
1Department of Rehabilitation Medicine, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands
2Capri Cardiac Rehabilitation Rotterdam, Rotterdam, The Netherlands
Accepted Aug 24, 2018; Published Jan 28, 2019
On May 29, 2018, Nienke ter Hoeve, defended her PhD thesis: Optimizing Cardiac Rehabilitation at the Erasmus University Rotterdam, The Netherlands. Supervisor: Henk J. Stam, Hendrika J. G. van den Berg-Emons and Ron T. van Domburg.
Cardiac rehabilitation focuses on the adoption of a healthy lifestyle and the optimization of cardiovascular risk factors and psychosocial status. Previous studies have shown that cardiac rehabilitation successfully improves health (e.g. blood pressure and lipid profile), quality of life, and risk of mortality in patients with coronary heart disease. Less is known about the effects of cardiac rehabilitation on physical activity, sedentary behaviour, fatigue and participation in society. The first part of this thesis focused on changes in these outcome measures in a cohort of patients participating in standard cardiac rehabilitation. The second part of the thesis evaluated the added value of behavioural lifestyle interventions integrated into standard cardiac rehabilitation.
The cardiac rehabilitation programme investigated lasted 6–12 weeks. The core of the programme consisted of an exercise programme (twice per week). In addition, educational sessions on cardiovascular risk factors and a heart-healthy lifestyle were offered. Upon indication and motivation, patients could also participate in a stress management programme, a dietary programme, a smoking cessation programme, and/or an individualized psychological programme. Measurements were performed at the start of the rehabilitation programme, at the end of rehabilitation (3 months) and at 12-month follow-up.
Physical activity and sedentary behaviour were measured in-depth using accelerometers. The results revealed that patients achieved a small improvement in moderate-to-vigorous intensity physical activity (MVPA; +5 min/day) by the end of the rehabilitation programme. More substantial improvements occurred for sedentary behaviour (–22 min/day). Despite these improvements, by the end of cardiac rehabilitation patients still spent relatively little time in MVPA and a long time sedentary. In conclusion, additional resources are needed to further improve physical activity and sedentary behaviour.
With regard to fatigue, there were improvements during and after cardiac rehabilitation. However, the prevalence of severely fatigued patients remained high 12 months after cardiac rehabilitation (8%) compared with a healthy population (3.5%). For patients with severe fatigue additional interventions seem necessary.
Regarding participation in society, the proportion of patients experiencing restrictions decreased from 69% before cardiac rehabilitation to 29% at 12-month follow-up. Dissatisfaction with participation decreased from 71% to 53%. Despite these considerable improvements, the proportion of patients that experienced restrictions and dissatisfaction remained high at follow-up. Since we also found that experienced restrictions and dissatisfaction are associated with quality of life, we suggest that a more individualized approach, focusing on activities in which restrictions and dissatisfaction are experienced, is needed.
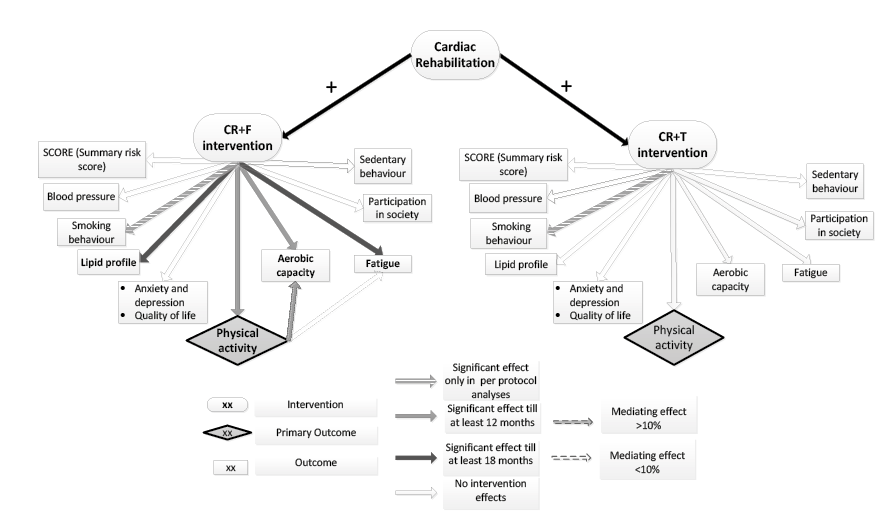
The second part of this thesis examined the outcomes of the OPTICARE randomized controlled trial to investigate the added value of 2 novel behavioural lifestyle interventions in addition to standard cardiac rehabilitation (Fig. 1). The first novel CR+F (cardiac rehabilitation+ face-to-face counselling) intervention consisted of 3 months of standard cardiac rehabilitation with the addition of 3 pedometer-based, face-to-face physical activity group counselling sessions. This initial phase was followed by 9 months of aftercare with 3 face-to-face group counselling sessions focusing on several lifestyle components (e.g. healthy diet, physical activity, and psychosocial functioning). The second novel intervention, the CR+T (cardiac rehabilitation+ telephonic counselling) intervention consisted of 3 months of standard cardiac rehabilitation with no additions in the initial phase. After the initial phase, patients participated in 9 months of aftercare with 5–6 telephone counselling sessions, which also focused on several lifestyle components. Measurements were performed at the start of the rehabilitation programme, and at 3-, 12- and 18-month follow-ups.
Fig. 1. Schematic representation of the outcomes of the OPTICARE randomized controlled trial: intervention effects of novel interventions compared with standard cardiac rehabilitation (CR) only. CR+F: cardiac rehabilitation plus face-to-face group counselling; CR+T: cardiac rehabilitation plus telephone counselling.
Compared with standard cardiac rehabilitation, adding 3 pedometer-based physical activity counselling sessions (initial phase CR+F) improved daily step count by an additional 500 steps/day at 3 months. Furthermore, time spent in prolonged MVPA periods (>10 min, which is suggested for health benefits) increased. There were no changes in total MVPA time or sedentary behaviour. At completion of the CR+F aftercare programme, improvements in step count partly diminished. However, the additional improvements in prolonged MVPA were maintained. No additional benefits were found for the CR+T intervention with regard to physical activity or sedentary behaviour (Fig. 2).
Fig. 2. Volume of physical behaviour and distribution over time. CR: cardiac rehabilitation; CR+F: cardiac rehabilitation plus face-to-face group counselling; CR+T: cardiac rehabilitation plus telephonic counselling; CR-only: standard cardiac rehabilitation; m: months. *Significant intervention effect for CR+F compared with CR-only.
The CR+F intervention was also successful in sustaining aerobic capacity gains up to 12 months and reaching long-term (18 months) improvements in fatigue. No additional improvements were found for participation in society. Again, no additional benefits were found for the CR+T intervention.
None of the novel interventions led to additional benefits with respect to SCORE, a risk function that estimates the 10-year risk of cardiovascular death based on total cholesterol, systolic blood pressure, and smoking status. Following standard cardiac rehabilitation patients had largely already reached target levels for modifiable risk factors.
Based on these results, it is recommended that face-to-face physical activity group-counselling sessions, including objective feedback (CR+F) be added to standard cardiac rehabilitation, although aftercare optimization is needed. The additional benefits in aerobic capacity and fatigue increase the clinical relevance of the CR+F intervention. These outcomes suggest that, with regard to cardiovascular risk factors, no additional resources are needed.
The OPTICARE RCT is an investigator-initiated study co-financed by Capri Cardiac Rehabilitation Rotterdam (the Netherlands), who financed the CR+F intervention, and the Zilveren Kruis healthcare insurance company (the Netherlands), who financed the CR+T intervention.
The author has no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize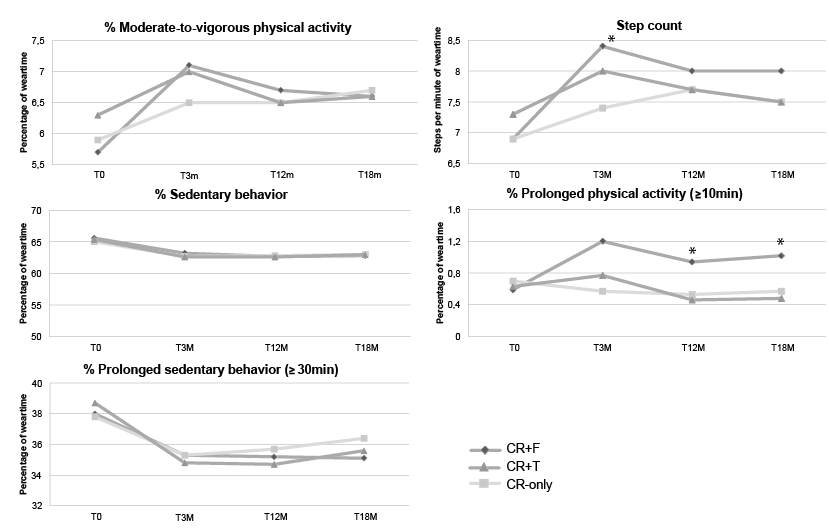 Click to show fullsize
Click to show fullsize