
1University of Bordeaux, Bordeaux, France
2CNRS, INCIA, UMR 5287, Bordeaux, France
3CHU de Bordeaux, Service de médecine physique et rééducation, Bordeaux, France
4EA 4136 Handicap et système nerveux, 5University of Bordeaux, Bordeaux, France
6CNRS, Institut des Maladies Neurodégénératives, UMR 5293, and 7CHU de Bordeaux, Service d’explorations fonctionnelles du système nerveux, Bordeaux, France
#These authors contributed equally to this paper.
Background: The course of Parkinson’s disease is characterized by gait disturbance and falls, which affect patients’ quality of life and engender high healthcare costs. These factors are not greatly improved by levodopa therapy or deep brain stimulation of the subthalamic nuclei. Indeed, the symptoms may even worsen with these treatment. Physiotherapy may be the most appropriate treatment to reduce the incidence of falls in these cases; how-ever, its benefits are modest.
Objective: To assess the effectiveness of trunk muscle strengthening in 10 patients with Parkinson’s disease being treated with deep brain stimulation of the subthalamic nuclei who are affected by gait disturbances and falls.
Method: A standardized physiotherapy programme centred on trunk muscle strengthening was conducted. Its effectiveness was assessed using a clinical approach combined with video-based motion analysis.
Results: After 4 weeks of trunk muscle strengthening, the gait item on the Unified Parkinson’s Disease Rating Scale (UPDRS, part 3) together with several gait kinematic parameters (step length, walking cycle duration variability, gait speed) were significantly improved and the number of falls decreased.
Conclusion: These preliminary findings suggest that physiotherapy centred on rachis mobility improves the quality of gait and reduces the number of falls in patients with Parkinson’s disease who are being treated with deep brain stimulation of the subthalamic nuclei. This is a potentially useful supplement to the traditional physiotherapy approach, in addition to the pharmacological and surgical treatment of Parkinson’s disease.
Key words: Parkinson’s disease; falls; gait; kinematic; rehabilitation.
Over time, patients with Parkinson’s disease treated operatively with subthalamic nucleus deep brain stimulation develop drug-resistant gait disturbance and falls. Traditional physiotherapy programmes for reducing the incidence of falls in these patients have modest effects. Thus, a physiotherapy programme based on trunk exercises could be helpful, since optimal axial motility and gait and posture quality are strongly linked. A specific programme was used for 10 patients with Parkinson’s disease treated operatively with subthalamic nucleus deep brain stimulation. The programme involved 2 physiotherapy sessions per day for 5 days a week over a period of 4 consecutive weeks. Quality of gait improved and the number of falls decreased significantly. In conclusion, specific standardized rehabilitation of axial motility is potentially a useful supplement to the traditional physiotherapy approach in order to reduce falls in patients with Parkinson’s disease who have been treated operatively with subthalamic nucleus deep brain stimulation.
Accepted Jun 18, 2018; Published Jan 28, 2019
JRM-CC 2018; 1: 1000003
Correspondence address: Dominique Guehl, Department of Clinical Neurophysiology, Pellegrin Hospital, Place Amélie Rabat Léon, FR-33000 Bordeaux, France. E-mail: dominique.guehl@u-bordeaux.fr
In the course of Parkinson’s disease (PD), axial symptoms, such as gait and balance impairments with falls, worsen. Up to 68% of patients with PD fall each year, with 50% falling repeatedly (1). Falls may cause multiple fractures, which are costly for medical and health services, and may be life-changing for patients (2).
Risk factors for falls in patients with PD are numerous, such as longer duration and higher severity of disease (for review see (3)). Levodopa is a potential risk factor for hip fractures, probably due to the occurrence of dyskinesia or orthostatic hypotension (4). Levodopatherapy may also make patients more mobile and therefore more likely to fall, since they are still able to move around despite their postural instability. Unpredictable freezing of gait (FOG) at step initiation, half turn, or during ongoing gait, can also induce falls (4). On the other hand, the rate of falls tends to stabilize or decrease with disease progression, since patients are more disabled and less able to move (1).
Balance and gait disabilities are difficult to treat in patients with PD, since levodopatherapy is only partially effective (5, 6). Furthermore, deep brain stimulation (DBS) of the subthalamic nucleus (STN), which is an effective treatment for rigidity, akinesia and tremor, but less so for axial symptoms, can sometimes worsen FOG and postural instability (7–10). Physiotherapy therefore represents a complementary approach for improving gait and balance (11–13). However, in some cases, it does not improve these symptoms in patients with PD, including those who have received STN stimulation. This preliminary study proposes an original standardized rehabilitation programme focused on trunk exercises in order to improve gait and reduce falls in previously operated patients with PD (STN-DBS) who continue to fall despite receiving conventional physiotherapy. In addition to a clinical approach, a three-dimensional (3D) kinematic system was used to objectively assess the influence of the rehabilitation programme on gait.
Ten patients with PD who had received STN-DBS were included in this study because they experienced gait disturbance and falls (minimum 1 fall/48 h) related to festination and/or FOG despite optimization of both pharmacological treatment and stimulation settings. Patients had to be receiving regular ambulatory rehabilitation (minimum of 2 sessions per week) from their practitioners, including gait rehabilitation and work on postural reflexes. Patients needing assistance for deambulation or with a disadvantaged family environment were excluded. All procedures performed in this study were approved by the local ethics committee from the University Hospital of Bordeaux. All patients provided written informed consent.
The patients were hospitalized in the rehabilitation department of the University Hospital in Bordeaux for 4 weeks. During this period they were treated daily 5 days a week with 2 physiotherapy sessions per day. Each session lasted 90 min. The intensity of sessions was increased progressively over the 4 weeks until the end of the period of hospitalization. In the mornings, the physiotherapy session focused on trunk mobility only. Passive trunk stretching was followed by active trunk stretching and muscle strengthening exercises in extension, flexion and rotation. In the afternoons, patients were asked to perform the same trunk exercises as in the morning for 1 h, and to perform cardiovascular training for 30 min on a cycle ergometer (Motomed, Viva 2, RECK-Technik GmbH & Co. KG, Medizintechnik, Betzenweiler, Germany). The patients were encouraged to repeat the trunk exercises every day during both the physiotherapy session and in their hospital rooms, and to correct their position as soon as they could in the evenings and at the weekend. At discharge, care was provided by their usual practitioner; patients received the same regular ambulatory rehabilitation as prior to hospitalization and were encouraged to continue trunk exercises every day, together with daily walking for at least 30 min and cycling on a stationary bicycle for 30 min 3 times a week.
Patients were assessed in the morning in the drug-On (usual dose in the morning)/DBS-On condition only, 24 h before the beginning and 24 h after the end of the rehabilitation programme. The stimulation parameter settings and drug dosages were unchanged throughout the evaluation. The total score on the motor part of the Unified Parkinson’s Disease Rating Scale (UPDRS, part 3), a composite axial score derived from the UPDRS 3 (items 18, 19, 20-face, 22-neck, 27–30), a gait score (item 30 of UPDRS 3) and a postural instability score (item 29 of UPDRS 3) were used to assess the clinical motor state of each patient. Activities-specific Balance (ABC) and Berg scales were used to assess confidence in balance and severity of imbalance (14, 15). The ABC is a 16-item scale, and ratings consist of a percentage range from 0% to 100% for each item. A score < 67% corresponds to adults at risk of falling (16). The Berg is a 14-item scale with a 5-point ordinal scale for each item, ranging from 0 to 4. “0” indicates the lowest level of function and “4” the highest level. The score out of 56 is interpreted as follows: 41–56 = low risk of falls, 21–40 = medium risk, 0–20 = high risk. Finally, a self-report questionnaire, in which the daily number of falls was noted systematically, was applied for 2 weeks before hospitalization and 3 weeks after discharge.
Patients were assessed for gait and posture on the motion platform 24 h before the beginning and 24 h after the end of the rehabilitation protocol (INCIA CNRS UMR5287, Bordeaux University).
Three-dimensional kinematic gait analyses. Kinematic data were acquired with a motion analysis system (Elite, BTS Spa, Milan, Italy) composed of 8 infrared cameras placed throughout the room (acquisition frequency 100 Hz). Each patient had reflective markers attached to the skin bilaterally on anatomical landmarks: heads of the first and fifth metatarsals, lateral malleolus, lateral femoral condyle, greater trochanter, anterior superior iliac spine, and acromion. Additional markers were positioned on the lumbar vertebra L3, thoracic vertebra T10, cervical vertebra C7 and sternum. The motion analysis system calculated the position of the markers in 3D. With the volume required for the movement, the spatial error of the system was < 2 mm (mean 1.5 mm, SD 0.2). The following gait parameters were assessed: walking speed, walking cycle duration, the variability coefficient of walking cycle duration, gait cadence, variability coefficient of cadence, double-stance duration, left- and right-stance duration, right- and left-step length, and right- and left-shifts of the trunk.
Test procedure. Patients had to walk on the walkway at a comfortable speed. Gait events (heel contact and toe-off for each foot) were identified from kinematic data, and gait spatio-temporal parameters were calculated for each cycle and then averaged with a Matlab routine (Matlab 2013, Mathworks, US). Subjects performed 6 trials, which allowed the identification of at least 18 walking cycles for each participant.
Descriptive analyses of clinical and paraclinical data (means and SD) were performed using SPSS Statistic Software (IBM SPSS Statistics). Patients served as their own controls. Comparison of clinical/paraclinical data obtained before and after rehabilitation was performed with the non-parametric Wilcoxon signed-rank test, with a threshold of significance of 5%.
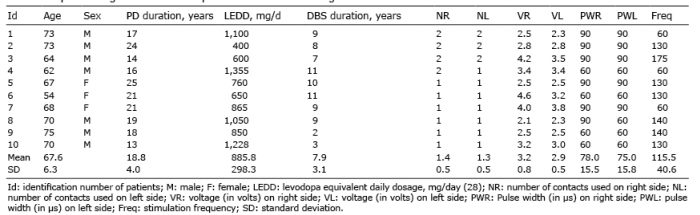
Demographic data and DBS settings are shown in Table I. The population was relatively elderly (mean age 67.6, standard deviation (SD) 6.3 years) with a predominance of men (7 males (M)/3 females (F)) and a long mean (SD) duration of disease, of 18.8 (4) years.
Table I. Epidemiological data and deep brain stimulation settings
Despite initial doubts and apprehension, no patient refused to perform or failed to complete the programme. No significant improvements were observed 4 weeks after rehabilitation regarding total UPDRS 3, postural stability and axial scores (Fig. 1; p = 0.20; p = 0.25 and p = 0.18, respectively). On the other hand, the gait item of the UPDRS 3 was significantly improved (mean 1.1 (SD 1) vs 0.7 (SD 0.7) before and after rehabilitation, respectively; p = 0.04).
Fig. 1. Impact of rehabilitation on clinical data. (*p < 0.05); For the postural stability and gait items (C and E, respectively), some values were similar between the patients. This explains why some lines are superimposed and appear as missing lines.
Individual inspection revealed an improvement in the Berg scores for patient 8 and an improvement in the ABC scores for patients 3 and 7 after rehabilitation (Fig. 2A, B). However, statistical analysis of the population did not demonstrate any significant improvement in the Berg scores after rehabilitation (mean 48.7 (SD 2.8) and 49.6 (SD 2.8) before and after rehabilitation, respectively; p = 0.39; Fig. 2A). Similarly, the mean ABC scores were not significantly improved by rehabilitation (42.6 (SD 11.1) and 45.9 (SD 11.9) before and after rehabilitation, respectively; p > 0.40; Fig. 2B). On the other hand, the mean daily number of falls decreased significantly, from 3.5 (SD 3.2) to 1.3 (SD 1.4) after rehabilitation (p = 0.01; Fig. 2C).
Fig. 2. Impact of rehabilitation on gait scales and number of falls.
Trunk posture. Two parameters related to trunk posture were analysed: the first (D1) was the horizontal distance between the C7 and L3 markers (Fig. 3A, sagittal deviation) and the second (D2) was the vertical distance between the right and left acromion markers (Fig. 3B, frontal deviation on a posterior view). There was a trend toward a decrease in D2 after rehabilitation (mean 19.8 (SD 17.3) mm and 11.1 (SD 6.8) mm before and after rehabilitation, respectively; p = 0.05). No significant change in D1 was observed after rehabilitation (mean 64.7 mm (SD 34.8) and 61.7 mm (SD 30.1) before and after rehabilitation, respectively; p = 0.89).
Fig. 3. Postural measures. (A) Measures in sagittal plane. D1: horizontal distance between C7 (7th cervical vertebra) and L3 (3th lumbar vertebra) markers. (B) Measures in frontal plane. D2: vertical distance between right and left acromion markers. T10: 10th thoracic vertebra.
Kinematic data for gait. The mean time for the walking cycle, right and left feet support durations and double-stance time were decreased significantly after rehabilitation (Table II). Rehabilitation significantly increased walking speed, cadence and length of the left step (Table II). In addition, a coefficient of variation was calculated for the walking cycle duration and cadence (CV = SD/mean × 100; (17)). Rehabilitation significantly reduced variability in the duration of the walking cycle and in gait cadence (Table II).
Table II. Impact of rehabilitation on kinematic data of gait
Rehabilitation targeting axial motility improved gait kinematic parameters and reduced the number of falls in patients with PD treated with STN-DBS. The gait item of the UPDRS 3 was significantly improved by trunk muscle strengthening, as confirmed by kinematic analysis. Walking cycle duration, and right-, left- and double-stance durations were significantly reduced by rehabilitation, together with an increase in left-step length, and an increase in gait speed and cadence. The latter was probably related to a significant decrease in variability in duration of walking cycles and a decrease in cadence variability after rehabilitation. The failure to increase right-step length was probably related to the higher rigidity and akinesia scores in the right lower limb than in the left lower limb in our population. Typically, parkinsonian gait is slow, with a shortened step length, reduced speed and an increase in variability of step length (18). These gait parameter abnormalities seem to predict falling in patients with PD and elderly people (19). Our patients experienced falls, although their Berg and ABC scores suggested a low risk of falling (16). This apparent discrepancy could be due to the fact that these scales were first designed to assess the risk of falling in elderly healthy patients. In addition, a ceiling effect on the Berg test was previously reported in patients with PD (20). Furthermore, this test does not assess reactive postural control, which is important, as it is associated with a greater risk of falling. On the other hand, the number of self-reported falls decreased significantly after rehabilitation, suggesting an indirect effect of axial mobility on the risk of falling in these operated patients with PD. This could be due to postural changes related to trunk muscle strengthening and/or the improvement in gait quality, as mentioned above. The axial and postural stability items of the UPDRS 3 were not modified by axial rehabilitation. This apparent lack of effectiveness of axial rehabilitation on clinical scores could be due, in part, to the size of the sample and to the fact that these clinical items represent only crude measures of balance disability and are subject to variations in clinical performance and interpretation (21). Indeed, clinical assessment of axial signs, such as gait and balance, remains imprecise, subjective and semi-quantitative. On the other hand, patients tended to improve their posture in the frontal plane, as suggested by a clear trend (p = 0.05) to a decrease in frontal deviation (D2 distance). Trunk-specific rehabilitation treatment has been reported previously to improve lateral trunk flexion in patients with PD (11). Postural abnormalities, notably mediolateral oscillations, are known to be associated with a higher risk of falling in patients with PD (22). Thus, our data suggest that the tendency to postural improvement in the frontal plane observed after trunk muscle strengthening in our population could have contributed to a reduction in the number of falls.
Regarding the impact of gait quality on the number of falls, our patients especially seemed to fall due to gait akinesia with festination episodes and some freezing of gait. Consequently, improvement in gait parameters due to trunk muscle strengthening could explain the decrease in the number of falls. The mechanisms by which trunk muscle strengthening improves quality of gait remain poorly understood. An abnormal increase in activity of trunk muscles during walking was reported recently in patients with PD who fall (23). This increase in axial rigidity could lead to less independence of the pelvis, trunk and head. This could, in turn, induce disturbed balance during walking (24, 25). Thus, we hypothesize that changes in axial motility induced by our physiotherapy programme may improve the coordination between the axial segments, and that this improvement could have a positive impact on gait quality. This hypothesis is in line with the notion that quality of gait and risk of falling depend closely on axial motility (26). In their study, Stozek et al. reported gait improvement in patients with PD after a rehabilitation programme including various physical exercises, such as trunk rotations (27).
In conclusion, trunk muscle strengthening should be an ongoing adjunct to PD medication and classical physical therapy in the context of gait abnormality with falls in patients with PD treated with STN-DBS.
Nevertheless, these preliminary data should be viewed with caution due to the small size of the patient sample. The therapy proposed in this study is probably more intensive than is generally available in routine care. How-ever, no patient refused the therapy or failed to perform it completely. Clinical and paraclinical data were collected 24 h after the end of the rehabilitation programme, whereas the number of daily post-rehabilitation falls was assessed 3 weeks after discharge. Thus, even if this period is short, it should be taken into account before directly associating these 2 types of parameter. Our results were obtained in patients with advanced PD who were operated for the severity of the disease (STN stimulation). It would therefore be interesting to administer this programme to non-operated patients. Our data, obtained by movement platform analysis, do not exactly reflect the patient’s environment, thus the parameters we measured are difficult to translate into routine daily practice. Finally, it remains to be investigated whether the reduction in falls and the improvement in gait found with our protocol have an impact on patients’ quality of life, and how long the benefit lasts.
In conclusion, gait and balance impairments are frequent in the course of PD, and involve a high risk of falls. Dealing with these axial symptoms is a challenge that not only concerns improving the autonomy and quality of life of these patients, but also reducing the cost of medical and health services. These preliminary results are encouraging and suggest that specific rehabilitation focused on axial motility is a potentially useful supplement to the traditional approach (pharmacological/surgical) of treating the primary deficits in patients with PD treated with STN-DBS.
The authors would like to thank the physiotherapists who cared for patients during the 4-week period of rehabilitation, and Ray Cooke for copyediting the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize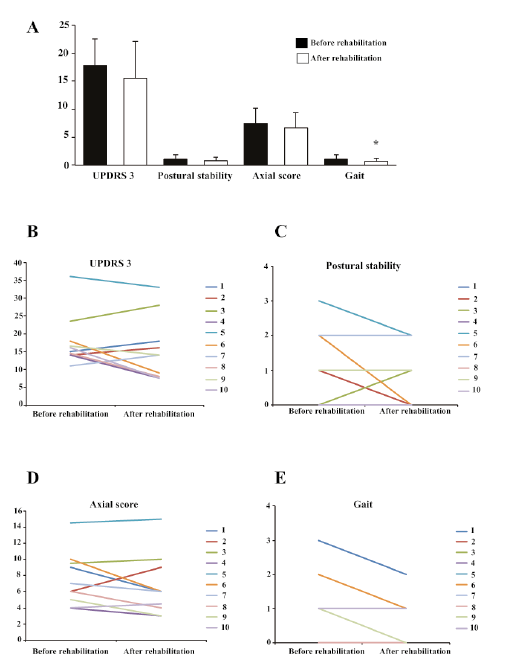 Click to show fullsize
Click to show fullsize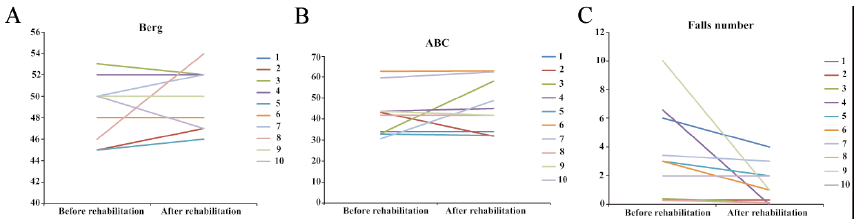 Click to show fullsize
Click to show fullsize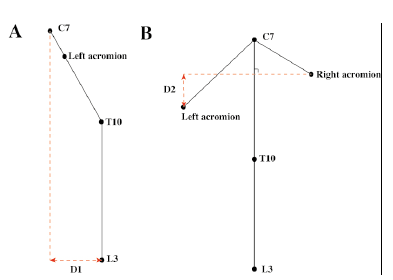 Click to show fullsize
Click to show fullsize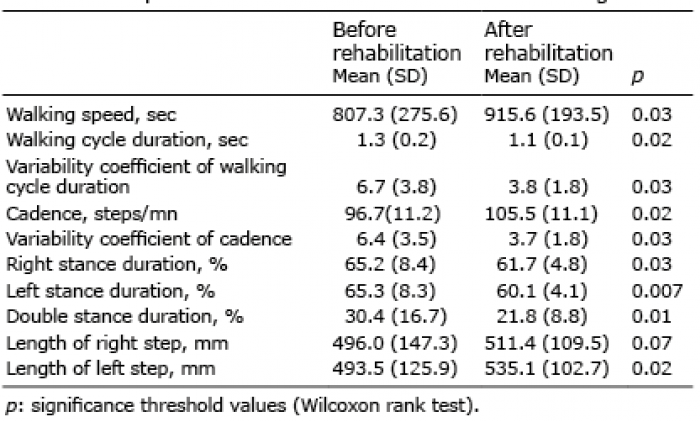 Click to show fullsize
Click to show fullsize