
1Division of Endocrinology, Department of Medicine, Cumming School of Medicine, University of Calgary, Calgary, Canada
2Division of Physical Medicine and Rehabilitation, Department of Clinical Neurosciences Cumming School of Medicine, University of Calgary, Calgary, Canada
Background: Growth hormone deficiency is a recognized consequence of traumatic brain injury. The aim of this study was to determine adherence to human growth hormone therapy among patients with traumatic brain injury compared with patients with hypothalamic or pituitary disease.
Methods: A retrospective chart review of patients with traumatic brain injury referred for growth hormone stimulation testing since December 2013. Within the same electronic medical record, patients who were started on human growth hormone for aetiologies other than traumatic brain injury were reviewed. Adherence to therapy at 1-year follow-up was compared.
Results: Of the patients with traumatic brain injury, 12/23 (52%) returned for follow-up at 1 year to continue human growth hormone treatment, whereas 11/23 (48%) did not return at 1 year. Amongst the patients with non-traumatic brain injury: 25/29 (86%) continued human growth hormone treatment, vs 4/29 (14%) who did not return. A higher proportion of patients with non-traumatic brain injury continued human growth hormone treat-ment; χ2 (1, n = 52)p = 7.238, p = 0.007.
Conclusion: There may be differences in the patient-perceived benefits of human growth hormone between these patient populations. However, it is important to consider the potential influences of cognitive and psychosocial dysfunction that can occur in patients with brain injuries.
Key words: endocrinology; neuroendocrinology; traumatic brain injury; acquired brain injury.
Accepted Sep 25, 2018; Published Nov 16, 2018
JRM-CC 2018; 1: 1000008
Correspondence address: Kirstie Lithgow, Division of Endocrinology, Department of Medicine, Cumming School of Medicine, University of Calgary, 1820 Richmond Road SW, Calgary AB, Canada, T2T 5C7. E-mail: kclithgo@ucalgary.ca
Traumatic brain injuries can damage the pituitary gland and cause hormone deficiencies. Growth hormone deficiency is the most common hormone deficiency in patients with head injuries. These patients have adverse symptoms and poor quality of life, but it is not known whether these issues can be reversed or improved by growth hormone replacement therapy. This study investigated how many patients who started on growth hormone therapy after brain injury continued the treatment long-term. This allowed us to estimate whether the patients perceived such treatment to be beneficial. More than half (52%) of the patients with traumatic brain injury chose to continue growth hormone therapy for one year or longer. However, while some patients with brain injury may experience benefit from growth hormone replacement, it is possible that not all patients find growth hormone therapy helpful.
Growth hormone deficiency (GHD) is an increasingly recognized potential consequence of traumatic brain injury (TBI) (1). Patients with GHD may present with impaired concentration, memory loss, low energy, depression, anxiety, social isolation, and poor quality of life (1–3). These symptoms are non-specific in nature and may overlap with the neurological and psychiatric sequelae of TBI. If symptomatology persists following TBI, formal evaluation for GHD with dynamic testing is an established practice at many centres, as GHD represents a potentially correctable aetiology contributing to reduced quality of life (2, 3). However, in the absence of any large, randomized control trials evaluating the efficacy of human growth hormone (hGH) replacement in this population, it is difficult to determine whether this therapy leads to any objective and measurable benefit. In a cohort of individuals with GHD due to other aetiologies (primarily hypothalamic and pituitary diseases), when hGH therapy was provided in a full reimbursement setting, adherence at 2 years exceeded 80% (4). Long-term adherence to hGH may therefore serve as a pragmatic indicator of patient-perceived efficacy, especially given that ongoing clinical follow-up was one of the only requisites for continuing treatment in this previous study (4). This is similar to our practice locally; after patients are proven to have GHD by dynamic testing, they are prescribed a 1-year supply of hGH (which is reimbursed by all insurers operating in our province) and must self-initiate a follow-up appointment at 12 months if they wish to have ongoing prescriptions for this therapy. Our objective was to evaluate adherence to hGH in individuals with GHD following TBI, and directly compare the adherence rates to that in other patients with GHD of non-TBI aetiology within the same referral population.
The procedures followed in this study were in accordance with the ethical approval of the Conjoint Health Research Ethics Board at the University of Calgary, Calgary, Alberta, Canada. Due to the retrospective nature of the study, the Ethics Board granted a waiver of the requirement to obtain informed consent from each patient. A retrospective review was performed of the electronic medical record (EMR) of patients referred to endocrinology from the Calgary Brain Injury Program in the period December 2013–2016 and subsequently diagnosed with GHD by dynamic testing (insulin tolerance test or glucagon stimulation test) and started on therapy with hGH ≥ 12 months ago. Within the same EMR, we reviewed records from patients who had been started on therapy with hGH for aetiologies of GHD other than TBI ≥ 12 months ago. From each patient chart, we collected demographic information, including age, sex, and severity of injury for the patients with TBI, and aetiology of GHD for the patient with non-TBI. Severity of injury was classified based on the Mayo Clinic Classification, which utilizes information regarding Glasgow Coma Scale, post-traumatic amnesia, and loss of consciousness to retrospectively determine the severity of TBI (5). For both groups of patients, we recorded the adherence to therapy at 1 year, which was defined according to the presence or absence of patient-initiated clinic follow-up within 12 months of starting hGH, a requisite step for ongoing prescriptions.
