
1Department of Physiotherapy, F aculty of Health Sciences, Catholic University San Antonio-UCAM, Murcia, Spain
2Optimus Osteopathy and Physiotherapy Clinic, Murcia, Spain
3Tú. Bienestar 360º, Physiotherapy and Medical Center, San Javier, Murcia, Spain
4Department of Basic Psycology and Methodology, Faculty of Psycology, University of Murcia, Murcia, Spain
5Department of Physiotherapy, European University of Madrid, Madrid, Spain
6Real Fundación Victoria Eugenia, Madrid, Spain
7Fishemo CEE, Spanish Federation of Hemophilia, Madrid, Spain
Objective: To verify the safety and effectiveness of manual therapy intervention using fascial therapy in adult patients with haemophilic elbow arthropathy.
Methods: Prospective cohort study. A total of 28 patients with haemophilic elbow arthropathy was recruited in 3 cities in Spain. Patients received onefascial therapy session per week for 3 weeks. The dependent variables were: frequency of joint bleeding, joint pain (visual analogue score) and joint status (Hemophilia Joint Health Score). Outcomes were measured at baseline (T0), post-treatment (T1) and after 3 months’ follow-up (T2). Using Student’s t-test, the means obtained in the evaluations were compared. The analysis of variance (ANOVA) test of repeated measures provided the intra-subject effect. The chosen level of significance was p < 0.05.
Results: A total of 28 patients were recruited according to the selection criteria. No joint bleeding occurred during or after the intervention. The primary outcome, frequency of bleeding, improved after intervention (p <0.001). The secondary variables joint status and joint pain improved after the experimental period (p <0.001). There were significant changes in the repeated measures factor in the frequency of haemarthrosis (F = 20.61; p = 0.00), joint status (F = 64.11; p = 0.00) and perceived pain (F = 33.15; p = 0.00).
Conclusion: Manual therapy using fascial therapy did not produce haemarthrosis in patients with haemophilic elbow arthropathy. Fascial therapy can improve the perception of pain and joint state, maintaining this improvement after a follow-up period of 3 months.
Key words: haemophilic arthropathy; elbow joint; manual
therapy; safety; effectiveness.
Accepted Apr 25, 2020: Published Jun 9, 2020
Jrm-CC 2020; 3: 1000035
Correspondence address: Rubén Cuesta-Barriuso, Real Fundación Victoria Eugenia, Madrid, Spain. E-mail: ruben.cuestab@gmail.com
Haemophilia is a rare disease in which there is a deficiency in some of the blood proteins, which makes it difficult for blood to clot. Patients with haemophilia can present degenerative lesions in joints such as the knee, ankle or elbow, due to joint bleeding, which appears spontaneously with minimal trauma. From an early age, these patients may develop mobility limitations, bleeding, and chronic pain, leading to degenerative damage, known as haemophilic arthropathy. This study examined the safety and efficacy of manual therapy in 28 patients with haemophilia and elbow arthropathy after 3 weeks of treatment. Manual therapy was shown to reduce joint bleeding, improving pain and joint status of the elbow in patients with elbow haemophilic arthropathy.
Haemophilia is a rare congenital coagulopathy characterized by a deficiency of a clotting factor. There are 2 types of haemophilia (A when there is an FVIII deficiency and B when there is an FIX deficiency) and, depending on the blood percentage of the missing factor, there are different bleeding phenotypes: severe (< 1%), moderate (1–5%) or mild (> 5%) (1).
Muscle and, mainly, joint bleeds (haemarthrosis) are the primary clinical manifestations in patients with haemophilia, accounting for as much as 85% of the bleeding events (2). The recurrence of haemarthrosis causes cytokine-mediated inflammatory damage to the target joint (3). In fact, the presence of an annual rate of 2–3 bleeding events in a single joint (target joint) can trigger degenerative structural changes in that joint (4).
Haemophilic arthropathy is characterized by chronic joint pain and destruction, loss of muscle strength, proprioceptive alterations and limitations in the range of joint movement (5). The incidence of arthropathy in the ankle joint is higher in patients with haemophilia under 40 years of age, followed by arthropathy in the elbow and knee joints (6).
The pathophysiological process leading to the destruction of the elbow joint is not entirely clear. Haemophilic arthropathy of the elbow is characterized by hypertrophy of the head of the radius and destruction of the cubitus-humeral joint, leading to significant limitation of elbow mobility and chronic debilitating pain (7). Moreover, the clinical symptoms of haemophilic elbow arthropathy, especially chronic pain, can lead to complications when the patient requires technical aids in activities of daily living (e.g. crutches) and the deterioration affects the joints of the lower limbs (8).
