
1Department of Physical Medicine and Rehabilitation, Temple University Hospital, Philadelphia, PA, USA
2MossRehab, Elkins Park, PA, USA
3Department of Rehabilitation Medicine, Sidney Kimmel Medical College, Philadelphia, PA, USA
Background: Intrathecal baclofen is considered an adjuvant therapy for patients with intractable spasms due to stiff-person syndrome. There is increasing evidence to support the use of intrathecal baclofen in the management of symptomatic stiff-person syndrome, with improvement in function.
Case report: A 38-year-old woman with stiff- person syndrome initially presented to inpatient rehabilitation for intractable muscle spasms. The symptoms made her non-ambulatory and limited her tolerance to wheelchair use for mobility. The patient underwent up-titration of oral baclofen and diazepam, with concurrent intravenous immunoglobulin cycles, leading to transient symptom relief. She agreed to explore intrathecal baclofen therapy. An initial trial of a single bolus of 50 μg intrathecal baclofen resulted in a significant decrease in spontaneous spasms, enabling modified independence in transfers and ambulation. The patient was subsequently implanted with a permanent intrathecal delivery system. To date, the intrathecal baclofen had been titrated to 186 μg per day with simple continuous delivery. The patient was weaned off oral baclofen. She attained complete functional independence with ambulation without the need for assistive devices, and has had no lasting post-procedural complications to date.
Conclusion: This case report adds to the increasing evidence of cases of refractory stiff-person syndrome managed successfully using intrathecal baclofen therapy.
Key words: stiff-person syndrome; intrathecal baclofen; intrathecal therapy.
Accepted Feb 4, 2021; Published Mar 3, 2021
JRM-CC 2021; 4: jrmcc00052
Correspondence address: Bruce Zhang, Temple University Hospital, Physical Medicine and Rehabilitation, 3401 N. Broad St, Philadelphia, PA 19140, USA. E-mail: bruce.zhang@tuhs.temple.edu
Doi: 10.2340/20030711-1000052
“Stiff-person-syndrome” is a rare disease that causes debilitating muscle spasms and pain. Patients often cannot walk as a result. The disease is believed to be auto-immune; for unclear reasons the body attacks a part of the central nervous system that normally works to calm the muscles. Sometimes medications that we normally take by mouth can be introduced into the human body directly through the central nervous system. Baclofen is one such medicine that can calm muscle spasms but often has intolerable side effects when taken by mouth. By introducing Baclofen in a controlled fashion directly into the central nervous system through a technique called “intrathecal delivery,” we can offer “stiff-person-syndrome” patients symptom relief without affecting the rest of the body. In this report, we describe a 38 year old woman with “stiff-person-syndrome” that responded very well to intrathecal baclofen. She was able to walk without assistance after treatment.
This case describes a woman with refractory stiff-person syndrome (SPS) who derived marked clinical improvement with intrathecal baclofen (ITB) therapy after failing up-titration of oral diazepam and baclofen with concurrent intravenous immunoglobulin (IVIG) cycles. Oral baclofen and diazepam are considered first-line therapies for symptomatic treatment of SPS, but often require aggressive up-titration, with, at times, intolerable side-effects. IVIG is considered next-line therapy, with the potential for symptom management and alteration of disease progression (1, 2). Case reports and series have demonstrated the viability of ITB therapy as an effective option for patients with intractable spasms due to SPS (3–7). This case report serves to add to the literature suggesting the efficacy of ITB as a successful adjuvant therapy. The notable aspect of this particular case is the significant functional improvement associated with ITB therapy.
A 38-year-old woman with a medical history of type I diabetes mellitus and SPS initially presented to inpatient rehabilitation with intractable and painful muscle spasms due to SPS. The diagnosis of SPS was confirmed by elevated anti-glutamic acid decarboxylase antibody levels (>250 IU/mL). Her symptoms were episodic in nature and triggered by light palpation along the lower limbs. Emotional distress also worsened symptoms. Episodes would last up to 8 h per day. Examination was notable for severe and painful muscle flexor spasms, which were clonic and diffuse. The spasms were particularly notable in her left lower limb with corresponding left ankle inversion, and right upper limb with elbow flexion and forearm supination. The patient underwent serial up-titration of oral baclofen up to 15 mg 3 times a day and diazepam up to 20 mg every 6 h, with concurrent IVIG cycles, with only transient symptom control. Her symptoms made her non-ambulatory and limited her tolerance to using a wheelchair for mobility. She also required moderate-to-maximum assistance for bed mobility, transfers and lower limb dressing. The patient was subsequently referred to the spasticity clinic to be assessed for ITB therapy. She underwent a trial of a single bolus of 50 μg baclofen via a lumbar puncture at the L3–L4 interspace (Fig. 1A and Fig. 1B), resulting in a significant decrease in spontaneous spasms, which lasted for hours. She demonstrated modified independence on transfers and ambulation following the test dose procedure, without requiring an assistive device. The patient was then referred to neurosurgery and ultimately implanted with a SynchroMed II intrathecal delivery system (Medtronic, Inc. Minneapolis, Minnesota, USA), with the catheter tip placed at the T8 spinal level. Her post-procedural course was complicated only by a transient post-dural puncture headache. To date, her ITB has been titrated to 186 μg per day with simple continuous delivery. The patient was weaned off oral baclofen and required only intermittent oral diazepam, with 5 mg once or twice daily. To date, she has mild allodynia in the left lower limb. She attained complete functional independence with ambulation and continues ambulating without needing an assistive device. She remains independent in bed mobility, lower limb dressing, and transfers. She continues ITB therapy with occasional IVIG cycles, directed by neurology. Her baclofen dose has been stable for 36 months following the titration phase of therapy. She has experienced no lasting adverse effects from ITB therapy.
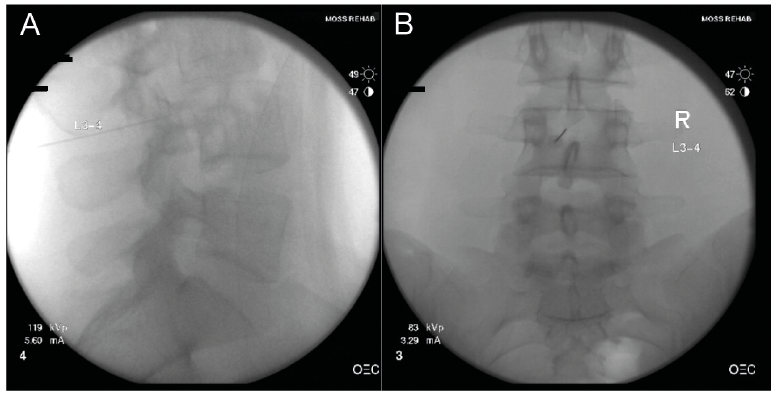
Fig. 1. (A) Sagittal view depicting fluoroscopy-guided intrathecal baclofen trial at the L3–L4 interspace. (B) Anterior-posterior view depicting fluoroscopy-guided intrathecal baclofen trial at the L3–L4 interspace. These are fluoroscopy derived radiographs (X-Rays) of anterior-posterior and lateral views of the patient’s lumbar spine, demonstrating appropriate placement of the spinal needle at the L3-L4 interspace during the patient’s initial intrathecal baclofen trial.
SPS is a rare disorder, consisting of muscle rigidity and rhythmic spasms, which can cause severe disability with impaired ambulation. The symptoms of SPS are thought to be secondary to decreased inhibition within the central nervous system (CNS) due to antibody-derived inhibition of glutamic acid decarboxylase (GAD), a crucial enzyme within the gamma amino butyric acid (GABA) formation pathway (1, 2). Patients have serum anti-GAD antibodies and, subsequently, have decreased GABA within the CNS. It is unclear whether titre levels correspond with clinical severity or presentation (8). The disease process is believed to be auto-immune in nature, and is particularly associated with type 1 diabetes mellitus, although other associations have been recognized, including thyroid disorders, vitiligo, pernicious anaemia, and paraneoplastic syndromes (1, 2).
Initial treatment typically consists of oral benzodiazepines, such as diazepam or oral baclofen, although baclofen effectiveness has not been verified in randomized clinical trials. Immune-modulation with IVIG is the next line of therapy, and rituximab, or beta cell repletion therapy is also an option (1). Case reports and series have previously demonstrated the viability of ITB therapy as an effective adjuvant option for patients with intractable spasms due to SPS (3–7). Stayer et al. described a retrospective series of 8 patients, notably highlighting 5 patients with intractable non-ambulatory SPS who responded to intrathecal therapy and were subsequently able to ambulate limited distances with crutches (6). The largest recent single-institution case series of 9 patients, by Abbetemarco et al., demonstrated more variable results with ambulation. Of the two patients who were non-ambulatory prior to ITB pump placement in the study, one did not attain ambulation with or without assistive device after ITB pump placement and chronic infusion, and the other was not included in the data-set (3).
The primary advantage of ITB delivery is the achievement of therapeutic baclofen levels with smaller drug doses compared with an oral route, maximizing efficacy while minimizing systemic side-effects (9). ITB may then be titrated to achieve a CNS effect beyond that which may have been tolerated from maximal oral therapy. ITB is often limited as a third-line or adjuvant therapy option, as it requires trial administration and subsequent surgical implantation of a pump device, which is invasive. Inherent risks include surgical site infection and hardware malfunction (9). There have been case reports of pump failure with intermittent catheter leakage in patients with SPS after baclofen pump implantation, resulting in acute baclofen withdrawal, which is a potentially life-threating complication (10, 11).
In the current case report, a swift, significant improvement in functional status was observed after ITB trial and subsequent pump implantation. The patient opted to trial ITB as an adjuvant with her intermittent IVIG sessions. Symptoms were exquisitely well controlled, and she was able to ambulate without assistive devices. Without ITB therapy, the patient would not have attained this degree of functional independence, particularly with regard to ambulation. To date, no adverse events have been reported after 36 months.
Although it is considered an adjuvant therapy, case reports and series have demonstrated the viability of ITB therapy as an effective option for patients with intractable spasms due to SPS (3–7). This case report adds to the growing evidence of successfully managed cases via ITB therapy.
This case report was presented as a poster at the 2019 Annual Assembly of the American Academy of Physical Medicine and Rehabilitation.
Dr. Saulino has served on speakers boards and has received funds for research from Medtronic, Inc.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize