
1Physiotherapy Department, Alder Hey Children’s NHS Foundation Trust, Liverpool, UK
2Children’s Nursing, Edge Hill University, Ormskirk, UK
3School of Health Professions, University of Plymouth, Plymouth, UK
4Oncology Department, Alder Hey Children’s NHS Foundation Trust, Liverpool, UK
5Department of Biostatistics, University of Liverpool, Liverpool, UK
6Department of Neurology, Alder Hey Children’s NHS Foundation Trust, Liverpool, UK
7Department of Physiotherapy, LUNEX International University of Sport, Exercise and Health, Differdange, Luxemburg
Objective: To determine current international practice regarding physiotherapy input for children with ataxia following surgery for posterior fossa tumour.
Design: An e-survey covering the following domains: participant demographics, treatment/intervention, virtual training, intensity/timing of treatment, and aims and outcomes of physiotherapy management.
Participants: Physiotherapists involved in the management of children with ataxia following surgical resection of posterior fossa tumour. Participants were contacted via 6 key groups; Paediatric Oncology Physiotherapy Network (POPs), Association of Paediatric Chartered Physiotherapists (APCP), European Paediatric Neurology Society (EPNS), International Society of Paediatric Oncology (SIOP)-Europe Brain Tumour Group, Posterior Fossa Society (PFS), and Pediatric Oncology Special Interest Group (SIG) (American Physical Therapy Association).
Results: A total of 96 physiotherapists participated: UK (n = 53), rest of Europe (n = 23), USA/
Canada (n = 10), and Australia/NZ (n = 10). The most common physiotherapy interventions used were balance exercises, gait re-education and proximal control activities. The most frequently
used adjuncts to treatment were mobility aids and orthotics. Challenges reported regarding
physiotherapy treatment were: reduced availability
of physiotherapy input following discharge from the acute setting, lack of evidence, impact of adjuvant
oncology treatment, and psychosocial impact.
Conclusion: This e-survey provides an initial scoping review of international physiotherapy practice in this area. It establishes a foundation for future research on improving rehabilitation of ataxia in this population.
Key words: paediatric; brain neoplasm; ataxia; rehabilitation; cerebellum.
Accepted Sep 25, 2019; published Dec 30, 2019
JRM-CC 2019; 2: 1000020
Correspondence address: Helen Hartley, Physiotherapy Department, Alder Hey Children’s NHS Foundation Trust, Eaton Road, Liverpool, L12 2AP, UK. E-mail: Helen.hartley@alderhey.nhs.uk
The aim of this study was to determine how physio-therapists in different countries currently treat children with balance/coordination problems following surgery for a brain tumour. An e-survey, with questions on type of physiotherapy treatment, intensity and timing of treatment, and aims and outcomes of physiotherapy management, was sent to special interest groups, which included physiotherapists with expertise in this area. A total of 96 physiotherapists participated in the survey. The most common physiotherapy treatments used were balance exercises and gait re-education. Mobility aids and orthotics (e.g. splints) were also commonly used. Physiotherapists reported challenges to treatment, including lack of availability of physiotherapy following discharge from hospital, lack of evidence to guide treatment, and impact of oncology treatment (e.g. chemotherapy/radiotherapy) on the child’s rehabilitation. In conclusion, there is little evidence in this area. The results of this survey provide an initial basis to understand the challenges of treatment and to plan future research.
Brain tumours are the most common group of solid tumours in childhood, accounting for almost one-quarter of all paediatric neoplasms worldwide (1). Approximately 50% of all childhood brain tumours are located in the posterior fossa region (2). Management of posterior fossa tumours (PFTs) typically involves surgical resection, solely or in combination with adjuvant treatment, such as radiotherapy or chemotherapy.
