
1Neurogenetics Branch, National Institute of Neurological Disorders and Stroke, NIH, Bethesda, MD, USA
2Clinical Center Department of Rehabilitation Medicine, National Institutes of Health, Bethesda, MD, USA
Introduction: Spinal and bulbar muscular atrophy is a progressive neuromuscular disease that leads to muscle weakness and reduced physical function. Benefits of physical therapy for people with spinal and bulbar muscular atrophy have not been report-ed in the literature.
Case report: A 62-year-old male patient with spinal and bulbar muscular atrophy reported falling, difficulty walking and completing upright tasks, and showed clinical signs of low baseline function on examination. Transportation challenges made it difficult for this patient to attend frequent one-on-one physical therapy sessions.
Interventions and outcomes: A minimally super-vised home-based exercise intervention was chosen with the goal of safely improving his functional capacity. The 5-visit clinical intervention, spread over 10 months, provided 3 exercise modules: seated-to-standing postural alignment and core muscle activation; upright functional and endurance training; and balance training and rhythmic walking. Post-intervention the patient had increased lower extremity muscle strength, improved balance, and reduced self-reported fatigue.
Conclusion: Home-based exercises were well tol-erated with no increase in creatine kinase. Multiple clinical measures of strength and function improved, possibly related to the patients’ excellent motivation and compliance with the programme. Promising utilization of a minimally supervised
home-based programme is described here.
Key words: motor neurone disease; exercise; Kennedy’s disease; spinal and bulbar muscular atrophy.
Accepted Sep 23, 2020; Published Nov 11, 2020
JRM-CC 2020; 3; jrmcc100041
Correspondence address: Joseph A. Shrader, Clinical Center Department of Rehabilitation Medicine, National Institutes of Health, Bethesda, MD, USA. E-mail: jshrader@cc.nih.gov
Doi: 10.2340/20030711-1000041
Spinal and bulbar muscular atrophy (SBMA) is a progressive neuromuscular disease that leads to weakness, frequent falls, and loss of function. The effects of physical therapy for people with SBMA have not been reported. A 62-year-old male patient with SBMA reported difficulty walking and completing standing tasks. Transportation challenges made it difficult for him to attend frequent physical therapy sessions. A minimally supervised, home-based exercise pro-gramme was provided. The programme was spread over 10 months and included 5 in-person therapy sessions and 3 exercise modules: seated-to-standing postural and core muscle strengthening; standing functional and endurance training; and balance and rhythmic walking exercises. Afterwards, the patient had increased leg strength, improved balance, and reduced fatigue, which were measured objectively. The exercise intervention was deemed helpful and safe by the patient and care providers, but required good patient participation, given the minimal supervision provided.
Spinal and bulbar muscular atrophy (SBMA) is an X-linked degenerative neuromuscular disorder caused by trinucleotide CAG repeat expansion in the androgen receptor (AR) gene on the X chromosome (1). Onset of symptoms ranges between 18 and 64 years of age, and typically includes slowly progressive weakness of the extremity and bulbar muscles, as well as balance challenges leading to falls (2). Previously, patients with SBMA and other neuromuscular diseases were ad-vised against exercise due to possible negative effects resulting from induced “overuse weakness”. However, literature reviewed by Krivickas suggests that a wide variety of patients with neuromuscular disease can benefit from exercise prescription that emphasizes flexibility, strengthening, aerobic, and balance (3). Preisler et al. reported an increase of 18% in maximal workload for patients with SBMA on a stationary cycle ergometer over 12 weeks, but found no significant change in VO2 max or improvements in activities of daily living (ADL) (4). Shrader et al. studied home-based functional exercise in patients with SBMA and reported benefits for men with low initial baseline function through post hoc analysis, although there was no significant effect on the primary outcome measure overall (5). The above studies suggest that a 62-year-old patient with SBMA with relatively low functional capacity may benefit from a home-based functional exercise programme.
Genetic testing confirmed the patient’s diagnosis of SBMA with a 47 CAG repeat expansion in the androgen receptor (AR) gene one year before the exercise intervention. The patient provided informed consent as part of NIH protocol NCT00004568. An evaluation showed a history of type II diabetes mellitus, hyperlipidaemia, and depression. The patient described bilateral proximal lower extremity muscle weakness and spasms, and frequent choking on food. He reported difficulty with long-distance ambulation and fear of walking on uneven surfaces. He had a history of falls. The patient described problems with fine motor dexterity skills and sustained activities above the shoulder level, such as hair-washing and overhead reaching. The patient expressed goals of improving functional capacity and confidence in safe community walking.