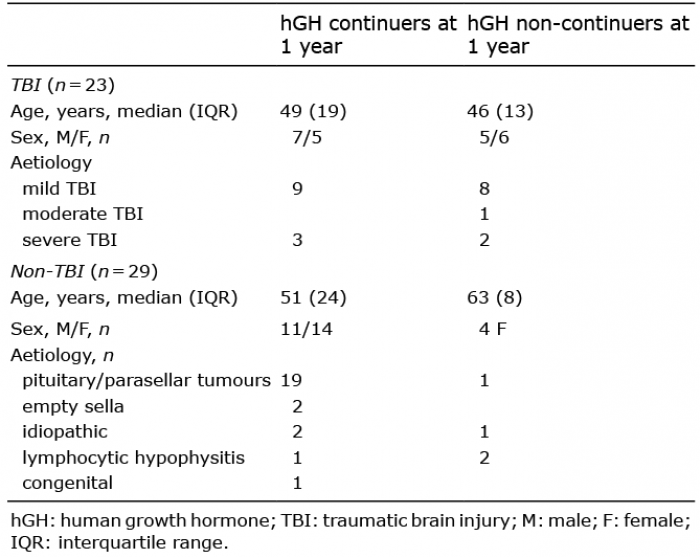
From the cohort of patients with GHD secondary to TBI, we identified 23 who were started on hGH more than 1 year prior to the time of analysis. Seventeen patients had mild, 1 had moderate, and 5 had severe TBIs. Twenty-nine patients with GHD secondary to other hypothalamic/pituitary disease, who had been prescribed GH for 1 year or more were identified. There were 19 patients with parasellar tumours, 4 with lymphocytic hypophysitis, 3 with idiopathic GHD, and 2 with empty sella syndrome, and 1 with congenital hypopituitarism. Of the patients with TBI, 12/23 (52%) returned for follow-up at 1 year and opted to continue hGH, whereas 11/23 (48%) did not return for follow-up at 1 year. Amongst the patients with non-TBI: 25/29 (86%) had opted to continue on hGH, vs 4/29 (14%) who did not continue therapy after 1 year. The characteristics of hGH continuers and non-continuers are shown in Table I.
Table I. Characteristics of patients
There were no trends with respect to age and sex between the continuers and non-continuers in either group of patients. A χ2 test was performed to examine the relationship between aetiology of GHD (TBI or non-TBI) and adherence to hGH; the patients with non-TBI were more likely to continue hGH; χ2 (1, n = 52) = 7.238, p = 0.007.
At 1 year, we observed high adherence rates to therapy
with hGH for patients with GHD secondary to hypothalamic-pituitary disease, whereas the adherence rates amongst patients with GHD secondary to TBI were comparatively modest. This suggests that there may be a difference in the patient experience or subjective benefits of GH replacement between those with GHD due to anatomical pituitary disease vs those with GHD due to TBI. However, in interpreting these results it is important to consider the potential influences of co-morbidities and psychosocial dysfunction that can occur in patients who have sustained brain injuries. TBI is known to be associated with chronic pain, mood disorders, sleep disorders, substance abuse, apathy, and long-term disability (6–9), all of which may be important barriers to adherence and follow-up. Patients with TBI may also have significant deficits in cognition and memory (10), which may contribute to missed appointments and medication non-adherence, further limiting the potential benefits of hGH therapy. Given the potential cognitive deficits and psychosocial barriers in patients with TBI, they may benefit from more intensive follow-up and additional reminders to return for appointments. Nonetheless, similar to the study described previously (4), our observations occur in a setting in which long-term continuation of hGH is highly feasible from a patient perspective; the medication is provided with complete or near-complete insurance reimbursement, and annual patient initiated follow-up is the only requirement for ongoing prescriptions. Given the lack of modifiable barriers to continuing hGH at our centre, adherence represents a practical means of estimating patient perceived efficacy.
Long-term adherence with growth hormone therapy may be impacted by other factors. Cut-offs for dynamic tests of growth hormone reserve have not been validated in the TBI population, and we were unable to obtain body mass index (BMI) values, which can influence peak GH response (11). These factors may have led to overestimation of the rates of GHD. In the absence of a blinded clinical trial, we cannot rule out that ongoing adherence to hGH was due to some degree of placebo effect. Our methodology did not allow for assessment of patient factors, including education, occupation, and socioeconomic status, which may have been a source of bias. Patients with hypothalamic and pituitary diseases often have had long-term follow-up with endocrinology prior to developing GHD, and require ongoing follow-up for replacement of other pituitary hormones of greater physiological importance than GH, whereas patients with TBI have comparatively limited contact with endocrinology. The patients with non-TBI may therefore have established better therapeutic rapport with the treating endocrinologist, which may influence the different patterns of follow-up and adherence to therapy seen in these 2 patient populations
Given the significant morbidity observed within this population, we are encouraged that a substantial proportion of patients with TBI elected to continue hGH therapy long term. GHD can have detrimental effects on both psychological and physical health, which may improve with hGH therapy. Previously reported benefits of hGH include improvements in sleep, energy, motivation, quality of life, motor speed, executive function, and memory (2, 12). We speculate that the hGH continuers experienced some degree of favourable effects that justified their long-term adherence, but additional investigation is required to validate this point. Our findings therefore underscore the need for further clinical outcome-oriented research in patients with GHD secondary to TBI, ideally in the form of a larger randomized placebo controlled trial.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize