
1Department of Nephrology, China Medical University Hospital, Taichung, Taiwan, ROC
2Department of Medicine, China Medical University, Taichung, Taichung, Taiwan, ROC
3Department of Physical Therapy and Graduate Institute of Rehabilitation Science, China Medical University, Taichung, Taiwan, ROC
Objective: To evaluate the effect of whole-body vibration training on working-age people on haemodialysis.
Design: Consecutive case series study.
Subjects: Seventeen working-age participants on maintenance haemodialysis were enrolled.
Methods: A 12-week whole-body vibration training programme, including different postures, was designed. The study evaluated and compared physical fitness, including a list of tests such as the 5-repetition sit-to-stand test, hand grip test, 2-min step test, and 8-foot up-and-go test; modified Berg balance scale; static and dynamic balance function; and quality of life, using a quality of life questionnaire before and after the training.
Results: All physical fitness parameters, except grip strength on the left side, improved after whole-body vibration training. For balance, the modified Berg balance scale demonstrated enhanced scores for equilibrium, with eyes closed on a stable surface and eyes open on an unstable surface, and movement velocity under the fast condition along the left and right directions (p=0.011). No significant improvements in quality of life were found.
Conclusion: Whole-body vibration exercise training enhanced physical fitness and static and dynamic balance control in working-age participants on haemodialysis.
Key words: renal dialysis; exercise; physical fitness; working age; whole-body vibration.
Accepted Nov 26, 2020; Published Jan 14, 2021
JRM-CC 2021; 4: jrmcc00046
Correspondence address: Chia-Ming Chang, E-mail: cmchang.cliff@gmail.com; Hsiu-Chen Lin, Department of Physical Therapy and Graduate Institute of Rehabilitation Science, China Medical University, Taichung 404, Taiwan, ROC. E-mail: hclin@mail.cmu.edu.tw
Doi: 10.2340/20030711-1000045
This study designed a series of exercises in different postures on a whole-body vibration machine for individuals on maintenance haemodialysis and evaluated the changes in their physical fitness, postural control and quality of life before and after a 12-week programme. Seventeen working-age participants on maintenance haemodialysis were enrolled and completed the whole-body vibration training programme. There were no significant changes in the scores on the quality of life questionnaire for multifactorial aspects. However, the physical fitness parameters, including a list of tests, such as the 5-repetition sit-to-stand test, hand grip test of right side, 2-min step test and 8-foot up-and-go test, improved after the whole-body vibration training. Their postural control also demonstrated improvements in the modified Berg balance scale, equilibrium scores with eyes closed on a stable surface and eyes open on an unstable surface, and movement velocity under the fast condition along the left and right directions.
End-stage renal disease (ESRD) generally occurs in older people; however, approximately half of such patients (49.0%) are aged between 20 and 65 years (1). ESRD patients on maintenance dialysis have poorer physical fitness function than their age-matched counterparts (2). These functional differences between populations are associated with exercise intolerance, frailty, falls, premature death, and unemployment (3–6). Subjective and objective limitations of physical fitness can also be observed in high-functioning people on dialysis (7).
A previous study found that exercise training benefitted patients with ESRD, in improving health-related quality of life (QoL) by enhancing psychological well-being and physical functioning (8). Whole-body vibration (WBV) training is a new form of exercise training that shown to be safe in patients with cerebral palsy (9), has become increasingly popular, and has been reported to exert beneficial effects on muscular performance, bone mineral density, postural control, functional mobility, and sensorimotor function in various populations, including elderly people, and in patients with Parkinson’s disease, degenerative disease, and other chronic diseases (10–14).
Unfortunately, studies investigating the effects of WBV training on patients on dialysis are limited, and these studies have enrolled elderly people and not those of working age. Seefried et al. reported the safety and feasibility of WBV training, designed as 2 sessions per week for 12 weeks, in 45–74-year-old people on dialysis (mean age 59 years) (15). They demonstrated an improvement in the total score on short physical performance battery tests that assess physical function. Doyle et al. conducted an 8-week WBV exercise training programme, thrice a week for 3 min, in dialysis patients (24–92 years; mean age 65 years); a wide age range was maintained in this study. Their results showed improved functional performance on the 60-s sit-to-stand (STS-60) test and several QoL domains (15).
Employment plays a crucial role in the QoL of working-age people on dialysis. However, the effects of WBV training on employment-related ability, physical fitness, and balance (2, 16) in this population remain unclear. Therefore, this study investigated the effects of a WBV training programme on physical fitness, balance, and QoL of working-age people on dialysis.
Study design
This was a prospective, open-label, non-randomized, single- centre exploratory study. The following baseline evaluations were performed for all patients: basic data, physical examination, physical fitness evaluations, and balance function evaluations. The patients then underwent a training programme for 30 min per session, thrice a week for 12 weeks. The tests performed at baseline evaluation were repeated after programme completion. This protocol was approved by the Institutional Review Board of China Medical University Hospital, Taichung, Taiwan (DMR101-IRB1-174).
Participants
The paticipants were screened and recruited from the out patient clinic of the Department of Nephrology in the China Medical University Hospital. The inclusion criteria were: (i) age between 18 and 65 years (working age), (ii) ability to walk independently, and (iii) receiving maintenance haemodialysis (HD) thrice a week for more than 3 months in an outpatient dialysis unit. Patients who were pregnant or had recent fractures or surgery, impaired consciousness, severe arthropathy, cerebrovascular disease, or cardiovascular episodes within 6 months were excluded. With the use of G-Power software, the sample size was estimated, based on the results of our pilot study with an effect size of 0.72, α = 0.05, and power = 0.8. The minimum sample size required was 14 participants.
Intervention
The participants visited our exercise room (The execise room locates in two floor higher of the same building with their haemodialysis room, and it is belonged to Department of Physical Therapy, China Medical University) before their routine HD session. Their blood pressure, heart rate, and respiratory rate were measured for safety before and after the training session and were used by a trained therapist to adjust the progression of WBV exercise. A 4–5-min light aerobic warm-up exercise was administered by a trained therapist. The patients then stood on a vertical vibration platform (Zen Pro® TVR-3900, Tonic Fitness Technology, Inc., Taiwan) to perform WBV exercise for a maximum of 30 min. The platform vibrated the entire time, while the participants performed squats, deep squats, wide-stance squats, toe stands, 1-legged squats, and lunges (Fig. 1). For safety, a suspension system was used to prevent falling during the WBV exercise. Training intensity was increased gradually according to the overload principle from static to dynamic, both legs to 1-legged stance, and eyes open to eyes closed (17). The vibration parameters were: vibration frequency progressing from 30 to 50 Hz, vibration amplitude up to 1.5 mm. Each exercise posture lasted 3 repetitions from 30 to 45 s with a resting interval of 20–30 s. After WBV exercise, 5–10 min of static stretching exercises was performed for cooling down. The participants who underwent at least 30 of the total 36 training sessions (above 80% attendance rate) were included in the analysis.
Fig. 1. Whole-body vibration (WBV) exercise on a vertical vibration platform. For safety, a suspension system was used to prevent falling.
Outcomes
Physical fitness. Four physical fitness evaluations were used; the 5-repetition (rep) sit-to-stand test; hand grip test; 2-min step test (2MST); and 8-foot up-and-go test. In the 5-rep sit-to-stand test, the participant was instructed to stand up and then sit back down from a standard chair as quickly as possible with their arms folded across their chest. This measured their leg strength. The time required by the participant to perform the 5-rep sit-to-stand test was recorded (18). In the hand grip test, the participants squeezed the dynamometer with maximum isometric effort for approximately 5 s. The maximal measured grip strength (kg) from 3 trials was recorded. The 2MST was used to measure aerobic endurance as an alternative to the 6-min walk test (6MWT). The participant stood up straight next to a wall, and the level corresponding to midway between the patella and iliac crest was marked on the wall using a tape. The participant then marched in place, lifting the knees to the height of the tape as many times as possible. The total number of times the right knee reached the tape level in 2 min was recorded (18). The 8-foot up-and-go test represents speed, agility, and balance while moving. The participant was seated on a standard chair. On the command “Go”, they were asked to stand, walk to the cone positioned 8 feet ahead, and then return to sit down in the chair, as quickly as possible. The time from “Go” to sitting back in the chair was recorded (18).
Balance function. The modified Berg balance scale and computerized dynamic posturography (CDP) system (PRO Balance Master, Neurocom, USA) were used to evaluate the participants’ static and dynamic balance function.
Static postural stability was measured using the sensory organization test (SOT) with different levels of challenges. The following testing conditions were used, from easy to difficult: SOT1 was performed with eyes open on a stable surface, with all sensory inputs; SOT2 was performed with eyes closed on a stable surface, with blocked vision; SOT4 was performed with eyes open on an unstable surface, with a disturbed somatosensory input; and SOT5 was performed with eyes closed on an unstable surface, with blocked vision and a disturbed somatosensory input.
Equilibrium scores (EQSs) calculated in each condition represented how (ranging from 0 to 100) the participants controlled body sway.
Dynamic postural control was examined through the limits of stability (LOS) and rhythmic weight shifting (RWS) tests in the CDP system. The LOS test evaluated the reaction and motor control ability to voluntarily move the body’s centre of gravity (COG). The outcome measures included the reaction time (RT), movement velocity (MVL), endpoint excursion (EPE), maximum excursion (MXE), and directional control (DCL). The RWS test assessed the ability to sway the body’s COG in the frontal (left and right) and sagittal (forward and backward) planes with 3 paces (slow, moderate, and fast). The on-axis MVL and DCL were calculated in this test.
Quality of life. QoL was assessed using the 36-Item Short Form Health Survey (SF-36) questionnaire. The SF-36 contains 8 domains, namely physical functioning, role limitations due to physical health and emotional problems, energy/fatigue, emotional well-being, social functioning, pain, and general health.
Statistical analysis
The normality of all the variables was tested first using the Shapiro–Wilk test. If the distribution of the variable did not fit the normal distribution, the Wilcoxon signed-rank test was used to compare the difference before and after the WBV exercise intervention. Otherwise, the paired sample Student t-test was used. All statistical analyses were performed using SPSS 12 (SPSS Inc., Chicago, IL, USA), and the significance level was set at 0.05.
Of the 120 participants on maintenance HD who met the inclusion criteria, 23 signed informed consent to join the current study. Six of them did not complete the exercise programme, due to insufficient time, kidney transplantation, or surgery of the lower limbs. Finally, 17 (73.9%) participants were enrolled in the study. Their demographic data are shown in Table I.
Table I. Demographic data of participants on haemodialysis
Physical fitness
Following the 12-week intervention, all fitness variables, except the grip strength on the left side, exhibited significant improvements in performance (Fig. 2).
Fig. 2. Effects of the 12-week whole-body vibration (WBV) exercise programme on physical fitness. (A) 5-rep sit-to-stand test, and 8-foot up-and-go test; (B) bilateral hand grip test; (C) 2-min step test.
Balance function
The results of balance functions are presented in Table II and Table III. Significant improvements were observed in the modified Berg balance scores after training (Table II). The participants also exhibited improvements with significantly higher EQSs under SOT2 and SOT4 conditions (Fig. 3).
Table II. Effects of whole-body vibration (WBV) training on scores of the modified Berg balance scale, limits of stability (LOS), and rhythmic weight shifting (RWS)
Table III. Quality of life questionnaire (Short-Form 36; SF-36) for participants on haemodialysis before and after the whole-body vibration (WBV) exercise programme
Fig. 3. Effects of whole-body vibration (WBV) training on static postural stability. EC: eye close; EO: eye open. The y-axis of fig 3 reprents the ”equilibrium score (EQS, %)” of the sensory organization test (SOT).
The RT, MVL, EPE, MXE, and DCL in the LOS test did not change significantly (Table II). For the RWS test, the training effects on MVL and DCL in both directions exhibited no significant differences, except for movement velocity in the left and right directions under the fast condition, which increased after training (Table II).
Quality of life
There were no statistically differences in the SF-36 questionnaire between baseline and after 12 weeks in all domains (Table III).
This study focused on the training effects of the 12-week WBV programme for working-age people on dialysis. Significant improvements were measured in physical fitness variables after the 12-week WBV programme. Improvements were also observed in the static and several dynamic balance variables.
This study demonstrated significant improvements in all physical fitness evaluations, and these results may represent enhancement of leg strength, hand grip, aerobic endurance, and coordination after training. Doyle et al. also reported improvements in physical fitness variables in the STS-60 test (15). Although the reason might be the focus on safety and feasibility, the amount of exercise might be inadequate to result in a significant improvement. Seefried et al. gradually extended the training time, from 5 to 20 min, during 12 weeks, and showed a trend of improvement in the balance test, physical performance, and skeletal muscle index, although without statistical significance (19). In the current study, after performing a 30-min exercise session, positive effects were observed on all the physical fitness variables. On the basis of the aforementioned descriptions, the time for a WBV exercise session might be a vital factor determining the effect of intervention. However, the minimal effective session time and WBV training intensity had not been established. A systematic review of 16 randomized controlled trials exhibited different training results with various dosages; these studies featured the session time, ranging from 1 to 30 min, the study duration ranging from 4 weeks to one year, and the number of training sessions, ranging from 16 to 730 (10). Additional studies may be required to estimate the minimal dose. Another possible reason for the discrepancy in our results might be our focus on the working age and relatively young participants on dialysis who might present favourable resilience.
Patients on HD demonstrated poorer postural control than did age-matched healthy people, in particular during quiet standing with a cognitive task (20), which might result in a high risk of falls. The fall rate of patients who either was the resident of a supported accommodation or not is 1.18–1.60 falls/ year, (21, 22) which is higher than that elderly people living in their own homes (23). In addition to myopathy, deficits might be observed in integrating visual, proprioceptive, and vestibular inputs necessary for efficient postural control (24, 25). Studies have demonstrated only improving trends in balance tests (15); the participants in the current study demonstrated significant improvements in moderate to challenging tasks in static balance tests and specific variables in dynamic balance tests after WBV training. The mechanisms through which WBV acted on motor control are not fully understood. Vibration applied to the musculotendinous system can elicit reflex muscle contractions and affect sensory processing. Further effects of vibration included modifications of tracking movements, increased postural sway, and gait modifications (26).
This study exhibited benefits from WBV training in both static and dynamic balance functions, as determined using detailed balance evaluations. In static balance tests, improvements were observed under SOT2 and SOT4 conditions for moderate to challenging tasks; however, no statistically significant changes were observed under simple (SOT1) and difficult (SOT5) conditions. The lack of changes under SOT1 might be attributed to the already good EQS of our participants before training and the limited improvement space. Under the eyes closed condition on an unstable surface, the EQS was relatively low, indicating the need for further training for improvement.
For the evaluation of dynamic balance, the LOS test is crucial and reliable to represent the ability to control the movement of the body’s COG (27). However, the participants in the current study did not exhibit significant improvements in the outcome measures of the LOS test. Studies evaluating the WBV effect on dynamic balance tests are limited. Cheung et al. reported improvements in MVL, MXE, and DCL after WBV training in elderly women (28), whereas Torvinen et al. (28, 29) found that WBV training had no effects on balance function. These discrepancies could be explained by individual differences in participants, administered doses, and controlling status. The participants in the studies by Torvinen et al. (28, 29) were young, healthy volunteers, which implied that young people with relatively good muscle strength may not readily gain additional benefits from WBV (29, 30). However, this observation does not rule out the efficacy of WBV on young people. Two studies have reported that WBV training increased flexibility, strength, and directional control, especially in the left–right direction, in the LOS and RWS tests in young athletes (31, 32).
For the RWS test, improvements were observed only in fast MVL in both directions. Most participants could shift their body COG to match up with the moving cursor on the screen under the slow- or medium-speed conditions. The MVL we used are comparable with ideal velocities in the manufacturer’s manual. However, under fast conditions, the participants would experience trouble catching up with the moving cursor before the training, with 79.4% ideal velocity in the left–right direction and 68.4% ideal velocity in the forward–backward direction. After programme completion, they performed better than previously, to catch up with the ideal velocity (88.8% and 73.6% ideal velocity in the left–right and forward–backward directions, respectively). This result implies that WBV training benefited the participants’ movement control under the fast condition. A similar study on older women demonstrated that WBV training improved leg strength and speed of movement (17).
Inconsistent changes in QoL were observed in some studies after WBV training in participants on dialysis (15, 33). No significant changes in QoL were observed, possibly because of the comorbidity and complexity that would affect the feeling of well-being in the participants on dialysis. Another explanation could be the small sample size with considerable variability, which reduced the statistical power of this study.
WBV exercise training is safe and has been performed in various frail populations (9–12, 15, 34, 35). In the current study, participants did not experience any severe or adverse effects during the 12-week training. The 73.9% completion rate was acceptable in this group of participants. Several modes of exercise training for participants on dialysis included aerobic exercise, resistance exercise, and combination in the literature. However, patients with ESRD conventionally exhibit a high non-adherence level to medical regimens and exercise (36, 37). Most exercise training studies focusing on participants on HD have used single-exercise modes, such as cycle ergometer, walking, or tai chi. However, prolonged repetitions of the same exercise might be considered boring for participants and reduce their adherence. In this study, WBV training was selected, not only because of its increasing popularity, but also because of its novelty to the participants. It is also considered a relatively passive facilitation of muscular activation that simultaneously poses a constant challenge to postural stability, which may be suitable for these participants. Using an appropriate design in the 30-min sessions, it is possible to achieve a favourable adherence in these participants and therefore encourage the promotion of continuance of exercise training.
Another particular focus of this study is young participants on dialysis. A rehabilitation study investigating patients on dialysis focused on the entire population or elderly people (38). The resilience of young patients on dialysis has seldom been mentioned. This study provided different results, demonstrating that WBV exercise significantly improved participants’ physical fitness and static and dynamic balance. We consider that age might be a factor; young people exhibit better functional recovery in rehabilitation after stroke and amputation (39–41). However, studies on the rehabilitation of young patients on dialysis and comparison of the effects of rehabilitation on different age groups of people on dialysis are required to support this assumption.
Study limitations
This study has some limitations. There was no control group. Most participants on maintenance HD would have barriers to exercise participation, and the physical function and health-related QoL of non-exercising participants on HD either did not change or declined over the period of the intervention (33, 37). Therefore, the status before the intervention was used as the baseline comparison. Secondly, the sample size is relatively small, which might reduce the power of certain study end-points. The fitness variables improved significantly; however, only certain changes in balance variables could be observed. We are especially interested in difficult tasks, such as SOT5, which present a large variance. Thirdly, the suspension system used to prevent the participants from falling might not be available in other facilities, which limits the generalization of WBV training. Although WBV training is safe, and no other studies have used such protective devices, we recommend using protective devices, at least at the start of training.
Conclusion
This study demonstrated the beneficial effects of WBV exercise training on physical fitness and static and dynamic balance control in participants on maintenance HD. The study also showed that WBV exercise can be a practical and effective training tool for young people on dialysis. This information may provide the basis for further advice and care in rehabilitation of young people on dialysis.
This study was supported by the National Science Council (NSC99-2314-B-039-015-MY3) and China Medical University (CMU101-S-34).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize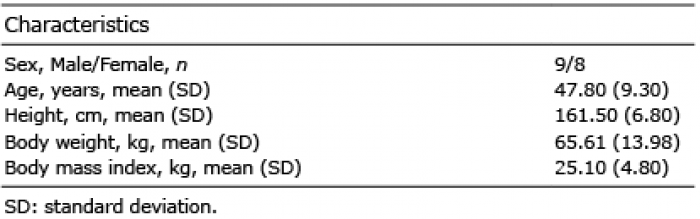 Click to show fullsize
Click to show fullsize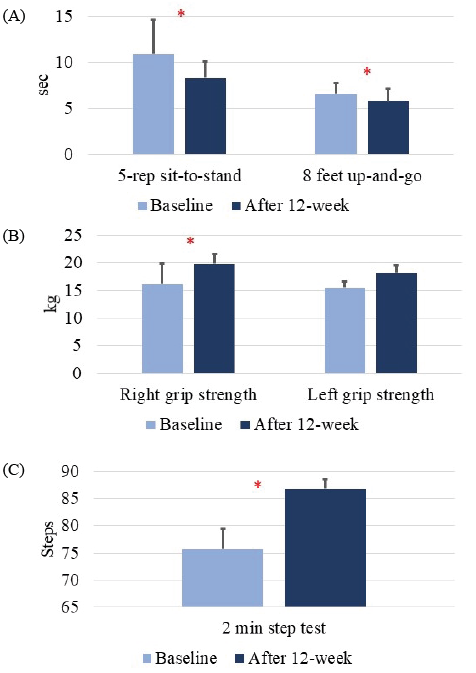 Click to show fullsize
Click to show fullsize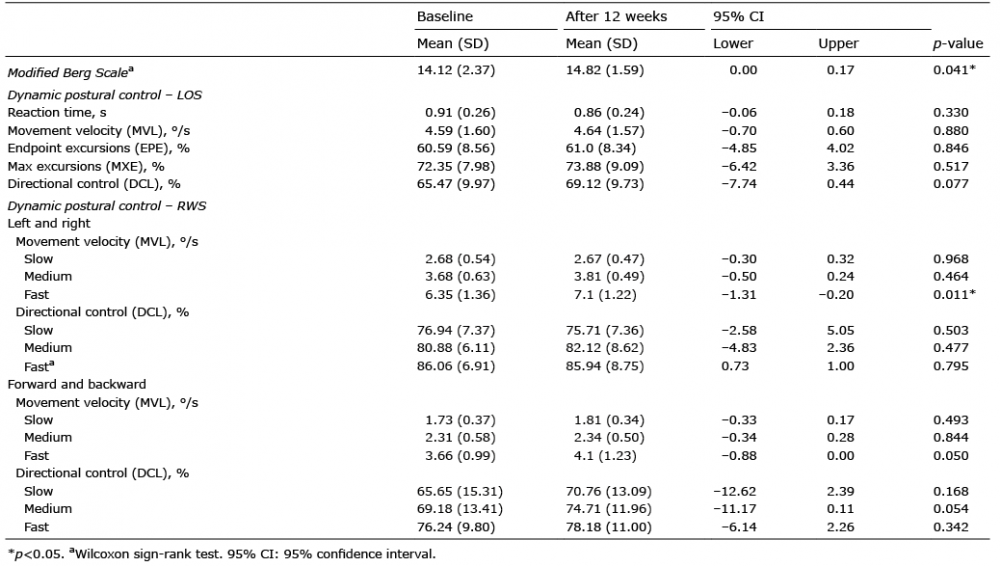 Click to show fullsize
Click to show fullsize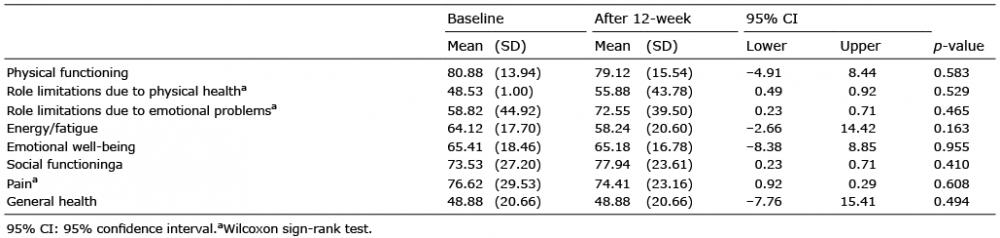 Click to show fullsize
Click to show fullsize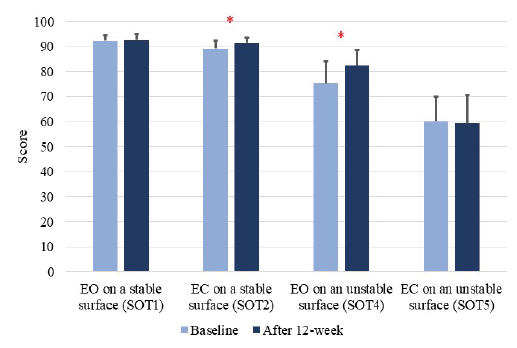 Click to show fullsize
Click to show fullsize