Despite the high prevalence of haemophilic elbow arthropathy in patients with haemophilia, a scarce number of physiotherapy studies have been conducted, aimed at improving joint condition and functionality related to this joint pathology (9, 10).
From a clinical perspective, haemophilic arthropathy resembles other degenerative joint processes, such as those that occur with ageing. Age-related alterations in fascial tissues include connective tissue densification and fibrosis (11), in addition to structural, biochemical, cellular, and functional changes in the extracellular matrix of skeletal muscles that contribute to the deterioration of the mechanical properties (12). Functionally, these pathological changes can modify the composition and properties of fascial tissues and skeletal muscle, thus contributing to the presence of pain, reduced muscle strength or range of motion, which cannot be explained solely by the loss of muscle mass (13), but are characteristic in degenerative joint diseases, also implying basal levels of inflammation, which are expressed especially in the extracellular matrix, affecting immune cell function, which is an important factor for the growth and regeneration of tissues (14).
Fascia is defined as the soft tissue component of the connective tissue system that permeates the human body, forming a continuous 3-dimensional matrix of structural support throughout the body (15). Myofascial release is a physiotherapy technique that consists in applying sustained pressure that aims to reduce fascial system restrictions. The mechanical stimulation promotes reorientation of collagen fibres by improving the quality of movement, circulation of fluids and lymphatic drainage (16). These changes can help improve adhesions caused by processes such as scarring and fibrosis in the body region to be treated. The myofascial induction technique is a manual physiotherapy technique that applies the principles of biomechanical loading of the soft tissue and the modifications of the neural reflexes, through stimulation of the mechanoreceptors in the fascia with the purpose of releasing fascial restrictions and restoring healthy tissue (17).
The main goal of the current study was to assess the safety of fascial therapy intervention in terms of the frequency of elbow haemarthrosis in patients with haemophilia. The secondary aim was to assess the efficacy of this technique for improving joint status and perception of pain in patients with haemophilic elbow arthropathy.
Between March and July 2018 all patients with elbow arthropathy at 3 spanish associations of patients with haemophilia (Valladolid, Galicia and Spanish Federation of Hemophilia) were screened and those who met the following criteria were recruited, as described previously.
Inclusion criteria were: age 18 years or over; diagnosis of congenital coagulopathy (haemophilia A and B or Von Willebrand disease); and medical diagnosis of haemophilic elbow arthropathy (>3 points on the Hemophilia Joint Health Score; HJHS) (18). Exclusion criteria were: patients who were receiving other physiotherapy treatments at the time of the study; patients who had developed elbow haemarthrosis during the study or in the week before the study began; patients who failed to written informed consent of the patient; and unwillingness to follow the study’s protocol requirements.
Volunteers who responded to either the invitation via the social worker of the associations, were assessed for eligibility. These individuals were recruited from 3 spanish associations of patients with haemophilia (Valladolid, Galicia and Spanish Federation of Hemophilia). Patients who had developed antibodies to FVIII or FIX (inhibitors), as well as patients on demand treatment, could also participate in the study.
The G-Power Analysis Program (Gpower version 3.1.9.2; Heinrich-Heine-Universität Düsseldorf, Germany) was used to determine the sample size (α = 0.05 and β = 0.20). Analysis determined that at least 16 patients with haemophilia should be included in the experimental group. One study of manual therapy in patients with haemophilic ankle arthropathy was used as the reference (pain effect size = 0.77) (19). Therefore, this study invited 30 patients to participate in order to allow for drop-outs or failure to meet the selection criteria.
Between January and February 2018, 30 volunteers were screened for eligibility for the study. One of these patients was unable to participate fully for work reasons and failed to attend 2 of the 3 sessions, while another patient declined to participate because of the distance of travel to participate in the intervention.
Intervention
The patients received physiotherapy treatment that consisted of the administration of 3 50-min sessions over 3 consecutive weeks.
The physiotherapy intervention was carried out by a physiotherapist experienced in fascial therapy and in the treatment of patients with haemophilia. Treatment included the application of 7 superficial and 4 deep techniques (Fig. 1 and Fig. 2).
This protocol implied the use of superficial glides on the ventral and dorsal area of both upper limbs, from the scapular waist, as well as of deep and telescopic techniques of the upper limb. The full content of the intervention is shown in https://inhefis.com/protocolo-de-terapia-fascial-en-artropatia-de-codo/.