Initial clinical assessment revealed normal passive upper and lower extremity joint range of motion. Manual muscle testing indicated strength for the right upper extremity as 4–/5 proximally and 4/5 distally, and 4–/5 proximally and distally for the left upper extremity. Strength for the bilat-eral lower extremities were 3/5 proximally and 4–/5 distally. Due to a history of falls and our observation of toe drag, the patient was provided with bilateral non-customized Swedish style ankle-foot orthoses (AFO), and was recommended a structured wide-based shoe for use with the AFO. Based on gait evaluation, the use of a rollator walker was recommended due to high level of fatigue, which he began using at the start of the second clinical visit.
Clinical measures that have been used in SBMA clinical trials were utilized to evaluate the patient’s functional status, including the Adult Myopathy Assessment Tool (AMAT), Timed 2-Minute Walk Test (T2MWT), Quantitative Muscle Assessment (QMA), Fatigue Severity Scale (FSS), and the Berg Balance Scale (BBS). Baseline measures were taken one month before the patient started the first exercise module.
The AMAT categorizes muscle function as mild, moderate, or severely affected, based on performance in a 13-item assessment. Patients are scored on their ability to complete various functional and endurance tasks (6). The cumulative score is derived from functional and endurance subscales; a composite score of 35 and above indicates that a patient is relatively high functioning. Composite scores of 25–34 indicate moderate function, and scores less than or equal to 24 indicate low function. AMAT baseline composite score was 24 for this patient.
The patient completed the T2MWT, which has been used previously in SBMA (2). A baseline measurement of 78 m was achieved, which is 39% of the predicted distance for a person of his age and sex.
QMA was used to measure isometric peak force of bilateral upper and lower extremity muscle groups (AEVERL Medical, LLC, Gainesville, GA, USA) by load cell measurement (Interface, Scottsdale, AZ, USA) with computer-assisted data acquisition. At baseline, maximal voluntary isometric contraction (MVIC) for the bilateral composite upper extremity muscle groups (grip, shoulder abduction, elbow flexion) was 854.5 N, which is 48% of total upper extremity predicted strength (N). The MVIC for bilateral composite lower extremity muscle groups (ankle dorsiflexion/plantarflexion, knee extension, hip extension) was 1,417.5 N, which is 40% of total lower extremity predicted strength. Predicted strength was attained from a normative isometric strength data set that accounts for sex, age, height, weight, and muscle group (7).
The FSS is a 9-part questionnaire in which subjects rate their fatigue level after performing ADL. The lowest score on each question is 1, indicating no fatigue, and the highest is 9, indicating high fatigue. Total scores range from 9 to 63, with a score of 36 and above indicating need for further medical evaluation. At baseline the patient scored 51, indicating that fatigue was a major concern.
The BBS is a 14-item performance-based balance assessment that provides a composite score between 0 and 56, with higher scores indicating better balance. Cut scores have been developed to demonstrate fall risk in elderly community-dwelling people: low fall risk (41–56), medium fall risk (21–40), and high fall risk (0–20). At baseline the patient scored 34.
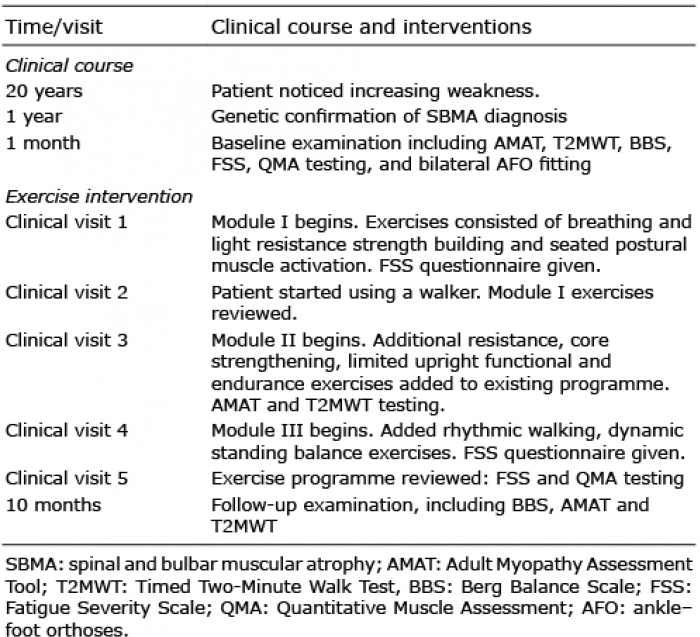
The patient was categorized as having low function compared with other patients with SBMA. Of particular concern was the presentation of 40% predicted lower extremity muscle strength, relatively short walking distance, and medium fall risk. We believed that an upright functional exercise programme that required complex move-ments including lunging (5) would be too challenging for the patient and potentially necessitate frequent visits. As an alternative, a self-directed, home-based exercise programme was used, with five 60–90-min clinical visits for exercise instruction, assessment, and progression (Table I). The patient was instructed to attempt 2 sets of 10 repetitions of each exercise, with a frequency of 3 non-consecutive days per week. The first exercise module began at clinical visit 1, and emphasized seated exercises for core activation and postural alignment. Clinical visit 2 followed one month later for walker mobility assessment. Clinical visit 3 began the second exercise module, involving the addition of upright functional tasks to the existing programme, and AMAT and T2MWT re-assessments. The third and final module began at clinical visit 4 and emphasized rhythmic walking and dynamic balance exercises with the goal of improving gait and balance. The exercise programme took between 45 and 55 min to complete when all modules had been added. The entire exercise programme was reviewed, fatigue was re-assessed, and QMA testing was performed on clinical visit 5. Performance reassessment for the BBS, AMAT, and T2MWT were performed at the end of 10 months.
Table I. Timeline of patient’s clinical course and rehabilitation interventions
The patient completed the intervention reporting full compliance and with no indication of adverse health events or alteration in creatine kinase levels, tested at baseline and 3 months later, with values of 718 and 558 U/L, respectively. Based on these acceptable values (5), and continuous reports of excellent exercise tolerance, we did not consider that further testing was warranted. A total AMAT score improvement of +5 from baseline to the end of the 10 months was observed, including a noted peak score of 31, and +7 improvement during the third clinical visit assessment (Table II). The patient’s improved BBS score of 44 re-categorized him from medium to low fall risk (Table II). A 39-m increase in T2MWT distance by the 10-month reassessment visit was observed. FSS score decreased by 28 points, indicating a reduction in fatigue (Table II). QMA reassessment indicated improved strength in some lower extremity muscle groups, partic-ularly the gastrocnemius and quadriceps, but showed no change in upper extremity muscle groups (Table III).
Table II. Safety biomarkers and reported outcome measures
Table III. Quantitative muscle strength with pre- and post-intervention changes
This case report describes a non-traditional self-directed, home-based exercise programme that led to better than expected results for this patient with SBMA. In addition to the functional improvements, increases in MVIC in the quadriceps and calf muscles were observed (Table III). By the end of the 10 months, the patient had im-proved strength in these 2 muscle groups, which we suggest could have contributed to the improved functional performance observed. Limited SBMA research has provided conflicting results regarding exercise and as a result, such strength improvements were unexpected. The patient may have achieved success with this programme, in part, because of targeted exercise selection, high patient compliance, and a willingness to increase overall physical activity.
The programme began with seated exercises to safely facilitate core muscle control. The AMAT subscale assessment suggests that sit-ups are one of the more challenging tasks for patients with SBMA, indicating trunk muscle weakness (6). To strengthen the core, exercises such as dynamic breathing, torso turns, exercise-band (Theraband)-resisted elbow extension and rowing were selected. In addition, exercises were prescribed to target the lower extremity muscle groups, in particular the quadri-ceps and gastrocnemius, as these muscle groups are affected more frequently in SBMA (2). Seated long-arc quad extensions show evidence of a positive correlation between quadriceps strength, balance improvement, and functional ability (8). Long-arc knee extension exercises were selected to help strengthen the patient’s quadriceps, along with bilateral heel raises, which have been shown to be a useful exercise for preventing falls, building stability, and improving functional movement by enhancing postural control (9). Furthermore, repeated heel raises were seen as one of the more difficult AMAT tasks, highlighting the level of distal weakness in patients with SBMA (6).
Exercises that focused on upright functional tasks were added to the programme during clinical visit 3. Repeated sit-to-stands were included as one of the first additions for the second module for its capacity to predict function-al ability. Eriksrud & Bohannon discussed a positive relationship between increased knee extension force and sit-to-stand performance (10), highlighting the potential benefit that seated long arc quad extensions and repeated sit-to-stands may have had with this patient’s increased bilateral knee extensor strength. The patient’s bilateral hip extension was 20% less than that found in a previous SBMA cohort (2). Standing hip extensions were selected to strengthen the gluteal muscles, but improved peak hip strength was not observed by the end of the 10 months. Despite no shoulder strength improvement from selected exercises such as upright rows, overall shoulder function-al and endurance AMAT subscale scores increased for the modified push-up and arm-raise tasks.
The addition of rhythmic and dynamic movement exercises for the third module was important for achieving the patient’s gait and balance goals. Anterior/posterior rocking with eyes open while on a soft pad was selected to increase postural control demand due to the reduction of sensory information in SBMA (2). To further challenge his limits of stability and reduce fall risk, the patient was coached in the clinical setting to safely exceed the backward limit of stability and practice a rapid backwards step to prevent falling backwards. These exercises may have helped increase the patients’ confidence and safety while walking.
Physical therapy care has been traditionally delivered face-to-face, but recent world events have increased the need for remote interventions via telehealth. Our group previously studied home exercises in people with SBMA, utilizing video cameras to verify exercise compliance and safety (5). However, these resources were not avail-able for this case and we relied on patient self-report of exercise tolerance and compliance. We initially discussed reduced monitoring with the patient, explaining that programme success would rely on his compliance and timely reporting of any adverse events, to which he agreed. He received one-on-one exercise demonstrations, with a minimum of 45 min of guided patient performance to assure he was proficient with all techniques. Regular travel to and from physical therapy clinics can be time-consuming, and exhausting for individuals with low base-line function, possibly leading to reduced participation. Home-based exercises that target objective impairments and match intensity to functional abilities may improve both exercise compliance and safety for people with SBMA. However, safe execution of upright tasks remains crucial, given the high risk of falls in this population. Additional suggestions, not utilized in this case, may include providing clinical training to caregivers to assist with home exercises and incorporating real-time video supervision, and wearable physical activity monitors. Supervised aquatic exercise, such as water walking, is also commonly recommended. Research is needed to help guide future advancements.
This self-directed home-based approach to therapy may not be suitable for many men with SBMA and low func-tion. In this case, it was necessary to implement this type of programme due to the patient’s infrequent availability for one-on-one clinical sessions. It is important to ac-knowledge that case studies do not provide cause-effect relationship evidence. However, QMA results showed increased strength in the quadriceps and gastrocnemius muscles, and a 5-point increase in total AMAT score highlighted an increase in functional capacity. The patient reported increasing confidence with upright activities throughout the intervention, which may have been an important motivating factor to continue the self-directed programme. He reported that regaining his ability to walk around a nearby lake with his son was meaningful. Although exercises, as discussed in this case, are recommended to be performed with clinical guidance, the results show improvement in this patient’s overall function and promise for the consideration of minimally supervised home-based exercise programming for men with SBMA.
Funding. This work was supported by intramural research funds from the National Institute of Neurological Disorders and Stroke and the National Institutes of Health Clinical Center, Bethesda, Maryland, USA.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize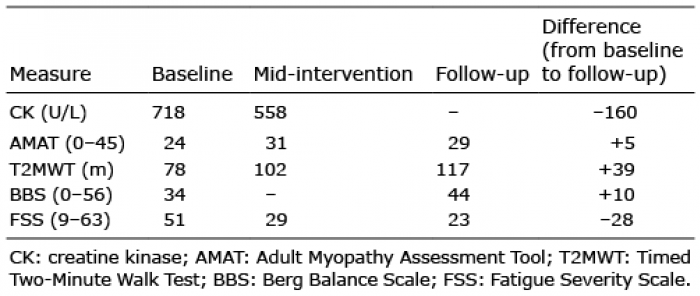 Click to show fullsize
Click to show fullsize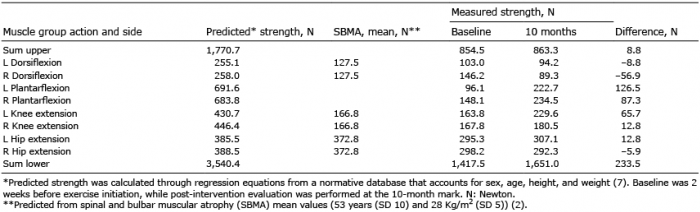 Click to show fullsize
Click to show fullsize