
1Department of Communication Disorders, New Mexico State University, Las Cruces, NM, USA
2National Institute for Empowerment of Persons with Multiple Disabilities, Muttukadu, Tamil Nadu, India
Objective: To assess and describe the involvement of all speech subsystems, including respiration, phonation, articulation, resonance, and prosody, in an individual with cervical spinal cord injury.
Methods: Detailed speech and voice assessment was performed that included Frenchay Dysarthria Assessment, cranial nerve examination, voice (perceptual and instrumental) and nasometric evaluation, and intelligibility and communicative effectiveness.
Results: Impaired respiratory and phonatory control correlated with the physical impairment of C4 and C5 prolapsed intervertebral disc. Cranial nerve examination indicated nerve IX and XI pathology. Phonatory deficits such as imprecise consonants and mild sibilant distortions were apparent. Voice analysis revealed a hoarse, breathy voice with reduced loudness and no problems with resonance. Reading and speaking rate was reduced, and overall a mild reduction in communicative effectiveness was perceived.
Conclusion: Assessment of the speech subsystems produced a comprehensive picture of the patient’s condition and impairments in one or more areas was identified. Treatment options to improve speech outcomes were provided.
Key words: dysarthria; spinal cord injury; speech intelligibility; hoarse voice.
Accepted Oct 15, 2019; Published Nov 12, 2019
JRM-CC 2019; 2: 1000022
Correspondence address: Bijoyaa Mohapatra, PhD, CCC-SLP, Department of Communication Disorders, New Mexico State University, PO Box 30001, NM- 88003-8001 Las Cruces, NM, USA. E-mail: bmohap@nmsu.edu
This article presents information about a patient who had spinal cord injury. He demonstrated reduced speech and voice characteristics in addition to physical impairments. The individual’s speech was evaluated for changes, and prominent characteristics were reported, such as lack of breath support, reduced vocal loudness, hoarseness of the voice, and decreased speech clarity. Speech therapy options were suggested. There is little information in the scientific literature about patients who present significant speech problems after cervical spinal injury. Through presentation of this case study we hope to add valuable information to the clinical and scientific database.
Corpectomy is a procedure for removal of the vertebral disc and end plate above and below a damaged fragment, sparing the anterior and contralateral cortices, while leaving them intact. C4 corpectomy is operated in the cervical region of the spinal cord. In patients undergoing C4 corpectomy, 3–5% of individuals may have spinal or recurrent laryngeal nerve damage leading to denervation to the diaphragm, and muscles involved in respiration and vocal cord movements (1, 2). This population presents with flaccid dysarthria, which accounts for up to 6% of aetiologies of all flaccid dysarthrias (3). The neuromuscular execution deficits associated with flaccid dysarthria due to impairment in respiration following spinal cord injury (SCI) affect a variety of speech components, manifesting as deviations in prosody (reduced loudness), articulation (imprecise consonant production), phonation (abnormally short breath groups and slow inspiration), and vocal quality (breathiness, hyponasality, or roughness) (4, 5).
Despite the global effects that cervical SCI has on respiration and speech, there are limited studies including a comprehensive evaluation of speech characteristics in this population. This is partly due to difficulty in identifying SCI patients who primarily report with speech and breathing problems. Most often, rehabilitation of physical disabilities (tetraplegia) takes precedence over speech difficulties in this population. In addition, there is a relatively low incidence of this condition; in the USA approximately 54 per 1 million people are affected by SCI (6). Therefore, this study was undertaken to expand our knowledge of speech deficits consequent to cervical SCI. The primary aim of this case report is to study the aetiology of the disorder, provide a comprehensive assessment of the various speech subsystems, including respiration, phonation, articulation, resonance and prosody, and suggest speech therapy options.
Symptoms and neurological evaluation
A 58-year-old man reported with an 8-month history of tingling sensation of both upper and lower limbs,
sphincteric disturbances, pain in the back of the neck, and decreased sensation of the lower abdomen for the last 2 months; quadriparesis chronologically involving the right upper limb, right lower limb, left upper limb, and left lower limb for the last 8 months; decreased sensation of the right ring finger, right little finger, and medial side of the right upper limb, followed by involvement of the left upper limb. Neurological examination revealed atrophy in both arms, forearms and hands, atrophy of the calf muscles (bilaterally), and the sensory system below dorsal 6 vertebrae was decreased. His upper limb tone was increased, and lower limb tone was reduced. Electromyographic findings were suggestive of chronic partial denervation. Nerve conduction studies revealed sensorimotor polyneuropathy. Magnetic resonance imaging (MRI) of the brain suggested chronic ischaemic changes in the periventricular and fronto-parietal subcortical regions of both hemispheres, and lacunar infarcts in the right basal ganglion. Spinal cord MRI suggested C4–C5 compressive myelopathy with cord atrophy, C3–C4 posterior disc prolapse causing central canal narrowing, and C4–C5 to C6–C7 neuroforaminal narrowing causing nerve root compression. After comprehensive neurological examination, a diagnosis of C4–C5 prolapsed intervertebral disc was made.
Surgery and in-patient rehabilitation
The patient underwent C4 corpectomy with adjacent discectomy and screwed plate fixation C3–C5 below. Recommendations for physical therapy were given post-surgery. Physical examination revealed hypotonicity in the limbs; voluntary control was relatively preserved in the upper limbs and more affected in the lower limbs. He was non-ambulatory and dependent for activities of daily living. He also presented with hoarseness of the voice and was referred for speech-language pathology consultation.
Speech evaluation
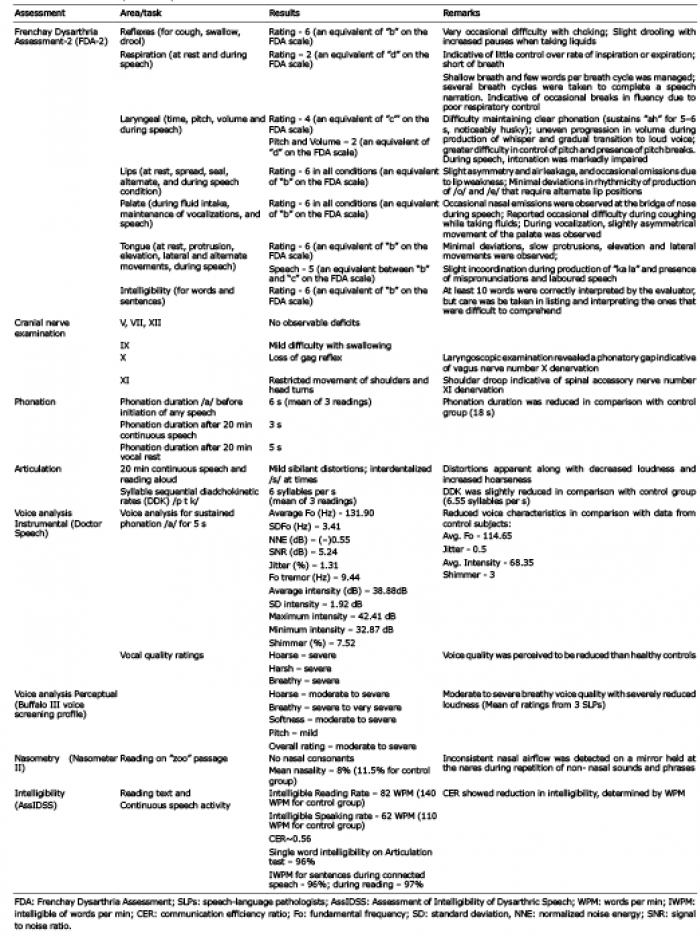
The patient was assessed in quiet surroundings under standard test conditions. He did not use a trusser or neck binder. Detailed analysis of all speech subsystems was conducted. Performance evaluation on each of the subsystems and corresponding tests are presented in Table I. The diagnosis was made as flaccid dysarthria consequent to SCI and recurrent laryngeal nerve damage
Table I. Assessment of speech subsystems
The Frenchay Dysarthria Assessment-2 (FDA-2) was utilized to determine physical functioning of the reflexes, respiratory, laryngeal, and articulatory subsystems, and intelligibility of speech production (7). The FDA ratings (a through e) were transformed into numerical values (8 to 0) for the purpose of numerical interpretation. Each point on the FDA form was denoted as equalling 1, so that a rating of “e” (denoting no functioning) was given a value of zero and a rating of “a” (normal functioning) was given a value of 8. Major deficits were observed in areas of respiration (poor respiratory control) and laryngeal functions (gradual deterioration in voice production). Cranial nerve examination was performed to determine the nerve functioning of cranial nerves V, VII, IX, X, XI and XII, the ones important for speech purposes. Cranial nerves IX and X, in particular, were found to be affected, manifesting as mild problems with swallowing and absence of gag reflex. Ear nose and throat (ENT) consultation was requested, and an indirect laryngoscopic examination revealed less movement and bowing of the left vocal cord during phonation (presence of phonatory gap). The right vocal cord was observed to be compensating. A subsequent MRI procedure revealed mild denervation atrophy of the posterior cricoarytenoid muscle, where atrophy of the posterior cricoarytenoid muscle can be an indicator of recurrent laryngeal nerve palsy (8).
Detailed voice analysis was conducted using Dr Speech Software (Tiger Electronics DRS Inc., Seattle, WA, USA) to assess frequency, intensity, tremors, signals-to-noise ratio and voice quality parameters. Buffalo III voice screening profile (9) was used in favour of the voice parameters on the instrumental analysis. Three experienced speech-language pathologists perceptually rated the subject’s voice on a reading passage task. The patient was instructed to read the passage at his normal speaking rate, selecting a loudness level that was appropriate for conversational speech between 2 people in a quiet room. Major findings were: higher-pitched voice and reduced loudness, and increased cycle-to-cycle variations in fundamental frequency and amplitude.
Nasometric findings were recorded on Nasometer II Model 6400 (Kay Pantex, Lincoln Park, New Jersey, USA) for the Zoo passage (no nasal consonants passage) to determine the presence of nasality. Occasional nasal airflow was observed. Inspiratory capacity was measured on an incentive Spirometer (Hudson RCI, USA) and was found to be reduced.
Based on the idea of the Assessment of Intelligibility of Dysarthric Speech (AssIDSS) (10), a similar assessment was performed in which one experienced speech-language pathologist and another linguist orthographically transcribed the single words on section 8 of the FDA-2, and words and reading passage on an Articulation test for calculations of the percent intelligibility scores. Total speaking rate (words per min; WPM) and intelligible words per min (IWPM) were computed in addition to the communication efficiency ratio (CER), where CER represents the ratio of IWPM to the mean rate of intelligible speech by a group of normal speakers. The normative data was obtained from a control group of 5 subjects in the same age range. CER was found to be reduced in this individual.
The patient presented with dysarthric characteristics, and impairments in the respiratory and laryngeal systems resulting in deviation in prosody and phonation during connected speech. The results are discussed in relation to the physiological subsystems of speech, and interpreted in relation to speech production and impact on intelligibility and communicative effectiveness.
Respiration
The patient presented with reduced respiratory function in the form of shallow decreased length and inspiration, and compensatory breathing strategies in the form of neck and glossopharyngeal breathing and intake of larger volumes with visible chest wall movements. Studies on respiratory function have provided evidence for reduction in vital and total lung capacity, inspiratory pressure, and expiratory pressure in individuals post-SCI (3, 11). This corresponds with the neurological findings of C4–C5 prolapsed intervertebral disc; lesions of C4 and above typically show weakened or absent diaphragm function (12). The patient was found to present with severe prosodic disturbances during connected speech, specifically with regard to rate, phrase length, stress pattern, and/or pitch and loudness variation due to respiratory impairment; the same observations have also been reported in other studies (4, 5, 13).
Phonation
Phonatory deficits, such as reduced volume, breathiness, and softness of voice, were observed. Short phrase length, reduced speech duration, incomplete glottal closure and prosodic abnormalities further added to the phonatory deficits. Similar findings were reported by Hoit et al. in a study of 10 adults with cervical SCI who presented with short phrases and prolonged inspiration that affected prosody; the deficits were attributed to respiratory impairment (5). Respiratory weakness in combination with SCI in flaccid dysarthria is not unusual, but the distinction between phonatory and prosodic abnormalities due to respiratory vs laryngeal weakness can be difficult and is of concern (3). Gasping for air, nares flaring, shoulder elevation, compensatory speech respiration, shortness of breath during speech, as well as other physical activities are some of the distinguishable characteristics associated with phonatory weakness, thereby differentiating it from laryngeal weakness, which is manifested by hoarse or harsh voice, diplophonia, and poor glottal coup compared with cough.
Respiratory and laryngeal subsystems of speech production are closely linked (14), and further investigations in addition to perceptual analysis are required to assess the relative contribution of both systems to speech production in the current case.
Articulation
Articulatory deficits, such as imprecise consonants, although present, was not markedly impaired and can be associated with respiratory disturbances in the absence of significant impairment of the articulators (5).
Resonance
The client showed no major impairments in palatal function. At the connected speech level, he had some nasal air flow for non-nasal sounds, which was detected on a mirror (held at the nares) despite intact velar function. The presence of resonatory disturbances in the absence of impaired velopharyngeal function may be due to the confounding influence of other factors, such as articulatory and phonatory disturbances and configuration of the vocal tract, which has been shown to influence perceptions of nasality (15).
Intelligibility and communicative effectiveness
Although the overall intelligibility of the patient was not severely affected following SCI, his reading and speaking rates were reduced. Research has shown that speech intelligibility is affected by limited respiratory support, reduction in vocal intensity, distributed vocal quality (16) and suprasegmental factors, such as rhythm, poor phonatory control (including intermittent phonation, inappropriate variation of pitch and loudness and excessive variation of intonation), stress patterns, and the rate of speech (17). All of these characteristics were perceived in the current case, suggesting that mild impairments in phonation and prosody in conjunction with mild to moderate respiratory impairments resulted in reduced speech intelligibility and overall communicative effectiveness.
Speech rehabilitation
In developing an effective treatment approach for individuals with SCI, involvement of several professionals from related disciplines needs to be considered. The team members may include doctors, case managers, psychologists, nursing staff, dieticians, physiotherapists, occupational therapists, pharmacists, physical therapists, recreational therapists, speech-language pathologists and/or vocational rehabilitationists. A speech pathologist can incorporate functional therapeutic activities that relate to the subject’s specific deficit areas, by increasing breath support, memory, functional and verbal expression, attention and concentration skills, executive function skills, and providing ongoing education to the subject and/or family.
In the current case, treatment could be focused on increasing breath support. The treatment protocol could include: inspiratory muscle trainer, spirometer for breathing exercises, sustained phonation, sentence recitation, syllable ratio across tasks, diadochokinetic syllable rates, and conversation (3, 18). By increasing vocal intensity and utterance length, the patient would be able to increase his functional communication skills and indirectly enhance health-related quality of life. By improving vital capacity and sustained phonation, he would improve the ability to clear secretion and decrease the risk of pneumonia.
In conclusion, detailed analyses of all speech subsytems will provide us with better understanding of the speech deficits and assist in identifying appropriate interventions to be used in this patient population.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize