectural University, Saitama, 5Faculty of Health Science, Juntendo University, Tokyo and 6Department of Orthopaedic Surgery, Dokkyo Medical University Saitama Medical Center, Saitama, Japan
Objectives: To determine whether individual measurements of the centre of pressure for the stance and stepping legs can reveal new characteristics of reduced anticipatory postural adjustments during gait initiation in post-stroke hemiplegic patients.
Methods: Subjects included 30 stroke patients and 10 healthy age-matched controls. The acceleration of the trunk, and the centre of pressure of each leg, were measured during gait initiation, 3 times each with the paretic and non-paretic legs leading. Anticipatory postural adjustments were characterized using trunk acceleration and centre of pressure displacement data.
Results: Latency of the posterior displacement peak of the paretic leg centre of pressure with either the paretic or non-paretic leg leading was significantly longer in stroke patients compared with controls, and was also longer than that of the non-paretic leg. The magnitude of the posterior displacement peak of the paretic leg centre of pressure was smaller than that of the non-paretic leg. Peak latency of the paretic stepping leg centre of pressure correlated with the clinical measures of motor dysfunction, postural balance, and gait ability.
Conclusion: Measurements of the latency and magnitude of centre of pressure displacement peak individually for the paretic and non-paretic legs can help elucidate the mechanism behind reduced anticipatory postural adjustments. This information will be useful in designing new treatment strategies for stroke patients.
Key words: postural control; balance; posture; kinematics; gait.
Accepted Jun 10, 2021; Epub ahead of print Jun 23, 2021
J Rehabil Med 2021; 53: jrm00211
Correspondence address: Tetsuya Jinno, Department of Orthopaedic Surgery, Dokkyo Medical University Saitama Medical Center, Saitama, Japan. E-mail: jinnot@dokkyomed.ac.jp
Doi: 10.2340/16501977-2856
Measuring the centre of pressure individually for the stance and stepping legs can reveal what happens during initiation of gait in stroke patients. The latency and magnitude of the centre of pressure displacement peak showed characteristic differences between stroke patients and control subjects, and between paretic and non-paretic legs. The peak latency of the paretic stepping leg centre of pressure correlated significantly with clinical measures of motor dysfunction, postural balance, and gait ability. These findings may contribute to the development of effective rehabilitation exercises for stroke patients.
B
alance control during gait initiation is crucial for starting stable gait, both in healthy individuals and in people with neuromuscular limitations (1, 2). Motion analyses of electromyograms, accelerations, and ground reaction forces during gait initiation can provide important clinical information for understanding the balance control mechanism. In post-stroke hemiplegic patients, sensory and motor impairments often make good balance control challenging (3–6). In particular, spasticity interferes not only with balance and gait, but also leads to suppression of the soleus muscle, which is required for gait initiation, and makes initiation of gait more difficult (4, 7, 8). The basic problems include motion asymmetry and unstable weight shift to the stance side during gait initiation. The unstable gait initiation is thought to be due to hypometric anticipatory postural adjustments (APAs) (8–10).
APAs are changes in posture prior to voluntary movement, which contribute to postural adjustments during gait initiation (11). Gait initiation APAs include activation of the tibialis anterior and suppression of the soleus prior to the start of movement (12, 13), along with posterior shift of the centre of pressure (COP) (14, 15). APAs might account for the time required for the combined COP, i.e. the mean COP of both legs, to shift from the centre of both soles to the posterior part of the stepping leg and then to the posterior part of the stance leg (16). APA occurs in the postural phase, and some reports have determined COP changes until heel-off of the stepping leg (17), while other reports have used COP changes until foot-off as the end of the APA period (16). Lateral and posterior shifts of the combined COP, which are typical measures of APAs during gait initiation, are known to be smaller in stroke patients (3, 10). Furthermore, in stroke patients, inactivation of the tibialis anterior on the paretic side, prolonged latent suppression of the soleus, and smaller shifts of the combined COP indicate reduced APA function (3, 8).
To the best of our knowledge, there are no detailed reports of the relationship between reduced APA function and the COP of the stance and stepping legs or of the paretic and non-paretic legs during gait initiation in stroke patients. Assessing COP in each leg individually might provide a better understanding of reduced APAs in stroke patients, with a view to devising better treatments while noting that asymmetry between the stance and stepping legs during gait initiation, and non-uniformity in the vertical component of the ground reaction force have been reported in healthy adults and elderly people (18, 19). Therefore, in post-stroke hemiplegic patients also, it is necessary to look for the details of reduced APA in individual COPs. The latency of muscle activity is important in assessing APA, and has been reported in many studies (17). On the other hand, when assessing APA, changes on each side in individual COPs remain unclear. Investigating factors in the reduced APAs with a focus on individual COPs is thus important in obtaining clinical treatment suggestions for post-stroke hemiplegic patients. The stabilometers used to assess individual COPs are compact and inexpensive, and are widely used even in clinical practice to quantify posture and balance. Electromyograms are often used to analyse APAs (8, 20), but accelerometers and stabilometers are also coming into widespread use because of the low burden on the patient and the simplicity of clinical measurements (10, 21).
The aim of the current study was therefore to investigate whether individual COPs show new characteristics of reduced APAs in post-stroke hemiplegic patients. The initial hypothesis was that the peak latency and the peak magnitude of displacement in individual COPs, as characteristics of the reduced APAs in post-stroke hemiplegic patients, are asymmetrically prolonged and decreased, respectively. The second hypothesis was that the characteristic changes in individual COPs are associated with motor impairments, balance indices, and gait ability in post-stroke hemiplegic patients.
Subjects
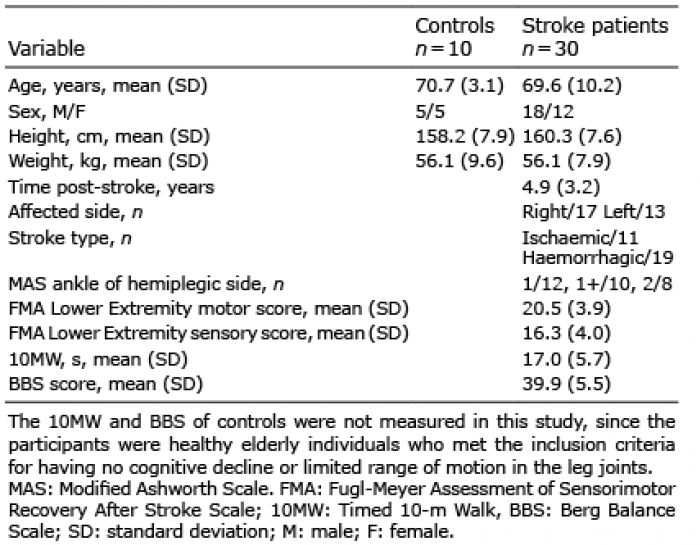
The study and control groups comprised 30 chronic post-stroke hemiplegic patients (17 right-sided, 13 left-sided) and 10 healthy aged-matched participants, respectively, with the characteristics shown in Table I. All of the subjects were capable of walking unassisted, with a score of at least 23 points on the Mini-Mental State Examination (MMSE) (22, 23), and were free of marked limitation in the range of motion of the leg joints. People excluded from the study were those with motor dysfunction not induced by stroke, severe higher-brain dysfunction that prevented comprehension of the study task, or visual disorders that could affect the study (13, 24). Participants were excluded if they presented with bilaterally affected legs, previous lower leg surgery or injuries, or any other neurological, musculoskeletal, or psychiatric conditions that could affect balance control (10). Specifically, individuals who had difficulty touching the sole of the foot to the ground from the beginning due to contracture of the ankle joint, or who had unilateral spatial neglect, were excluded.
The Research Ethics Committee of Tokyo Medical and Dental University Graduate School approved the study protocol (M2018-081). Written consent was obtained from all of the subjects after fully informing them in writing and orally about the study.
Table I. Basic participant information (n = 40)
Procedures
The equipment used included accelerometers (myoMOTION, Noraxon USA Inc., Scottsdale, IL, USA) with a sampling frequency of 1,500 Hz placed on the neck (C7), lower back (L3), and pelvis (S1), a stabilometer (UJK-200C, Unimec Co., Ltd, Tokyo, Japan) consisting of 2 measurement plates with a sampling frequency of 100 Hz for recording COP displacement and a simple light-emitting signalling device (Direction Indicator, Irisco Co., Ltd, Saitama, Japan) placed 5 m in front of the stabilometer, which displayed left and right arrows randomly (25, 26). Acceleration was processed with a 3-Hz cut-off, zero phase shift, fourth-order low-pass Butterworth filter (20), and COP signal was processed with a 10-Hz cut-off, zero phase shift, fourth-order low-pass Butterworth filter (10, 21). Before starting the measurements, the equipment was first set so that either the left or right arrow would light up with a manual switch on the cue signal controller. Measurements were then started with the accelerometer and stabilometer. When the experimenter pressed a button on the cue signal controller to start measurements, a synchronization signal was sent to the light-emitting signalling device, accelerometer, and stabilometer. The light-emitting signal device received the synchronization signal and the lamp in the specified direction lit up. The accelerometer and stabilometer received the synchronization signal, and the recorded data were sent to the computer.
All participants were asked to stand upright with their heels at pelvis width on the stabilometer, facing the light-emitting signalling device (8). Participants started gait barefoot without any technical assistance, such as orthoses or assistive devices. The participants were instructed to begin walking at a normal comfortable pace when a signalling arrow came on, and, starting with the leg on the side indicated by the arrow, take at least 3 steps. Each participant started with the left and right legs randomly at least 3 times each, i.e. a total of 6 times (8, 10). The experimental environment and experimental circuit are shown in Fig. 1.
The primary endpoints were acceleration signals and COP data during gait initiation. The secondary endpoints were clinical measures of motor dysfunction evaluated by the Fugl-Meyer Assessment of Sensorimotor Recovery After Stroke Scale (FMA) Lower Extremity motor score (24), postural balance evaluated by the Berg Balance Scale (BBS) (27–29), and gait ability evaluated by the Timed 10-m Walk (10MW). These evaluations have been widely used in previous studies to clinically understand motor function in stroke patients (3, 8). Secondary endpoints were measured by a physical therapist at a later date, so that gait initiation measurements would be unaffected.
Antero-posterior and medio-lateral acceleration signals of the neck (C7), lower back (L3), and pelvis (S1) were collected for 2 s, after the signalling arrow was displayed. The accelerations were assigned a positive value when the trunk moved anteriorly or towards the stance leg side. For trunk acceleration, peak values in the antero-posterior and medio-lateral directions were measured at C7, L3, and S1 (21). The start of acceleration was defined as the point at which acceleration exceeded ±standard deviation (SD) from the mean acceleration data at rest for 1 s before the light signal, and each acceleration was analysed (20).
COP data were collected for 3 s, starting 1 s before the signalling arrow was displayed. The COP was deemed stationary if it did not move for at least 3 s, as seen on the stabilometer monitor. Movement was deemed to have started when variation in the magnitude of the combined COP after the signalling arrow was displayed exceeded ±3 SD of the variations during the stationary state (8). Antero-posterior and medio-lateral displacements of the combined COP from the stationary position to the displacement peak were calculated by combining left- and right-side ground reaction forces (21). In addition to the combined COP, the latency of the posterior displacement peak (peak latency) and the magnitude at the displacement peak (peak magnitude) of the stance and stepping leg COPs were analysed individually.
Fig. 1. Experimental set-up. A cue signal controller (Irisco Co., Ltd, Saitama, Japan) generated synchronization signals for all equipment. A signal in the left or right direction was input to the light stimulator positioned 5 m away, indicating which leg should be leading.
Statistical analyses
For each participant, the accelerations at the 3 points of the body, the combined COPs of both legs and the individual COPs, i.e. the COP of each leg, were analysed. Of the total of 6 trials, 3 measurements were made with the paretic leg leading and 3 measurements were made with the non-paretic leg leading. The mean value for each was statistically compared. Unpaired t-tests were used to analyse the difference between the control and the stroke patient groups. Paired t-tests were used to analyse the difference within the subjects. Only in the stroke patient group, correlations between the COP data and the clinical measures of FMA, BBS, and 10MW were calculated, using Pearson’s test to validate the clinical significance of the COPs. In trials leading with the paretic leg, 6 of the stroke patients did not show any posterior displacement of the individual COP, and hence were excluded from the analyses. A software package (SPSS Statistics ver. 19, IBM, Chicago, IL, USA) was used for the statistical analyses. The level of significance was set at 5%.
When the paretic leg was leading, the peak trunk acceleration at S1 towards the stance side was significantly smaller in the stroke patient group than in the control group (p < 0.01). When the non-paretic leg was leading, the peak trunk acceleration at C7, instead of S1, towards the stance side was significantly smaller in the stroke patient group than in the control group (p < 0.01). Regardless of whether the paretic or non-paretic leg was leading, there was no significant difference in antero-posterior trunk acceleration at C7, L3, or S1 when the stroke and control groups were compared.
Fig. 2 shows examples of antero-posterior displacements of the combined and individual COPs in each subject group. As shown in this example, the subjects in the control group generally demonstrated an earlier displacement peak of the stepping leg COP than that of the stance leg COP. On the other hand, in stroke patients, at least when the paretic leg was leading, the peak of the stance leg occurred earlier than that of the stepping leg. That is, the peak latency of the paretic stepping leg COP was longer than that of the non-paretic stance leg COP. Statistical analysis results of this tendency are shown in Fig. 3.
When the paretic side was leading, the peak latency of the combined COP was longer in the stroke patients compared with the controls (p < 0.05) (Fig. 3A). The peak latency of the stepping leg COP was longer in the stroke patients than the controls (a: p < 0.05) (Fig. 3B). In addition, in a comparison of peak latency in individual COPs, no significant difference was seen in peak latency of individual COPs between controls and the non-paretic stance leg in post-stroke hemiplegic patients. The comparison within the stroke patient group shows that the peak latency of the paretic stepping leg COP was longer than that of the non-paretic stance leg COP (b: p < 0.05) (Fig. 3B). As mentioned previously, 6 of the stroke patients did not show any posterior displacement of the paretic leg COP, and hence were excluded from the comparison.
When the non-paretic side was leading, the peak latency of the combined COP was longer in the stroke patients compared with the control group (p < 0.05) (Fig. 3A). The peak latency of the paretic stance leg COP in the stroke patients was longer than that of the stance leg COP of the control subjects (c: p < 0.01) (Fig. 3B). In addition, in a comparison of peak latency for individual COPs, peak latency of individual COPs on the non-paretic stepping leg in post-stroke hemiplegic patients were longer than those in control subjects (d: p < 0.05) (Fig. 3B). The comparison within the stroke patient group shows that the peak latency of the paretic stance leg COP was longer than that of the non-paretic stepping leg COP (e: p < 0.01) (Fig. 3B).
In a comparison between paretic and non-paretic sides in the stance leg, peak latency was longer on the paretic side than on the non-paretic side (f: p < 0.001) (Fig. 3B). No significant difference was seen in a comparison of peak latency between paretic and non-paretic sides in the stepping leg.
Fig. 2. Examples of antero-posterior displacements of the centre of pressure (COP) of each leg during gait initiation. (A) Control. (B) Stroke patient with the paretic leg leading. Solid line: COP trajectory of the stepping leg. Dashed line: COP trajectory of the stance leg. Arrows show the peak latency of the COP posterior displacement.
Fig. 3. Comparison of the peak latency of the combined and individual centre of pressures (COPs) in each subject group. (A) Peak latency of the combined COP. (B) Peak latency of the stance and stepping leg COPs. *p < 0.05, **p < 0.01. Error bars represent standard deviation. The letters a–f in (B) are related to comparisons described in the text.
Examples of COP displacement trajectories in each subject group are shown in Fig. 4. In general, in the control group, the peak magnitude of the individual COP was equally large for both the stance and stepping legs, while in the stroke patient group the peak magnitude was smaller for the paretic leg than for the non-paretic leg when the paretic leg was leading. Statistical analysis results of these tendencies are shown in Fig. 5.
When the paretic side was leading, the peak magnitude of the combined COP was reduced in the stroke patients compared with the control group (p < 0.001) (Fig. 5A). The peak magnitudes of both the paretic and non-paretic leg COPs of the stroke patients were also smaller than those of the control group (a, b: p < 0.001) (Fig. 5B). Within the stroke patients, the peak magnitude of the paretic stance leg COP was smaller than that of the non-paretic stepping leg COP (c: p < 0.05) (Fig. 5B).
When the non-paretic leg was leading, the peak magnitude of the combined COP of the stroke patients was reduced compared with the control group (p < 0.001) (Fig. 5A). The peak magnitudes of both the paretic and non-paretic leg COP of the stroke patients were also smaller than those of the control group (d, e: p < 0.001) (Fig. 5B). Within the stroke patients, the peak magnitude of the paretic stance leg COP was smaller than that of the non-paretic stepping leg COP (f: p < 0.01) (Fig. 5B).
In a comparison between paretic and non-paretic sides in the stance leg, peak magnitude was smaller on the paretic side than on the non-paretic side (g: p < 0.05) (Fig. 5B). In a comparison between paretic and non-paretic sides in the stepping leg, peak magnitude was also smaller on the paretic side than on the non-paretic side (h: p < 0.01) (Fig. 5B).
In terms of parameters that might correlate with APAs and to characterize them in stroke patients during gait initiation, the peak magnitude of the combined COP with the paretic leg leading was found to correlate with BBS score (r = 0.5, p < 0.05) (Fig. 6A), but not with the FMA or 10MW results. The peak latency of the combined COP with the paretic leg leading did not significantly correlate with the FMA, BBS, or 10MW results.
When the non-paretic leg was leading, neither the peak latency nor the peak magnitude of the combined COP correlated with the FMA, BBS, or 10MW results. The peak latency and the peak magnitude of the individual COPs of the paretic and non-paretic legs also did not correlate with the FMA, BBS, or 10MW results.
In contrast, when the paretic leg was leading, the peak latency of the paretic leg COP correlated with the FMA score (r = –0.57, p < 0.01) (Fig. 6B), with the BBS score (r = –0.41, p < 0.01) (Fig. 6C), and with the 10MW results (r = 0.48, p < 0.01) (Fig. 6D). The peak magnitude of the paretic leg COP with the paretic leg leading did not correlate significantly with the FMA, BBS, or 10MW results. Furthermore, no correlation was found between the FMA, BBS, or 10MW results and either the peak latency or the peak magnitude of the non-paretic leg COP.
Fig. 4. Examples of displacement trajectories of the combined and individual centre of pressures (COPs) in each subject group during gait initiation. (A) Control. (B) Stroke patients with the paretic leg leading. Stars indicate COP when the signalling arrow was displayed for gait initiation.
Fig. 5. Comparison of the peak displacement magnitude of the combined and individual centre of pressures (COPs) in each subject group. (A) Peak magnitude of the combined COP displacement. (B) Peak magnitude of the stance and stepping leg COPs. *p<0.05, **p<0.01, ***p<0.001. Error bars represent standard deviation. The letters a–h in (B) are related to comparisons described in the text.
Fig. 6. Correlations of the centre of pressure (COP) displacement in stroke patients against clinical measures of motor dysfunction, postural balance, and gait ability. (A) Relationship between peak magnitude of the combined COP and the Berg Balance Scale (BBS) score. (B) Relationship between peak latency of the paretic stepping leg COP and the Fugl-Meyer Assessment of Sensorimotor Recovery After Stroke Scale (FMA) Lower Extremity motor score. (C) Relationship between peak latency of the paretic stepping leg COP and the BBS score. (D) Relationship between peak latency of the paretic stepping leg COP and the Timed 10-m Walk (10MW) results. r: Pearson’s correlation.
The aim of this study was to investigate whether individual COPs show new characteristics of the reduced APAs during gait initiation in post-stroke hemiplegic patients. A detailed examination was conducted of the changes in individual COPs on each side as an assessment index for APA. The study revealed that individual COPs show 2 main results. The first is that a prolongation of peak latency in individual COPs and a decline in peak magnitude in individual COPs are asymmetrically produced as characteristics of the reduced APAs in post-stroke hemiplegic patients. The second result was that individual COPs of post-stroke hemiplegic patients were associated with motor impairment, balance indices, and gait ability. These results can explain the problem of left–right asymmetry and the difficulty in weight transfer to the stance leg experienced by post-stroke hemiplegic patients.
Acceleration of the pelvis (S1) toward the stance side during gait initiation was decreased in post-stroke hemiplegic patients when leading with the paretic leg compared with age-matched control subjects. This finding might be related to inactivity of the gluteus medius or ankle extensor muscles of the paretic leg, as suggested in previous studies that reported a difficulty in adjusting the centre of gravity towards the stance direction during gait initiation in post-stroke hemiplegic patients (4, 30). It might also be related to a decrease in the amount of medio-lateral displacement of the combined COP (31, 32). Moreover, the current study found that, in stroke patients, acceleration of the neck (C7) was smaller when leading with the non- paretic leg. This is thought to be due to asymmetry in the movements as a result of postural adjustment strategies to compensate for the difference in the leading leg.
In this study, the peak latency of the paretic stepping leg COP in the stroke patients was longer than that in the controls. A previous study that found longer peak latency of combined COP in stroke patients did not analyse the paretic and non-paretic legs separately (8, 10, 33). However, the current study compared the peak latency of the individual COP in the paretic and non-paretic legs of the stroke patients, and found a significant increase in the latency of the paretic leg. This appears to indicate a gap in the timing of body weight movement between the paretic and non-paretic legs when the paretic leg is swung forward. Increase in the peak latency of the paretic stepping leg COP might be a new explanation for the asymmetry and difficulty that stroke patients have when shifting their centre of gravity to the stance side (3). In the APAs of the stroke patients, the peak latency of the paretic leg COP was longer than that of the non-paretic leg due to prolonged muscle latency and spasticity of the leg on the paretic side (8). In addition, in a comparison between paretic and non-paretic sides in the stance leg, peak latency was longer on the paretic side than on the non-paretic side. This shows that peak latency of individual COPs on the paretic side when the non-paretic side is leading is the most delayed. In the stepping leg, peak latency in the individual COP was longer even on the non-paretic side compared with the control, so a delay effect is inferred on movement of the paretic side when the non-paretic side is leading. Chang et al. (17) reported that post-stroke patients showed delayed activity in the tibialis anterior, increased reaction time and impaired APA, all of which were also apparent on the non-paretic side. These changes may be involved in the delay in peak latency of the non-paretic leg when the non-paretic leg is the leading side.
No posterior displacements of the paretic leg COP were observed in 6 of the stroke patients in this study. These patients manifested with a prolonged time to heel lifting and decreased pelvic (S1) acceleration. Previous studies have reported that 35% of stroke patients lack COP displacement during the APA phase and perform slow weight transfer at low gait speeds (10). The current study suggests that, in stroke patients, the peak latencies of the paretic and non-paretic leg COPs differ, and that individual COP measurements for the stepping and stance legs are more informative than the combined COP measurements. Extension of the peak latency of the paretic leg COP shows temporal characteristics that are useful for understanding the asymmetry of movement between the paretic and non-paretic legs during gait initiation in stroke patients.
The stroke patients in the current study showed smaller magnitudes of COP displacements than did the control group, similar to previous studies (8). However, unlike previous research, the present study compared the peak magnitude of the paretic and non-paretic leg COPs separately. Our analyses showed that the stroke patients had a smaller peak magnitude of COPs in both the paretic and non-paretic legs than the controls, and that the peak magnitude of the paretic leg was smaller than that of the non-paretic leg.
The decreased peak magnitude of the paretic leg COP seems to be an unreported factor behind the decreased medio-lateral COP displacements identified in previous research (32, 33). This decreased peak magnitude may be explained by inactivity of the gluteus medius at the onset of movement, as demonstrated electromyographically by Kirker et al. (30) in post-stroke hemiplegic patients. In APAs of the stroke patients, the increased peak latency and the reduced peak magnitude of the paretic leg COP occurred with either the paretic or non-paretic leg leading, although there was a difference in the magnitude between the stance and stepping legs. Previous studies have reported inactivity of bilateral foot muscles and decreased combined COP displacements due to impaired APA, but the present results show that peak magnitude of individual COP in the non-paretic leg is also affected (8). The reduced peak magnitude of the paretic leg COP might be related to difficulty in moving the centre of gravity to the stance side during gait initiation in stroke patients (34).
In this study, investigation of the relationship between the COP displacement peaks and clinical measures showed that the peak magnitude of the combined COP with the paretic leg leading correlated significantly with BBS score. The peak latency of the paretic stepping leg COP also correlated significantly with the FMA, BBS, and 10MW results. Although previous studies reported that the combined COP displacement in stroke patients was associated with decreased gait speed and stride length (6, 13, 35), the current study showed that the peak latency of the individual COPs correlated with clinical severity in stroke patients and could be a new measure of their reduced APAs.
A limitation of this study was that detailed analysis was not possible for patients without posterior COP displacements in the paretic leg (10). In this study, details of the gait initiation mechanism were obtained by analysing left and right COPs, and foot strike patterns were not analysed (36). The relationship between foot strike pattern and kinematic parameters at gait initiation could be elucidated in greater detail by analysing foot strike patterns. Although the ratios of stroke types were not equal, participants in the current study were chronic stroke hemiplegic patients, and the inclusion and exclusion criteria were mainly set regarding motor function, thus the results would not have been markedly affected by this difference. The results of this study, unlike the asymmetry due to differences between the dominant and non-dominant lower leg reported in healthy individuals, represent the characteristics of movement disorders in post-stroke hemiplegic patients, as shown in previous studies (8, 10, 16). Further studies are needed to examine the relationship between motor dysfunction, postural balance, and gait ability in stroke patients in greater detail. Our primary interest, however, was in showing whether individual COPs could reveal new characteristics of reduced APAs in stroke patients. The findings show asymmetry in individual COPs to be a new characteristic of reduced APAs.
In summary, the present investigation of individual COPs has shown new characteristics of reduced APAs during gait initiation in stroke patients, including decreased acceleration of the trunk towards the stance leg, as well as increased peak latency and decreased peak magnitude of the paretic leg COP. In addition, the peak latency of the paretic leg COP was also related to clinical measures of motor dysfunction, postural balance, and gait ability. A newly revealed feature of the decline in APA function in stroke patients is that displacement of the paretic leg COP has increased peak latency and decreased peak magnitude, and there is delayed and insufficiently propelled initiation of movement of the paretic leg. Stroke patients might thus find it difficult to adjust their centre of gravity towards the stance side during gait initiation, which can hinder gait and balance. Therefore, it may be advisable to use exercises to help such patients move their centre of gravity towards the stance side and improve the paretic leg function. The point is that the delayed peak latency on the paretic side at the start of gait in post-stroke hemiplegic patients is associated with motor dysfunction and decreased gait balance ability. The theoretical framework of treatment is thus to promote functional improvement of the paretic leg so as to approach the timing of movement of the non-paretic leg, and to reduce temporal asymmetry. Treatments developed based on this theoretical framework may be clinically applicable to the analysis of postural control and the improvement in paretic leg function. Functional improvement in APAs can thus contribute to improvements in motor function, postural balance, and gait ability.
The authors would like to thank all the participants for their contributions to this study. The authors would also like to thank Ms Sachiko Nelson and Mr Kazuho Hosoda for assisting with the measurements at the study site. Thanks to Forte Science Communications, Inc., for editing the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize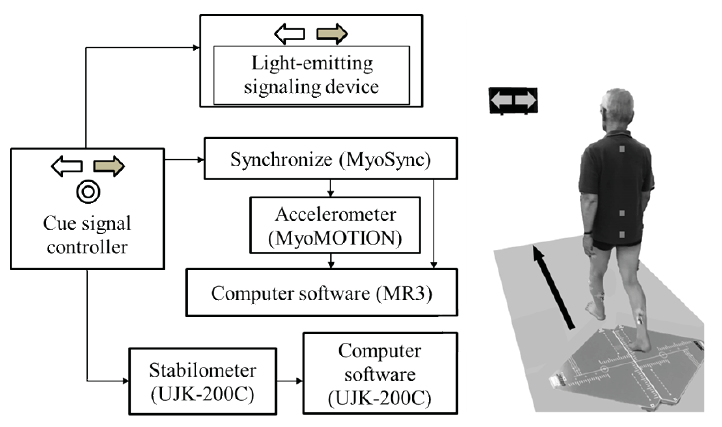 Click to show fullsize
Click to show fullsize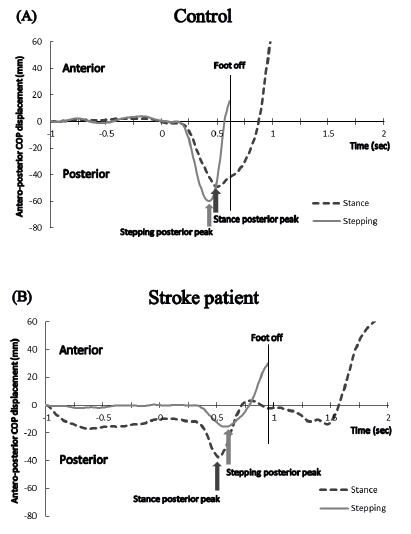 Click to show fullsize
Click to show fullsize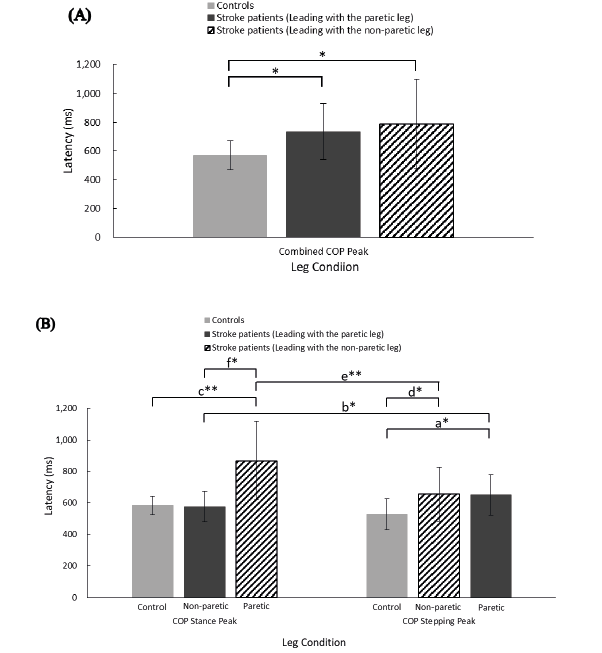 Click to show fullsize
Click to show fullsize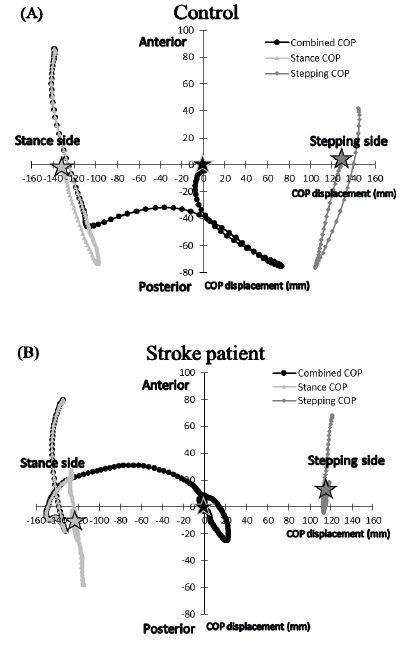 Click to show fullsize
Click to show fullsize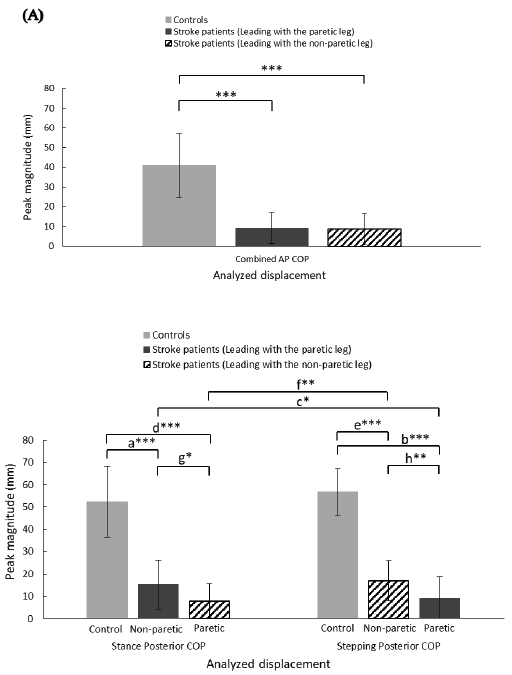 Click to show fullsize
Click to show fullsize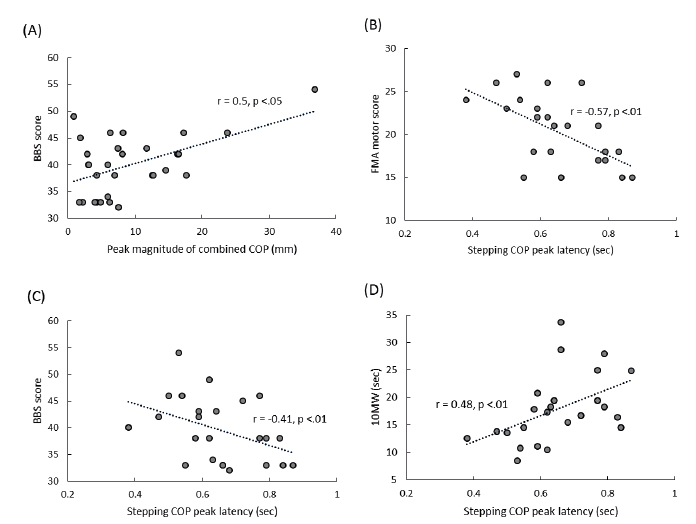 Click to show fullsize
Click to show fullsize