Children with PFT have a distinctive set of issues, including potential for change pre-/post-operatively, rapid onset of ataxia, hydrocephalus and increased intra-cranial pressure, in addition to potential problems from subsequent oncological management, such as radiotherapy. Of these issues, ataxia is the predominant motor problem in children with PFT (3, 4). Ataxia can describe a related number of impairments, including upper-limb control, balance, gait difficulties, oculomotor dysfunction, and speech problems (5). Wilne et al. (6) presented a systematic review and meta-analysis with pooled data from 5 studies of children with PFT (n = 476), reporting that 60% of children demonstrated ataxia pre-operatively, indicating the prevalence of ataxia in this population group.
In addition, there is increasing understanding of the long-term impact on mobility in this population group, with up to 70% of children noted to have balance problems following completion of neurosurgical/oncology treatment (3, 7). Following surgical management of PFTs, children are typically referred for rehabilitation, including physiotherapy, yet there is little evidence to guide physiotherapists on how best to assess and treat this population. Balance and coordination problems can be a significant challenge following initial treatment, as these can affect activities of daily living, return to school, and participation with peers (3, 8).
Despite the lack of evidence to guide best practice, it is recognized that physiotherapy is integral to the treatment of children with neurological deficits following management of a brain tumour (9), yet, to date, the practice of physiotherapists in managing children with PFT has not been reported. Understanding current practice could help with development of clinical guidelines and assist with the planning of clinical trials in this population. In order to gain increased knowledge of physiotherapy treatment for children with PFT across different countries, an e-survey was developed to scope current practice.
This is the first study to investigate the current practice of physiotherapists in this population group. The aim of the study was to determine current international practice regarding physiotherapy input for children with ataxia following surgical resection of PFT.
Study design
A cross-sectional study design was used, with data collected via an online survey (e-survey).
Participants
The target population in this study was physiotherapists who were involved in the assessment and treatment of children with ataxia following surgical resection of PFT. The survey (in English) was disseminated via the Paediatric Physiotherapy Network groups of Paediatric Neurosciences Physiotherapists and Paediatric Oncology Physiotherapists (both UK-based groups), the Association of Paediatric Chartered Physiotherapists (APCP), International Society of Paediatric Oncology European Brain Tumour group (SIOP), Children’s Oncology Group (COG) (international membership), Paediatric Physical Therapist Special Interest Group (USA), Posterior Fossa Society (international multidisciplinary special interest group), and European Paediatric Neurology Society (EPNS). “Snowballing” was encouraged, through an automatic request as part of the e-survey to forward the link to therapy colleagues with an interest in this area.
The study was approved by Edge Hill University FOHSC Research Ethics Committee (FOHSC 170).
Instrument
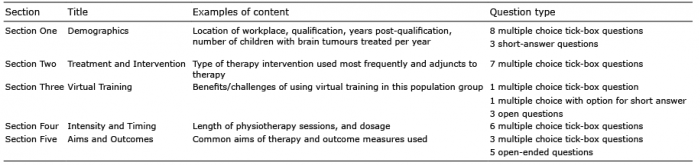
A literature search identified no previous surveys on this topic that could be used for this study. An e-survey (SurveyMonkey®) was therefore designed by the research team (who have clinical expertise in this field and a background in survey development) to ensure that the specific aim of this study was met. The e-survey had 5 domains (Table I), with a mixture of open and closed questions. The survey began with an initial filter question checking that respondents were physiotherapists working with children with PFTs. Selecting “no” to the filter question directed potential respondents to an automatic response that ended their participation.
The e-survey included a section on virtual training (defined as the use of computer technologies that provide an interactive environment requiring limb movement to react to on-screen game-play (10)), reflecting the recent trend towards the use of technology in paediatric neuro-rehabilitation (11, 12). This section was also planned to inform development of a future RCT examining virtual training intervention in children with ataxia following surgical resection of PFTs.
Prior to disseminating the e-survey it was piloted in order to optimize face and content validity and reliability (13). Four clinicians were purposefully selected to ensure that there were 2 contacts from the UK (an acute hospital-based therapist and a community-based therapist), a representative from Europe (speaking English as a second language) and a representative from the USA. Minor changes were made to the questionnaire as a result of the pilot feedback.
Table I. Structure of e-survey
Procedure
The e-survey was disseminated via gatekeepers for each of the identified network groups, with permission from each group received to circulate the e-survey to its members. This enabled the gatekeepers to email their members with a link to the e-survey. A short introductory page of the e-survey provided the participants with sufficient information to enable them to reach an informed decision as to whether to participate. The return of the survey was deemed to be the respondent’s consent to participate. The respondents were given 2 weeks to respond, then a reminder was sent electronically. All due care and attention was paid to the management of the data, in line with guidance from local policies and the General Data Protection Regulation (GDPR 2018). The respondents’ responses were anonymous.
Data analysis
Using SurveyMonkey®, the data were exported into a Microsoft Excel spreadsheet for further analysis. Descriptive statistics were used to report the closed questions. The qualitative analysis was informed by a deductive approach situated in an essentialist framework (reporting the respondents’ perceptions and experiences assuming a straightforward relationship between the written responses and the perceptions) (14). All data from selected open questions were transferred from Microsoft Excel into NVivo to allow the data to be read and re-read and initial codes generated. Codes were sorted and organized into groups, and where there was evidence of recurring responses initial themes were developed and subsequently refined.
A total of 120 out of 140 respondents who accessed the survey answered yes to the initial filter question and proceeded to enter the e-survey. It is not possible to report a response rate, since it is not known how many physiotherapists the e-survey reached, due to the method of disseminating the e-survey and subsequent snowballing.
Initial questions were answered by 96 respondents, with some of the later open-ended questions answered by fewer respondents (mean 60 respondents); however, some of these questions were applicable only to certain physiotherapist groups, e.g. if they had used virtual training. Where abbreviations were used by respondents in quotations presented in the paper, these have been written in full for the sake of clarity. Throughout the results section percentage responses are presented, calculated from the number of respondents who answered each individual question.
Demographics
Overall, 12 countries were represented, with more than 50 responses from physiotherapists across the UK, 23 from the rest of Europe (including Belgium, Germany, France, Italy, Lithuania, the Netherlands and the Republic of Ireland), 10 from the USA/Canada, and 10 from Australia/New Zealand. Further details are shown in Table II.
Fifty-nine percent (n = 56) of respondents had more than 5 years’ experience of working with children with brain tumours. The median number of children with PFT treated per year was 10. Where respondents indicated that they had completed further training, the most common type of training was a short course in either ataxia or oncology.
The primary work setting of the respondents was an inpatient setting (72%, n = 66), with 66% (n = 61) of physiotherapists reporting that they worked within a specialist team for neuro-oncology (Table III).
Table II. Respondent demographics (n = 96)
Table III. Participant experience/workplace setting (n = 96)
Therapy intervention
Respondents selected, from a predetermined list, the types of therapy interventions they used in this population group. This question allowed the physiotherapists to indicate all possible interventions they might use, selecting more than 1 possible answer. The results indicate that physiotherapists use a range of interventions, with balance exercises (n = 73, 97%), gait re-education (n = 71, 95%) and proximal control exercises (n = 70, 93%) utilized by the highest number of respondents, as illustrated in Fig. 1. Additional types of treatment reported by the respondents in the “other” category included gym ball (n = 3, 4%), coordination exercises (n = 2, 3%), hippotherapy (n = 2, 3%), rebound therapy (n = 1, 1%), robotics (n = 1, 1%), vocational (n = 1, 1%), vojta (involves the therapeutic use of reflex locomotion; www.vojta.com) (n = 1, 1%), and approximation exercise (n = 1, 1%).
When asked which type of intervention they used most often, 3 intervention types were commonly reported; balance exercises (n = 21, 28%), task-specific training (n = 17, 23%) and proximal control activities (n = 16, 21%). These 3 intervention types were also the most frequently ranked in the therapists “top 3” most effective types of treatment.
Respondents then selected, from a predetermined list of “adjuncts to therapy”, which types they used in this population (multiple responses were possible). The results indicate that physiotherapists use a range of adjuncts, with orthotics (n = 61, 82%), walking/mobility aids (n = 60, 81%) and taping (n = 32, 43%) used most frequently (Fig. 2). Other adjuncts suggested by the respondents included gym ball activities. Orthotics (n = 23, 31%) and walking/mobility aids (n = 23, 31%) were the 2 adjuncts used most often by the therapists, and were also the top 2 adjuncts rated as most effective by the physiotherapists. Treadmill training was ranked as the third most effective adjunct to therapy.
Fig. 1. Types of therapy interventions used.
Fig. 2. Types of adjunct to therapy used.
Virtual training
Fifty-seven percent of respondents (n = 44) reported that they had used virtual training in their practice. The physiotherapists indicated that they had used virtual training most commonly in children with PFTs (n = 32, 73%), acquired brain injury (n = 28, 64%), and traumatic brain injury (n = 27, 61%).
Respondents gave details regarding their top 3 benefits and challenges to using virtual training in their practice, and these answers were thematically analysed. Benefits to using virtual training fell into 3 broad categories; engagement/compliance, physical benefits, and resource/equipment benefits. Engagement/compliance was the most frequently reported benefit, with therapists repeatedly reporting that virtual training was “fun and engaging”, and “games are fun”. Physiotherapists thought that this method of therapy was “patient friendly” and offered a way to achieve “good compliance” whilst being motivational. Therapists noted the potential physical benefits from using virtual training, which included the ability to work on specific problems, such as upper-limb co-ordination and balance. Resource/equipment factors were also reported as a positive aspect, with 2 respondents noting the potential for the technology to “track progress” and that the technology is easily available, with “no additional equipment required”, as children have “access to it at home”.
Challenges to using virtual training were also grouped into similar domains; engagement, physical, and equipment/resources. Therapists were concerned that children might become frustrated if they could not play a game that they had been able to play before they had become ill. One therapist highlighted that virtual training might be “demotivating if difficult”. Physical barriers/challenges were noted, with therapists raising concerns that, if children had visual difficulties or significant mobility problems, this might limit their potential to use this intervention, with one respondent noting that it could be “difficult if child can’t stand”. The most frequent response with regard to challenges to virtual training focused on equipment/resource issues. The responses centred on 2 areas; access to the resource or technical difficulties to using it in this specific population. A therapist reported that it was “not timely to set up” and another therapist reported that “it wasn’t sensitive enough to use”.
Intensity and timing of treatment
The most common frequency of treatment in the inpatient setting was 4–5 times per week (n = 31, 42%). Treatment was typically less intense in the outpatient/community setting, although there was a wide range of responses for this setting, ranging from monthly to up to 4–5 times a week. Physiotherapists also reported that they often intensified treatment at specific time-points, although the reasons for this varied, e.g. immediately post-operatively or post-chemotherapy/radiotherapy. The majority of input was delivered on a 1:1 basis by a physiotherapist, with 89% (n = 64) of physiotherapists reporting that sessions lasted 30–60 min. Respondents were also asked how long (on average) their therapy intervention continued for children with PFTs. There was variation in responses, with a relatively even spread of answers; from less than 3 months to more than 2 years, which reflected the differing needs of this population group.
Aims and outcomes
Physiotherapists reported common aims for physio-therapy treatment, including improving coordination, balance, muscle strength and providing education to the child/family regarding activity (Fig. 3). Other aims identified by the respondents included reducing fatigue and improving participation according to the child’s specific goals. Physiotherapists also indicated that they considered several factors when goal-setting for children, typically involving functional and participation targets. These included child-specific factors (e.g. age, pain levels, fatigue) and disease-related factors (e.g. limitations of disease and treatment).
Fig. 3. Aims of physiotherapy treatment.
Seventy-five percent (n = 52) of physiotherapists (from a total of 69 who responded to this question) reported that they used standardized outcome measures to assess children with PFTs. The most commonly used outcome measure was the Scale for the Assessment and Rating of Ataxia (SARA) (n = 28), followed by the Berg/Paediatric Balance Scale (n = 11) and the Gross Motor Function Measure (n = 8).
Sixty-nine respondents reported frequent problems/challenges that they encountered when treating children following surgical resection of PFT. Three main themes were identified, each with 2 subthemes (Fig. 4). Condition-specific factors included direct medical problems (e.g. the impact of the tumour itself or cerebellar mutism syndrome) or treatment-related issues (e.g. the impact of chemotherapy and radiotherapy, which may include nausea, fatigue or chemotherapy-induced peripheral neuropathy). A number of respondents (n = 9) also commented that fatigue can be exacerbated by the child having to travel to another site for radiotherapy; one physiotherapist commented “during radiotherapy patients have to travel, difficulty planning rehabilitation” and another noted that “children transfer to a different hospital for chemo/radio so disjointed service”.
Fig. 4. Problems/challenges encountered when treating children following surgical management of a posterior fossa tumour.
Physiotherapists also repeatedly reported challenges to rehabilitation in terms of child and family factors, both from an emotional/psychosocial perspective and expectations/engagement (child and parents). Emotional and psychosocial factors arising from the impact of the illness on the child were reported as challenges by the respondents, such as the “loss of friendship groups and social life”. Another physiotherapist noted that “psychosocial issues around functional loss had a huge impact on participation”. However, even if the respondents are aware of the potential psychosocial factors and emotional stresses, they reported that it can still be difficult to manage the child’s and family’s expectations of rehabilitation. The challenge of engaging families in the early stages post-operatively, when the child may be viewed as acutely unwell, was emphasized by therapists, as typified by this response “initially post-op barriers are generally related to family and their views on surgery – families very overprotective with the patients – tend to be slow to get up and move”. In addition, following the acute neurosurgical phase there is then the challenge of continuing to integrate rehabilitation during the child’s oncology treatment, when, again, they might be unwell. One respondent noted the challenge of “parental coping and mental space to think about rehab versus oncology treatment”. This view was supported by another respondent, who noted the “priority of chemo-therapy/radiation versus physical therapy”. Respondents reported that parents commonly regarded rehabilitation as a low priority until after oncological treatment had finished, as “sometimes the parents don’t want the therapists to work with their kids if they are hurting.” Engagement directly with the child was also seen as important to maximize therapy sessions, although this challenge was not reported as frequently as the challenge of working with the families. Therapists noted that some children had difficulty engaging with older staff, as they were “too much like mum, just nagging”, highlighting the importance of rapport-building between the child and the therapist.
The challenge highlighted most frequently by the therapists related to service delivery of therapy input. This is presented in 2 areas; resource factors and lack of evidence. In terms of resource deficits, the area highlighted was physiotherapy staffing levels, with respondents commenting that “staffing (problem), as often need intensive physiotherapy post-surgery and discharged home”. This seemed to be particularly influenced by a perception of pressure to discharge children home quickly, for example, “caseload on a neurosurgical ward – time until discharge to home”, alongside problems with subsequent community/local physiotherapy input on discharge home. One respondent described the challenge as being “district general hospital only with limited therapy; community has variable expertise and staffing”. In addition to staffing requirements, challenges related to space and equipment were also reported, including “limited space and equipment” and “no dedicated rehab team/ward”. In addition to resource issues, the other area that respondents felt directly impacted on physiotherapy input is the lack of evidence for therapy input in this area. This was detailed repeatedly by therapists, who noted the “lack of research” and “limited evidence, especially clinical guidelines”.
The final question of the e-survey asked therapists to document their main reasons for discharging a child from their care. The most common answers were if the child’s goals had been met (n = 50, 71%) or if there was a plateau in physical function (n = 43, 61%).
This study provides a unique contribution to the understanding of current international practice for children with ataxia following surgical resection of PFTs, and presents new data that have not previously been reported. The lack of evidence to guide physiotherapy practice in this area presents a challenge for therapists integrated in a culture of evidenced-based practice. This study provides an insight to current practice, and a foundation on which to base further exploration of this subject.
Over 90 therapists, from 12 countries, completed the e-survey; although the largest cohort was from the UK, there was good representation internationally, particularly across Europe.
The majority of respondents had been qualified for more than 10 years, suggesting a broad range of experience to draw on when answering questions. However, these experienced therapists also reported looking for, but failing to find, postgraduate training opportunities in this field, indicating that therapists may lack opportunities to develop specialist knowledge. Despite the lack of training opportunities, the UK National Institute for Health and Care Excellence (NICE) neuro-oncology guidelines (9) recommend that clinicians involved in this specialist area should have access to training.
Team working
Two thirds of the therapists reported they worked as part of a specialist Neuro-Oncology Rehabilitation Team. Team working is recognized as important in rehabilitation to enable a cohesive approach with children who have many professionals involved in their care (15), and multidisciplinary team working is reported as best practice in the rehabilitation of adults with brain tumours (16). Team working may be particularly important in children with PFT who have multiple transition points in their care, e.g. from neurosurgery to oncology, into community management, and ultimately into late effects follow-up; thus, communication between professionals is essential (17). The presence of such specialist teams provides the basis of expertise, which could help in the formulation of national clinical guidelines, e.g. as seen recently in the development of the UK Stroke in Childhood Clinical Guidelines (18), although clearly developing evidence-based clinical guidelines would be challenging in view of the lack of evidence in this area.
Therapy interventions
Balance exercises, gait re-education and proximal control exercises were the most commonly used interventions reported by respondents. Balance exercises are regularly used in neurorehabilitation, and there is some evidence of effect for adults with ataxia (5, 19), although a lack of evidence in children with PFTs is noted. The use of proximal control was also widely supported, especially in the UK, and although commonly used as a treatment for ataxia, research evidence to support its efficacy is lacking.
Adjuncts to treatment reflected consistent practice across different countries/level of experience, with orthotics and mobility aids reported to be the most commonly used and deemed the most effective by therapists. This is despite there being no specific evidence published on the effectiveness of mobility aids/orthotics in children with PFTs. Further exploration of the type of orthotics used and the aim of this intervention adjunct may be useful in future research to understand the high frequency of their use.
Virtual training
A number of therapists had used virtual training in some format in their practice, most commonly with children with PFTs. The results are also in keeping with recent trials, which demonstrated a trend towards effectiveness when utilizing technology for therapy management of children with ataxia (11, 20, 21). Therapists identified a number of benefits to using virtual training, both in terms of engagement for the children, which was repeatedly mentioned (and is reported in the literature (22)), and potential clinical gains, such as working on co-ordination. The potential impact on co-ordination is supported by a study in children with Down syndrome (23). However, most studies have focused on balance (11, 24, 25), which did not feature significantly in the therapists’ views about the potential benefits of virtual training. Challenges to using virtual training included access to equipment/training requirements, and gaming systems that are not sensitive enough to adapt to specific children’s difficulties. Similar benefits and challenges were reported in Levac’s (26, 27) exploration of clinician’s experiences of virtual reality working with children with acquired brain injury. Therapists were not directly asked which types of virtual training they had utilized, e.g. off-the-shelf or bespoke gaming options, further analysis of which type of virtual training therapists preferred may also be of value in the future.
Intensity of intervention
Commonly, intense in-patient treatment was offered, with intensity reducing following discharge/transition to community settings. There is no specific evidence to support this decision, although workforce structure may be influential. However, there is evidence on the benefit of intense in-patient rehabilitation in the adult brain tumour population, with reports of significant functional gains in the acute rehabilitation process, with the most gain found during the initial inpatient stay (16, 28).
Therapists reported that they commonly intensified therapy treatment at certain time-points, with the immediate post-operative period being the most highly intensive treatment phase, which is reflected by increased input in the inpatient setting. However, they also identified a strong trend of individualizing intensity of therapy input, taking a number of factors into account, such as adjuvant treatment, fatigue and availability of ongoing community services. An individualized approach is recommended in paediatric neuro-rehabilitation for other conditions, e.g. in childhood stroke (18).
Aims/individualized approach
An individualized approach was noted in terms of goal-setting, with therapists being aware of condition-specific factors. Although there is no specific literature to support this in the PFT population, the use of individualized goal-setting is evident in the wider literature on paediatric rehabilitation and, in particular, for children with cerebral palsy, where there is a larger evidence-base (29, 30). The aims of therapy intervention covered the whole International Classification of Functioning Disability and Health (ICF), from those focusing on impairment (e.g. improving balance) to influencing activity (improving fitness) and also considering participation (e.g. assisting with return to sport). Environmental and family factors were also considered in the individualized goal-setting. Three-quarters of therapists reported that they used standardized outcome measures, again highlighting areas of good practice. The SARA (31) was the most commonly used outcome measure, which is encouraging, as its inter-rater reliability and construct validity have been demonstrated in this population group (32). However, the SARA is predominantly an impairment-based outcome measure and activity-based outcome measures, e.g. the PEDI, were less widely used.
Challenges to therapy
This is the first time that physiotherapists’ views across different countries have been explored identifying specific challenges to rehabilitation. Three themes emerged; condition-specific factors, child and family factors, and physiotherapy delivery factors. Therapists frequently reported challenges related to engagement/expectations of parents, particularly balancing rehabilitation post-surgery or when the child might be unwell during radiotherapy/chemotherapy, which is unique to this population group. Jones (33) described the emotional reactions the child and their family may experience during the initial period post-diagnosis, reporting shock, confusion and uncertainty about prognosis, treatment and outcomes. Feelings of helplessness, loss of control and frustration due to lack of information can also impact families’ acceptance of multidisciplinary therapy input (34), and there is no literature to guide practitioners regarding parental expectations of rehabilitation in children with PFTs.
Study limitations
The e-survey tool was piloted, but not formally validated, prior to use, which means that the survey results must be interpreted with some caution. Despite being aware that many people in the target networks were fluent in English, a known limitation is that the survey was only available in English. In addition, snowballing via the special interest groups means that it is not possible to calculate the response rate.
Targeting special interest groups might raise a potential bias, as members of an interest group are potentially more likely to be following best practice, which could be less representative of the whole professional group. However, in order to gain views from therapists who were experienced in the field this was considered the most appropriate source for the sample population. IP addresses were not captured, in order to anonymize the survey and encourage open responses. However, a limitation of this is that, if network connectivity is lost, the responses stop under this IP log-in, and if the respondent logs in again they are counted as a new respondent. The completion rate for the survey (of all surveys started) was 41%, this was influenced by the fact that some questions were not applicable for all therapists to answer; for example, if they had not worked in a particular setting. However, it was noted that there was a slight tail off in responses towards the end of the survey, which could reflect response fatigue due to the length of the survey. A shorter survey with fewer open questions may have achieved a higher completion rate.
Conclusion
This e-survey demonstrates the wide range of intervention types used by therapists. Common adjuncts to treatment included orthotics and walking aids. Broad consensus was noted in terms of treatment intensity in the in-patient setting. Good areas of practice were demonstrated, including multi-disciplinary team rehabilitation and use of individualized treatment planning and standardized outcome measures. This e-survey also makes an important contribution to understanding the challenges involved in rehabilitation in this population group, whilst establishing the foundation for future research into ataxia rehabilitation interventions.
Helen Hartley is funded by a National Institute for Health Research (NIHR), Clinical Doctoral Fellowship for this research.This article presents independent research funded by the National Institute for Health Research (NIHR). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.


 Click to show fullsize
Click to show fullsize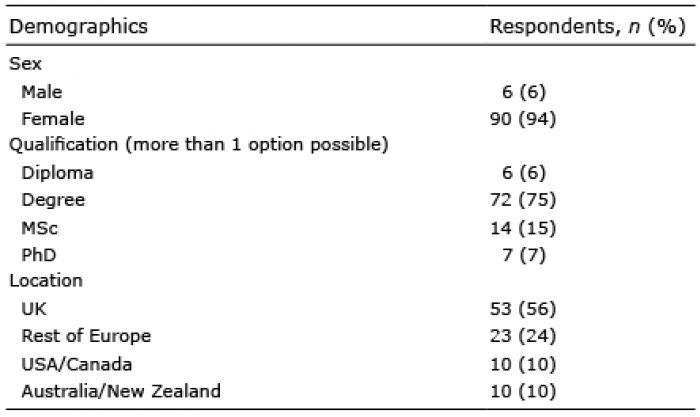 Click to show fullsize
Click to show fullsize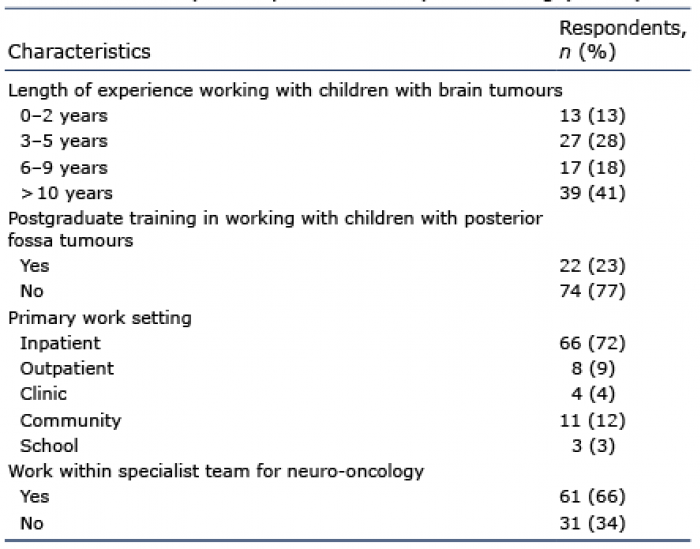 Click to show fullsize
Click to show fullsize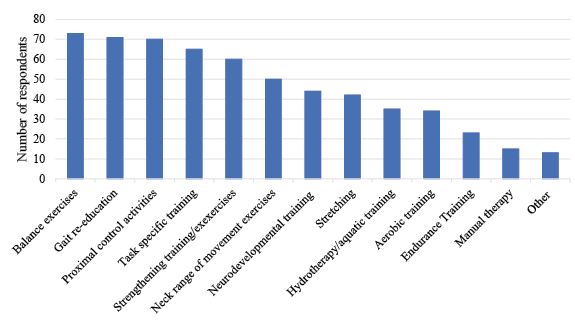 Click to show fullsize
Click to show fullsize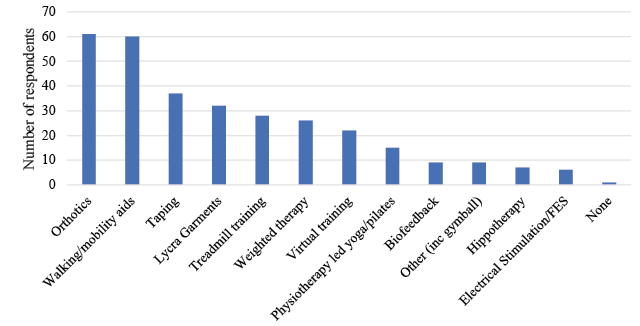 Click to show fullsize
Click to show fullsize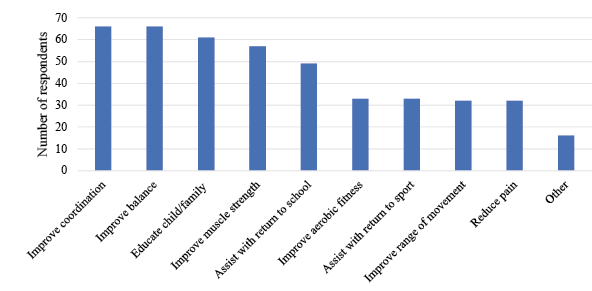 Click to show fullsize
Click to show fullsize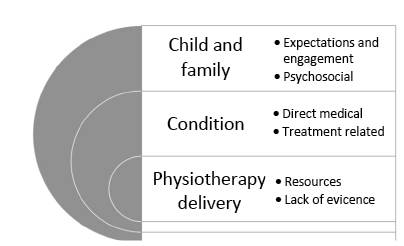 Click to show fullsize
Click to show fullsize