Fig. 1. Transverse sliding manoeuvre for the biceps brachii muscle. After locating the restriction zones (transversely), compression frictions are performed with separation, performing 2 cycles of 15 transverse frictions.
Fig. 2. Upper limb telescopic manoeuvre. In slight flexion and abduction (10º–15º), a slight traction is generated by dropping the weight of the lower limb for about 5 min (until 3 elongations are felt), following the movement facilitated.
Measures and outcomes
The primary outcome of this study was frequency of bleeding. The bleeding rate in patients with haemophilic arthropathy may be overestimated due to the difficulty of differentiating between pain caused by arthropathy and acute bleeding (20). The principal researcher provided the patients included in the study with a self-report to record any bleeding (joint and muscle) experienced during the intervention or follow-up period. Similarly, telephone follow-up was performed over 48 h following each treatment session to confirm no muscle bleeding or haemarthrosis. This record was used to evaluate the safety of the intervention, in terms of the emergence of muscle and joint bleeding in the treatment area (21).
The secondary outcomes were the change in joint health state evaluated by HJHS 2.1; and the perception of elbow pain measured by visual analogue scale (VAS).
For measurement of joint health state, we used the HJHS 2.1 (18). This scale, which includes 8 items (joint swelling, duration of swelling, muscle atrophy, strength, crepitus on motion, flexion and extension loss, and pain), ranges from 0 to 20 points per joint (the higher the score, the higher the degree of joint deterioration).
The perception of elbow pain was assessed using the VAS, with scores ranging from 0 to 10 (where 0 indicates no pain and 10 the maximum perception of pain reported by the patient). This scale has already been used in the past for the assessment of joint pain in patients with congenital coagulopathies (22).
The baseline evaluation assessed the main independent clinical variables (type, haemophilia severity and treatment, presence of inhibitors and dosage of the pharmacological treatment of clotting concentrates), anthropometric variables (weight, size and body mass index) and sociodemographic variables (age and dominance of upper limbs) of patients recruited in the study.
Three evaluations were carried out: baseline (T0), post-treatment (T1), and after the subsequent 12 weeks without treatment (follow-up; T2). All assessments were carried out by a single physiotherapist, who was experienced in the treatment of patients with haemophilia and other congenital coagulopathies.
Before beginning the study, a pilot study was carried out with the rater and a physiotherapist with more than 20 years of clinical experience to establish the inter-rater reliability of the dependent variable for joint health. This pilot study assessed 5 healthy subjects without joint elbow pathology, while both raters took the measurements under the same conditions and following the same protocol as for patients with haemophilia included in the study. Interobserver reliability for joint health was high, with significant interobserver correlations (p < 0.01) for the score on the right elbow (intraclass correlation coefficient; ICC = 0.94) and left elbow (ICC = 0.93).
Ethical considerations
This study was conducted according to the principles of the Declaration of Helsinki, with approval from the ethics committee of the University of Murcia (ID: 1505/2017). The study was registered before publication in the International Clinical Trials Registry (ClinicalTrials.gov identifier: NCT03009591.
Statistical analysis
The main descriptive statistics (mean, standard deviation and range) of the evaluations carried out in all variables at the beginning of the study have been calculated. Interobserver reliability was calculated using the ICC. The changes between the different evaluations, baseline (T0), post-treatment (T1) and follow-up (T2), were observed using the Students t-test for paired samples. The analysis of variance (ANOVA) test of repeated measures provided the intra-subject effect. The error rate of the significance level was controlled by the Bonferroni correction. When Mauchly’s sphericity test was significant, the Greenhouse-Geisser correction coefficient was used. The partial eta-squared value was calculated as an indicator of effect size (classified as small 0.01, medium 0.06 and large 0.14) (23). To assess clinical relevance, the standard error of measurement (SEM) and minimal detectable change (MDC) for each dependent variable (24) were computed.
The selected level of significance was p < 0.05. An intention-to-treat analysis was used to analyse the results. Statistical analysis was carried out with version 19.0 of the statistical package SPSS for Windows (IBM Company, Armonk, NY, USA).
A total of 28 patients with haemophilia were enrolled in the trial. None of the 28 patients who were finally included in the study dropped out during the intervention or in the follow-up period (Fig. 3).
Fig. 3. Study flow chart. T0: baseline; T1: post-treatment; T2: follow-up assessments.
Table I shows the main descriptive statistics of independent variables at baseline. The median age was 40 years (IQR 15), median height was 174 cm (IQR 13.75), and the median body mass index was 25.67 kg/m2 (IQR 5.04). When analysing sample distribution, significant differences were found in the variables for factor VIII/IX concentrate dosing (median 2,750; IQR 1,000; p = 0.02), haemophilia type and severity, type of treatment, development of inhibitors, and dominance (p < 0.001). No differences were found in the dependent variables at pretreatment assessment (p > 0.05).
Table I. Descriptive characteristics of all patients (n = 28) at baseline of the study
Table II shows the statistics regarding central tendency and dispersion, median and interquartile range, for the dependent variables measured in the study, during the 3 evaluations carried out. No patient experienced elbow haemarthrosis during the treatment period. After treatment global improvement was found in all measured outcomes (p < 0.001). All the measured outcomes remained significantly improved during follow-up assessment in comparison with baseline (p < 0.001). The changes observed following the intervention in joint state on the HJHS scale were found in the items: loss of flexion (p = 0.03), loss of extension (p = 0.04), crepitus (p = 0.02) and perception of joint pain (p = 0.04). The greatest MDC96 for joint pain was 1.66 and 0.97 after treatment and follow-up period, respectively, while the largest MDC96 for frequency of haemarthrosis was 1.08 after treatment.
Table II. Descriptive statistics (median and interquartile range) for the 3 assessments
Table III shows the results of the intra-subject effects test in each of the dependent variables. Significant changes were found in the repeated measures factor. The frequency of elbow haemarthrosis varied depending on the time when it was evaluated [F (1.07, 59.28) = 20.61; p = 0.00; η2p = 0.27]. Likewise, differences were found in joint status [F (2, 110) = 64.11; p = 0.00; η2p = 0.53] and the perception of elbow pain [F (1.24, 68.18) = 33.15; p = 0.00¸ η2p = 0.37].
Table III. Intra-subject analysis in each of the dependent variables
Table IV shows the results of the paired comparison analysis at pretreatment (T0), T1 and T2. Pairwise comparison analysis showed an improvement in terms of frequency of joint bleeding, elbow joint health, and joint pain during the study period. There was a significant improvement (p < 0.001) after the intervention (T0–T1) and at follow-up compared with the baseline value (T0–T2) for all the dependent variables evaluated.
Table IV. Pairwise comparison analysis, means difference and (significance) and minimal detectable change, between the 3 evaluations
The aim of this study was to evaluate the safety and effectiveness of fascial therapy treatment in patients with haemophilic elbow arthropathy. The results support the assumption that a fascial therapy intervention may have a positive effect on the frequency of joint bleeding, joint health and the perception of elbow joint pain in patients with haemophilia. This improvement persisted after the 3-week intervention, until a 3-month follow-up.
Safety in terms of preventing and reducing the frequency of haemarthrosis in patients with haemophilia receiving physiotherapy is essential. The use of strength and proprioception programmes (25, 26) and therapeutic exercise does not appear to cause haemarthrosis (27). Similarly, with the application of manual therapy techniques (10, 19, 21, 28, 29), no haemarthrosis or muscle haematomas have been reported.
Following intervention and follow-up, a significant decrease was found in the frequency of haemarthrosis in both elbows. The fascial system penetrates and surrounds all organs, muscles, bones and nerve fibres, allowing all systems in the treated region to operate in an integrated manner (30). Fascial therapy aims to release the restrictions present in the elbow joint and adjacent structures. These restrictions, typical in haemophilic arthropathy, can affect intra-articular stress, synovial hypertrophy and the compression of periarticular structures, promoting the development of haemarthrosis or microbleeds in the joints. The safety of fascial therapy has been demonstrated in previous articles, where myofascial release techniques were applied to patients with haemophilic ankle arthropathy (21, 29).
In the early stages of joint deterioration, arthroscopic synovectomy or radiosynovectomy may reduce the frequency of joint bleeding. However, when the patient develops a mechanical blockage, these interventions are ineffective. It is in this last stage, where surgical techniques such as the removal of the head of the radius with limited synovectomy can eliminate mechanical blockage, increasing the range of motion of the elbow joint, and preventing chronic irritation. According to the results of this study, the use of a fascial therapy intervention can be a therapeutic alternative to decrease the frequency of haemarthrosis in patients with haemophilic elbow arthropathy prior to surgical interventions resorted to in the later stages of joint deterioration. One of the key factors for the proper development of an active exercise or training programme is the correct execution of the movements required in each of the exercises. An altered movement pattern due to tensions or restrictions in the various muscle or myofascial chains can lead to inadequate or inefficient execution, which can generate or accentuate the patient’s pathological symptoms. The fascia presents a large number of mechanoreceptors, having an active participation in the shaping of movement. A free and competent fascial system helps to shape a suitable neuromuscular pattern for movement, a key aspect in terms of training and performance (31).
The fascial system assists the human body in its vital functions: it ensures the maintenance of posture and motor expression and helps to achieve salutogenic homeostasis (32). Reducing adhesions caused by fibrosis processes through the use of fascial techniques can improve the mobility and function of the treated region, while reducing the intensity of perceived pain (33). The current study found an improvement in joint health in both elbows following intervention and follow-up. These changes in joint health have been described in the ankle joint (21, 29), with flexion and extension movements being 2 of the 8 items of the measuring instrument (HJHS) exhibiting the greatest differences after the intervention.
The use of myofascial release techniques is proposed as a tool to reduce fascial restrictions and restore healthy tissue (17), which may have a potential effect on the perception of pain in the affected region. The results of reduced joint pain in patients with haemophilic elbow arthropathy are consistent with those related to myofascial induction in the approach to neck and lower back pain (34), pain associated with lateral epicondylitis (35) and haemophilic ankle arthropathy (21, 29).
MDC values were calculated for all variables, in order to establish the impact on clinical reasoning when applying a fascial therapy treatment in patients with haemophilic elbow arthropathy. Calculating MDC granted us the opportunity to determine whether the differences revealed were true differences based on the differing methodological approach, or simply the result of a measurement error. According to Pallant (23) partial eta-squared values greater than 0.14 represent large effect sizes. Patients treated with manual therapy showed a high effect size in the studied variables. Although changes in the frequency of elbow bleeds and high effect size were found in the patients included in the study, these results should be analysed with caution. Although the results obtained in this cohort study are positive, we should not evaluate the effectiveness of the intervention beyond the sample recruited in the present study.
Degenerative joint damage and other clinical aspects, such as joint pain or restrictions of periarticular structures, characteristic of haemophilic elbow arthropathy, should be considered when interpreting the results. Using a fascial-therapy-based physiotherapy treatment may thus improve elbow joint bleeding, range of motion and functionality in patients with haemophilic elbow arthropathy. Clinical decision-makers need to be cautious when prescribing physiotherapy treatments based on manual therapy and fascial therapy in patients with haemophilia. Haemophilia patients require individualized management while undergoing physical therapy intervention. Physio-therapy administration requires the physiotherapist’s knowledge of the patient’s bleeding history and the type of pharmacological treatment they receive (prophylactic or on demand). Likewise, it is essential to know the physical effects the patient presents and the characteristic clinical manifestations of muscle or joint bleeding in haemophilia, which might appear as a consequence of manual intervention or therapeutic exercise in patients with haemophilia (36).
Although it is a rare disease, the main limitation of this study is the reduced sample size, even though it is a cohort study in which primarily the safety of the fascial therapy in patients with haemophilic elbow arthropathy is assessed. The use of more objective and accurate measuring instruments is another of the main limitations, which has been compensated by the previous implementation of a pilot study, with an analysis of inter-rater reliability.
The application of a short-duration intervention, only 3 sessions of physiotherapy, pain-free and without the risk of bleeding can favour adherence to physiotherapeutic treatments in patients with haemophilia. Fascial therapy does not require the use of specific instruments or technical means, which favours its application. The fascial therapy protocol disclosed in this project may be an effective alternative in addressing joint health and chronic pain in patients with haemophilic elbow arthropathy.
Addressing chronic diseases requires specific diagnosis, medical or surgical treatment, rehabilitation and follow-up. Healthcare channels should include all the components needed to achieve high-quality health services. Therefore, rehabilitation and physiotherapy treatments should be included as an essential approach in clinical practice guidelines based on scientific evidence (37). Recently, the need for clinical studies of physiotherapy in haemophilia with a larger sample size has been indicated (38). This cohort study is the physiotherapy trial with a greater number of patients with haemophilic arthropathy of the elbow performed to date. A randomized clinical study is needed to confirm the results reported by this study. Designing a study with a larger sample size, meeting the highest methodological quality characteristics (randomization, intent-to-treat analysis, multicentre patient recruitment or blinding of the rater) may endorse the validity of the efficacy results outlined in this study. The large effect size of the improvement of variables such as joint bleeding, elbow pain and joint health is a promising indicator of the efficacy of fascial therapy, and future studies should confirm the findings of this study.
In conclusion, manual therapy through fascial therapy can safely relieve elbow pain and reduce the frequency of joint bleeding in patients with haemophilia and elbow arthropathy. Pain-relieving effect and improvement in elbow joint health status persists for at least 12 weeks after the treatment period. Manual therapy may be clinically beneficial for patients with haemophilic elbow arthropathy. Fascial therapy should be a preferred technique in patients with haemophilia if a trained professional is available.
The authors are especially grateful to the Spanish Federation of Hemophilia, Association Gallega of Hemophilia and the Association of Hemophilia of Valladolid-Palencia for their help in recruiting the sample.
Funding or grants or equipment provided for the project from any source. The authors received the following financial support for the research, authorship, and/or publication of this article: Baxalta US Inc, now part of Shire [Grant ID number: H16-36143]. Baxalta US Inc, now part of Shire had no influence on the research or on the interpretation of data and final conclusions drawn.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize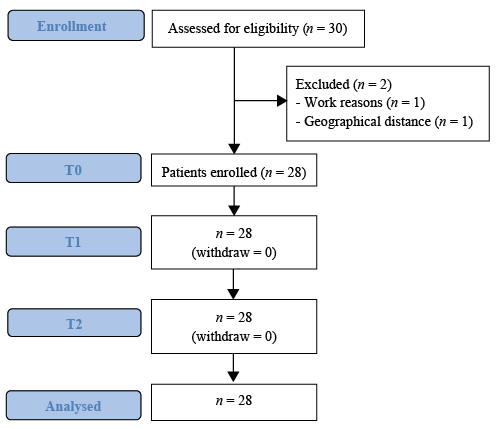 Click to show fullsize
Click to show fullsize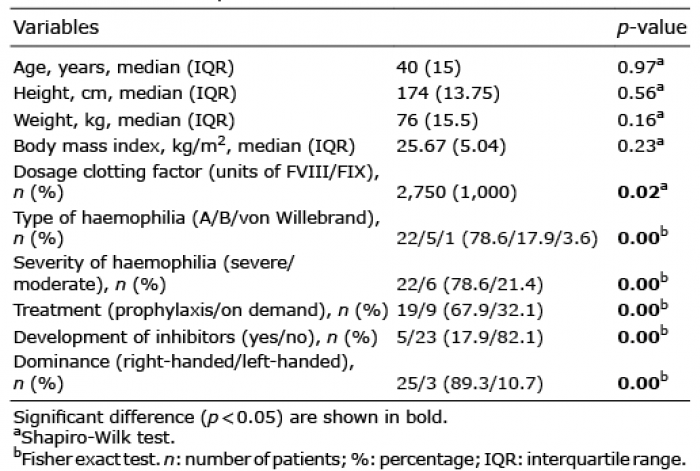 Click to show fullsize
Click to show fullsize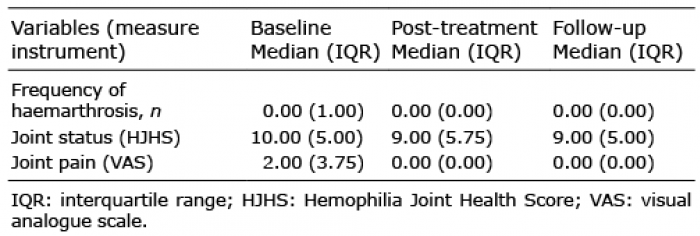 Click to show fullsize
Click to show fullsize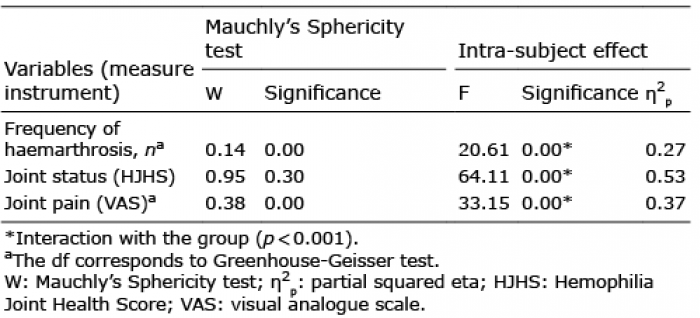 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize