
1Providence Veterans Affairs Medical Center, Providence, Rhode Island, USA
2Center for Cardiac Fitness at The Miriam Hospital, Providence, Rhode Island, USA
3Division of Cardiology, Warren Alpert School of Brown University, Providence, Rhode Island, USA
Objective: To evaluate the safety and outcomes of aerobic and resistance training in patients undergoing cardiac rehabilitation after spontaneous coronary artery dissection.
Methods: Eleven patients with spontaneous coronary artery dissection at 2 academic centres were studied retrospectively during cardiac rehabilitation from July 2013 to September 2017. Patients underwent maximal effort exercise testing at enrollment and discharge per institutional protocol. Patients were prescribed individualized exercise regimens based on stress test results, stress management with a behavioural psychologist, and diet counselling with a nutritionist. Resistance training was introduced during weeks 3–5 with close blood pressure monitoring.
Results: Ten patients who completed cardiac rehabilitation showed improvements in aerobic exercise capacity and exercise duration. For resistance training, patients increased the total number of resistance exercise modalities, repetitions, or both. After cardiac rehabilitation, significant improvements were found in exercise capacity, Mental Composite Score, Physical Composite Score, anxiety measured by Generalied Anxiety Disorders (GAD-7), and positive affect. During a mean follow-up of 14 months, no patients had any recurrent dissection or major adverse cardiac events.
Conclusion: Cardiac rehabilitation is safe and improves functional status, anxiety, positive affect and quality of life in patients with spontaneous coronary artery dissection. Future studies should explore ways to further improve the psychosocial and functional status of these patients.
Key words: cardiovascular rehabilitation; secondary prevention; safety.
Accepted Feb 15, 2018; Published May 23, 2018
JRM-CC 2018; 1: 1000001
Correspondence address: Wen-Chih Wu, 830 Chalkstone Avenue, Providence, RI 02908, USA. E-mail: wen-chih_wu@brown.edu
Given paucity of literature, we studied safety and outcome of cardiac rehabilitation (CR) in patients after spontaneous-coronary-artery-dissection (SCAD). Eleven patients with SCAD diagnosed by coronary angiography during 2013–2017 who were enrolled in a hospital-based-CR program were studied. Training started with aerobic exercise for 3–5 weeks followed by resistance training while maintaining a blood pressure <140/90 during exercise. Eight of 11 patients completed 36 CR sessions, two completed 20 sessions, and one patient dropped-out after initial session. At the time of CR completion, there was improvement in CR exercise duration, number and repetition of CR resistance exercises, METs achieved during stress test, Mental-Composite-Score, Physical-Composite-Score, and GAD-7 Anxiety score. There were no major adverse cardiac events during 14 months of follow-up. CR is safe and effective in improving physical and psychosocial function after SCAD.
Spontaneous coronary artery dissection (SCAD) occurs most commonly in young women without classic cardiovascular risk factors (1). Fibromuscular dysplasia has been identified as a predisposing condition in the majority of patients with SCAD (1, 2). Patients with SCAD may present as acute myocardial infarction (AMI), ventricular arrhythmias, sudden cardiac death, or heart failure. The diagnosis is made during coronary angiography showing non-atherosclerotic, non-iatrogenic or non-traumatic arterial dissection (1). SCAD can be managed either conservatively or by revascularization (1, 2). Given that strenuous activity or extreme mental stress has been identified as a precipitating factor for SCAD, physicians may be concerned about these patients participating in cardiac rehabilitation (CR) (3). Patients may also be apprehensive about exercising due to fear of precipitating another event. Unlike AMI, there are no clear guidelines for exercise regimens in patients with SCAD, due to limited data. Since healing of dissection is seen on angiography by 4 weeks after the index event in the majority of patients (4), it is potentially safe to start CR at that time. The objective of this study is to evaluate the safety and outcomes of CR in patients with SCAD.
Data from 2 academic centres for patients with SCAD diagnosed by cardiac catheterization and enrolled in the institutional CR programme (n = 11) were studied retrospectively from July 2013 to September 2017.
The CR programme consists of 90-min sessions 3 times a week for 12 weeks. Patients also receive educational sessions and behavioural counselling on stress management, nutrition and exercise, from psychologist, nutritionist and exercise physiologist or nurse, respectively.
At enrollment and discharge, patients underwent symptom-limited exercise testing up to a maximum systolic blood pressure (SBP) of 140 or diastolic blood pressure (DBP) of 90 mmHg (whichever came first). An individualized exercise prescription was established based on the patient’s needs and entrance stress test. At induction, low intensity aerobic exercise (Stationary biking and walking or running on treadmill) was prescribed, aiming either at the lower end of the target heart rate (set at 70–85% of the maximum heart rate achieved during exercise test), blood pressure (BP) response to exercise (< 140/90 mmHg or 20 mmHg increase in SBP from baseline) or the Rate of Perceived Exertion Scale (RPE, 4–6/10 Borg scale). BP was closely monitored during resistance training to avoid excessive shear stress on the vessel wall during the lifting phase (5, 6). Patients progressed to higher intensity aerobic exercise (by increasing workloads at higher level exercise equipment) during weeks 3–5, as tolerated. Resistance training was also introduced during weeks 3–5. During the lifting phase, the SBP was monitored to maintain < 140 mmHg, and DBP to 90 mmHg or 20 mmHg increase in SBP from baseline. After patients were able to perform 12–15 repetitions of their initial regimen with the physiological parameters within the above-mentioned range, the number of repetitions and/or resistance load was increased, or another resistance exercise was introduced. It was not until this point that the patients were encouraged to start outside exercise on non-CR days.
Chart abstraction was conducted to obtain data on age, sex, medical history, AACVPR risk category (7), health-related quality of life (RAND-36: Mental Composite Scores (MCS)and Physical Composite Scores (PCS)) (8), social support (ENRICHD survey) (9), depression symptoms (PHQ-9) (10), dietary habits (Rate Your Plate survey) (11) and mood (positive and negative affect: PANAS survey) (12), exercise regimen and functional status (difference in metabolid equivalents (METs) of exit minus baseline exercise test).
Exercise regimen and progression were described qualitatively and semi-quantitatively. Before/after comparison of duration of exercise, functional status (METs in exercise test), RAND-36, ENRICHD, PHQ-9, Rate Your Plate and PANAS were performed using paired-sample t-test. A 2-sided p-value ≤ 0.05 was considered significant.
Eleven patients with SCAD on cardiac catheterization were enrolled into CR. Eight patients completed 36 ± 1 sessions, 2 patients underwent a tailored shorter regimen (20 ± 1 sessions) due to work, and 1 patient dropped out after enrollment. The patients’ mean age was 46.2 years (9 females and 2 males). Six patients had known anxiety disorder and five had cardiovascular risk factors (3 had hypertension, 1 was currently smoking and 3 were former smokers). Patients were stratified into low (n = 6), intermediate (n = 4) and high (n = 1) risk categories by AACVPR criteria.
Four patients developed SCAD while performing moderate to intense exercise (2 of whom had acute mental stress). When they developed symptoms of SCAD 2 patients were performing regular daily activities, 4 were sedentary (1 of whom had acute mental stress), and 1 patient was cheering while watching sports.
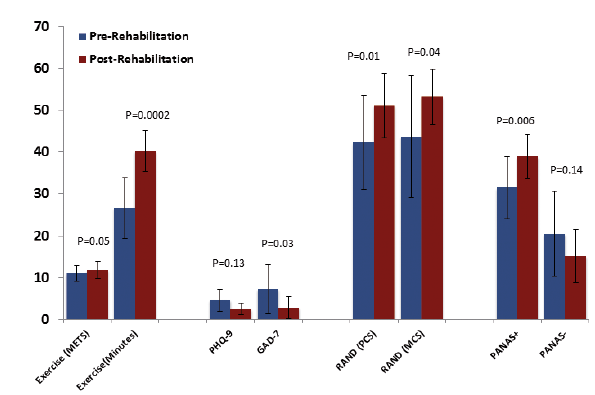
Data was reported on 10 patients, and 1 patient dropped out after the intake visit. All 10 patients attended 1–4 visits (mean 2 visits) with the CR psychologist. Eight patients attended 1–2 (mean 1) visits with the nutritionist. All 10 patients showed improvement in their aerobic exercise capacity during CR sessions, irrespective of their baseline functional capacity, with increase in exercise duration from 26.6 to 40.2 min (increase = 13.6 min, standard deviation (SD) 2.2 min; p = 0.0002). For resistance training, 7 patients increased the total number of resistance exercise modalities; 1 patient increased the number of repetitions and 2 patients increased both modality and repetitions (Table I). Data on METs improvement were analysed on 8 patients, as 1 patient did not have an exit stress test and the other patient did not have an entrance stress test. Significant improvements were found in their exercise capacity from 11.0 to 11.8 METs (increase = 0.8, SD 0.04 METs; p = 0.05).
Nine patients had a complete psychosocial assessment, while the GAD-7 score was complete in all 10 patients. The Mental Composite Score improved significantly from 43.6 to 53.1 (increase = 9.5, SD 7.8; p = 0.04), the Physical Composite Score from 42.2 to 51.1 (increase = 8.9, SD –3.5; p = 0.01), GAD-7 from 7.2 to 2.8 (change = –4.4, SD –3.3; p = 0.03), and positive affect from 31.4 to 38.8 (change = 7.4, SD –2.2; p = 0.006) (Fig. 1).
Fig. 1. Cardiac rehabilitation outcomes with mean, standard deviation and p-value at enrollment and programme completion. METs: metabolic equivalents; PHQ-9: Patient Health Questionnaire; GAD-7: General Anxiety Disorder 7-item scale; PCS: Physical Composite Score; MCS: Mental Composite Score; PANAS: Positive and Negative Affect Schedule.
No significant change from baseline was found for SBP (114.1 to 111.5 mmHg), DBP (71.5 to 69.4 mmHg), BMI (25.3 to 24.4), PHQ-9 (4.6 to 2.5), ENRICHD (30.3 to 31.8), Negative affect (20.4 to 15.1) and Rate Your Plate (54.7 to 57.3).
Three patients had non-cardiac chest pain during CR, which was treated conservatively and they returned to exercise sessions. Follow-up was available for all 10 patients, for a mean of 14 (range 6–53) months. None of them had any recurrent dissection or major adverse cardiac events.
In this study 10 patients with SCAD successfully completed CR with no serious exercise-related complications. There was significant improvement in perceived physical and mental health parameters, as well as modest improvements in exercise capacity. All patients showed improvement in duration and intensity of aerobic exercise as well as load and number of resistance exercise modalities.
This is one of the first studies to report on quantitative psychosocial and functional outcomes for a cohort of patients with SCAD who completed CR with comprehensive aerobic and resistance training. We built on previous studies by Krittanawong et al., who reported on potential psychosocial and functional benefits of CR in a qualitative fashion (3), and expanded on the feasibility and safety study of CR in SCAD described by Silber et al. (13). The current report contrasts the study by Chou et al. who utilized a Canadian CR programme, which enrolled patients with SCAD > 6 months after the initial event, on weekly sessions for 12–24 weeks (14). Similar to our results, significant improvements in functional status was reported by the Canadian regimen. However, while no significant improvements in anxiety, depression or stress scores were found by Chou and colleagues, significant psychosocial improvements (RAND-36, positive affect, anxiety) were found in our cohort.
We also found a disconnect between the remarkable improvements in exercise duration during sessions (+26 min) as well as perceived physical function (+9 points in Physical Composite Score) and the modest change in METs (+0.8). It is possible that the gradual regimen and the monitored setting helped the patients overcome their fear of exercising. Their confidence in their exercise capacity possibly increased over time, which explains the increased duration of the exercise time during sessions. The visits to behavioural psychologists may also have helped in stress management and fear, given improvements in perceived mental function (+9 points in Mental Composite Score), positive affect and anxiety scores. The potential reasons for this disconnect can be several. First, the majority of patients had excellent functional capacity at baseline, and few to none of them had comorbidities that would limit their functional ability. Secondly, the gradual regimen we used for SCAD compared with the standard CR (mean improvement of 2.0 METs in our centre) may not have enhanced their functional status improvement to a similar degree.
This study is limited by the small sample size related to the low prevalence of SCAD (0.3%) (2). In addition, there were no patients who needed to resume participation in competitive sports, which limited the generalizability of these results to that population.
In conclusion, CR is safe, and improved both psychosocial and physical function and overall quality of life in patients with SCAD. Future studies should explore ways to further improve functional status in these patients.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize