
1Division of Physical Medicine & Rehabilitation, Department of Medicine, McMaster University, Hamilton, Canada
2Department of Radiology, McMaster University, Hamilton, Canada
3Division of Plastic Surgery, Department of Surgery, McMaster University, Hamilton, Canada
Objective: To describe a case of nerve kinking correlating with surgical findings in neurogenic thoracic outlet syndrome in a patient with history of brachial neuritis. Thoracic outlet syndrome and brachial neuritis are briefly reviewed.
Case report: A 32-year-old woman with a history of bilateral brachial neuritis presented with paraesthesias in her hand when abducting her shoulder to 45° or higher. A kink in the superior trunk of the brachial plexus, as well as asymmetrically narrowed costoclavicular space, was found on magnetic resonance imaging with the shoulder abducted. Conservative measures failed, leading to partial anterior scalenectomy and neurolysis, which led to improvement in her symptoms.
Conclusion: Anatomical variations in combination with biomechanical changes after brachial neuritis can be associated with neurogenic thoracic outlet syndrome.
Key words: brachial plexus neuritis; thoracic outlet syndrome; electromyography; physiotherapy
Accepted Apr 16, 2020; Published June 15, 2020
JRM-CC 2020; 3: 1000034
Correspondence address: Steven Baker, McMaster University Neuromuscular Clinic, 1200 Main St. W, Hamilton, ON L8N 3Z5, Canada. E-mail: bakersk@mcmaster.ca
Brachial neuritis is a painful condition of a group of nerves in the arm and shoulder, which often occurs spontaneously. This is associated with weakness. A different condition, thoracic outlet syndrome, can also cause problems with the nerves or blood vessels in the arm, due to squeezing on these structures, for a variety of reasons. Our case is of a woman initially presenting with brachial neuritis, who then developed thoracic outlet syndrome during her physiotherapy. The weakness she developed from the brachial neuritis led to abnormal movements of her shoulder, causing the nerves in her arm to be squeezed, and her hand to become numb. She underwent magnetic resonance imaging, showing the nerve was kinked in this area. She eventually had surgery to release the kink, which almost completely resolved her symptoms.
Thoracic outlet syndrome (TOS) is a controversial diagnosis, and is often difficult to make. Contributing factors that may predispose to TOS include the presence of a cervical rib, fibrous bands, hypertrophied muscles, repetitive trauma, or anatomical variants (1). Surgical management is often a last resort after conservative measures fail.
We report here a case of cervical trunk kinking and arm numbness in a young woman with biomechanical changes after brachial neuritis. Magnetic resonance imaging (MRI) evidence of nerve kinking correlated with symptoms of neurogenic thoracic outlet syndrome, which, after failed conservative measures, eventually responded to partial anterior scalenectomy and neurolysis.
A 32-year-old woman was referred to our neuromuscular clinic with a one-year history of bilateral scapular winging, a presumed diagnosis of brachial neuritis, and left arm numbness and paraesthesias with use, which had developed more recently. The brachial neuritis had started approximately 2 weeks after temporomandibular joint surgery, and she presented with severe, bilateral shoulder pain that woke her from sleep. The pain subsided after 2–3 weeks; however, she was left with bilateral weakness and scapular winging. As she started physiotherapy, she developed paraesthesias only in the left arm. Her past medical history included acid reflux and irritable bowel syndrome. Her only medication was gabapentin 600 mg twice daily. She had a magnetic resonance imaging (MRI) of her cervical spine prior to the referral, which was unremarkable.
Her nerve conduction study approximately one year after onset of the brachial neuritis was fairly unremarkable, with borderline low sensory nerve action potentials over the median nerve to the thumb, and ulnar nerve to the fourth and fifth digits on the left. Needle electromyography exam showed 1+ polyphasics and decreased recruitment in the right serratus anterior, but normal studies for the left serratus anterior, trapezius, deltoid, and biceps.
The weakness on her right side improved with time, but worsened on the left. In addition, her paraesthesias worsened, so that when she abducted her left shoulder to 45° or more paraesthesias occurred. She also developed paraesthesias with any pressure over her pectoralis muscles or scalenes, including pressure from wearing a seatbelt, or even tight clothing. The paraesthesias were localized to her hand and forearm, but she had pain more proximally in her shoulder and neck. Now she was also having difficulty performing activities of daily living (ADLs), playing with her young children, and driving, secondary to these symptoms. The working diagnosis at this time was history of bilateral brachial neuritis plus left thoracic outlet syndrome.
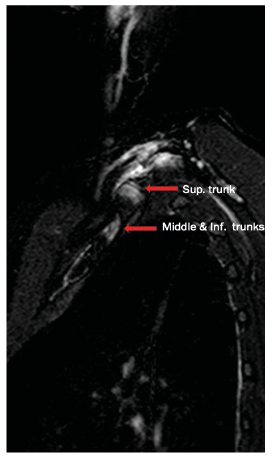
An initial MRI of her left brachial plexus showed increased T2 signal in the C8 root, superior trunk, and posterior cord. Over the next 2 years several treatments were tried, including a course of prednisone, baclofen, and gabapentin, none of which improved her symptoms. A trial of an ultrasound-guided botulinum toxin injection to the left anterior scalene was also undertaken, which provided no benefit. A subsequent MRI of the brachial plexus was ordered, but now with her arm in full abduction. This MRI (Fig. 1) showed that the superior trunk separates from the inferior and middle trunks and takes a 90° turn and kinks as it travels toward the costoclavicular space, where it has mildly elevated T2 signal. It also showed the posterior cord travelling through the proximal costoclavicular space, which is markedly narrowed compared with the other side, and has an increased T2 signal here compared with the arm in the neutral position.
Fig. 1. Sagittal STIR MRI sequence with shoulder abducted showing superior trunk separating from the middle and inferior trunks, and kinking toward the costoclavicular space.
Because of the kinking, as well as the asymmetrically narrowed costoclavicular space, and in the setting of unsuccessful conservative management, surgical management was pursued. A supraclavicular technique was used. A segment of fascia constricting a portion of the brachial plexus was released and a small portion of the anterior scalene was excised. There was no rib removal.
After the operation, the patient’s symptoms improved by at least 80%. She became independent in ADLs, was not taking any medication for neuropathic pain, and was able to drive without problems. She reported ongoing paraesthesias if her arm was held abducted to 150° or with prolonged pressure over her anterior scalenes or pectoralis, but had improved significantly.
Repeat MRI 2.5 years after her operation showed almost complete resolution of the T2 hyperintense signal and thickening of the distal superior trunk and proximal posterior cord of the brachial plexus. The superior trunk of the brachial plexus continued to demonstrate a kink upon shoulder abduction, although it was less conspicuous.
TOS involves compression of the nerves and/or blood vessels through the thoracic outlet in the upper extremity, causing a variety of symptoms (1). It is further categorized into neurogenic, arterial, and vascular (1). Neurogenic TOS symptoms include paraesthesias, weakness, heaviness, as well as neck pain or occipital neuralgia. There are no definitive diagnostic tests, though electromyography and cervical MRI may be helpful in ruling out other diagnoses. Conservative management is first-line management, through physiotherapy, corticosteroids, or injections into the scalenes (1, 2).
If conservative management is not successful, surgical options are considered. There are several techniques for surgical management of TOS (1). In the current patient, a supraclavicular approach was chosen. This approach shows similar functional outcomes, but less post-operative complications, compared with an axillary approach (3).
Brachial neuritis is a condition marked by acute, severe pain in one or both shoulders, followed by a period of weakness, but in which the pain subsides (4). The most commonly affected nerves are the suprascapular, long thoracic, and anterior interosseous (5). Aetiology is often unknown, but can result after an illness or surgery (6). A hereditary form can also exist, although it is less common, and is linked to the SEPT9 gene (6). This was not tested for in this case, as no family members had similar histories. Electrodiagnostic testing is crucial for the diagnosis of brachial neuritis (6), although unfortunately we did not see this patient until she developed paraesthesias of her left upper extremity, almost 1 year after her initial diagnosis. One study showed that the majority of acute electrodiagnostic abnormalities for brachial neuritis resolves at a mean of 12 months (5), which explains why we may not have seen active changes on the left.
In our patient, her initial presentation to another neurologist was typical for bilateral brachial neuritis. However, the delayed onset paraesthesia was not consistent with the time-course for this diagnosis, so an additional diagnosis of left TOS was postulated. While recurrent brachial neuritis has been described (6), it is unlikely in this case given the almost complete resolution of her symptoms after surgical intervention.
Our hypothesis is that with the patient’s history of brachial neuritis, there was already atrophy in the shoulder girdle leading to biomechanical dysfunction, predisposing her to TOS. The association of brachial neuritis contributing to TOS, to our knowledge, has not been described before; however, muscle weakness leading to abnormal shoulder or head position has been described as contributing to TOS (7, 8). It is unclear if the patient also had an underlying anatomical variation with asymmetry in her costoclavicular space or a congenital fibrous band that was not previously known. There was no previous imaging of this area and she had no symptoms prior to the brachial neuritis. Anatomical variations have been known to predispose to TOS (9), though symptoms may only present after an injury (10). In addition, this is the first time a 90° kink in the trunk of the brachial plexus has been described on shoulder-abducted MRI, which was correlated with intra-operative findings. Knowledge of this possibility may be useful for surgeons planning thoracic outlet decompression.
Conclusion
Aetiologies of neurogenic TOS can be complex and multi-factorial. Anatomical variations paired with injuries or mechanical changes, such as weakness or atrophy after brachial neuritis, could predispose individuals to develop symptoms consistent with neurogenic thoracic outlet syndrome that otherwise may have gone unnoticed.


 Click to show fullsize
Click to show fullsize