
1Department of Rehabilitation Medicine, Sidney Kimmel Medical College, Thomas Jefferson University Hospital, Philadelphia, USA
2Department of Biology, University of Pennsylvania, Philadelphia, PA, USA
Objective: Low back pain caused by osteoporosis-induced thoracolumbar vertebral compression fractures is a common debilitating disorder. The aims of this study were to determine the accuracy and efficacy of spinal dorsal ramus injection and radiofrequency neurolysis for pain reduction in patients with this condition.
Methods: This study was a retrospective chart review of 46 patients with low back pain caused by osteoporosis-induced thoracolumbar vertebral compression fractures. All patients had been treated with spinal dorsal ramus injection with mixed Sensorcaine (Fresenius Kabi, USA) and Depo-Medrol (Pfizer, USA). In some patients further treatment with radiofrequency neurolysis had been required after the initial injection wore off.
Results: Out of a total of 46 patients, 45 (97.7%) had ≥ 50% reduction in low back pain immediately after injection. After the initial injection wore off, 18 patients remained pain free and 27 required radiofrequency neurolysis. The follow-up period ranged from 60 to 1,440 days (mean 335 days). The intensity of low back pain decreased from 7.09 ± 0.84 (numerical pain scale of 0–10) before treatment to 1.39 ± 1.51 immediately after the injection, and to 0.96 ± 1.36 at the last office visit.
Conclusion: Spinal dorsal ramus injection and radiofrequency neurolysis are effective and accurate therapies for low back pain caused by osteoporosis-induced thoracolumbar vertebral compression fractures.
Key words: spinal dorsal rami injection; radiofrequency neurolysis; low back pain; thoracolumbar vertebral compression fractures; osteoporosis.
Accepted Mar 16, 2021; Published Apr 12, 2021
JRM-CC 2021; 4: jrmcc00054
Correspondence address: Linqiu Zhou, Department of Rehabilitation Medicine, Sidney Kimmel Medical College, Thomas Jefferson University Hospital, Philadelphia, PA, USA. Email: linzhoumd@yahoo.com
Doi: 10.2340/20030711-1000056
Low back pain caused by osteoporosis-induced fractures is a common debilitating disorder. The fractured vertebra results in a wedge deformity. A small nerve at the back of this fractured vertebra can become stretched causing back pain. Injecting this small spinal nerve with local anaesthetics provides relief of low back pain. In some cases, if pain recurs after the initial injected medication has worn off, burning this nerve with a special needle can provide long-term pain reduction. Both the injection and the burning of the nerve are minimally invasive, effective and accurate procedures.
Osteoporosis is one of the most common bone diseases worldwide. Patients with osteoporosis are prone to fractures in the spine, proximal hip and distal wrist. Ageing populations have resulted in increased osteoporotic thoracolumbar vertebral compression fractures (TLVCFs). In most patients, the fracture occurs at the thoracic and lumbar spine, especially at the thoracolumbar junction. Low back pain (LBP) caused by TLVCFs can impair patients’ physical functioning and quality of life. The cost and time of caring for these patients place a significant burden on their families and on society (1). LBP caused by TLVCFs is not fully understood, and treatment is challenging (2).
In the last 20 years, vertebroplasty and kyphoplasty have become popular tools to treat LBP caused by osteoporosis-induced TLVCFs (3–6). These procedures consist of injecting medical cement into the fractured vertebral body to enhance stability and reduce pain. However, these procedures are invasive and costly (6–8). Furthermore, vertebroplasty and kyphoplasty may not be safe options for patients with severe deconditioning, cardiac and pulmonary comorbidities, anticoagulation usage, burst fractures, pedicle fractures, or severe compression fractures (9). Furthermore, after vertebroplasty, some patients have continuing LBP.
In a previous study (10), we found that patients with TLVCFs present with LBP at the corresponding spinal dorsal rami (SDR) distributions. It was hypothesized that if these SDR were injected with a low volume of local anaesthetic, the pain would be relieved immediately. In cases with longer than 24 h of pain relief after injection, the injected SDR are the origin of the pain. In some cases, radiofrequency neurolysis (RFN) can provide long-term pain relief if pain recurs after the local anaesthetic has worn off.
The aims of this study were to test the accuracy and efficacy of SDR injection and RFN for LBP caused by TLVCFs.
This was a retrospective chart review. The patients were from the urban and suburban areas. The study was approved by the Thomas Jefferson Institutional Review Board for Studies of Human Subjects (04U463R). The chart review included patients from January 2008 to June 2019.
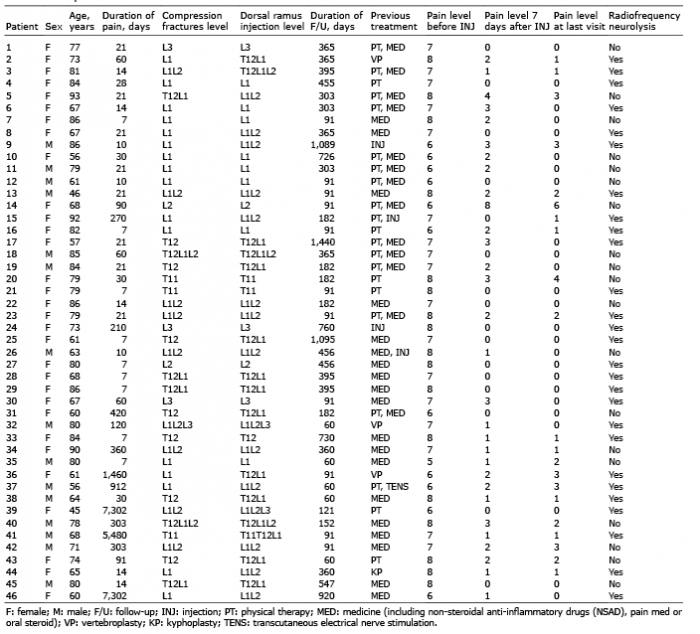
Inclusion criteria were: patients presenting with LBP and osteoporosis-induced TLVCFs at the lower thoracic and upper lumbar spine had undergone lumbar dorsal ramus injection. A total of 46 patients were included in the study. The duration of LBP ranged from 7 days to 20 years, with a mean duration of 1.5 years (Table I). All patients had been diagnosed with osteoporosis-induced TLVCFs by imaging studies (X-ray, computed tomography (CT) scan, or magnetic resonance imaging (MRI)). Out of the total of 46 patients, 31 had a single-level fracture (T11: 3, T12: 7, L1: 16, L2: 2, and L3: 3) and 15 had multi-level fractures (T12/L1: 4, T12/L1/L2: 2, L1/L2: 8, L1/L2/L3: 1). Four patients presented pain in the same area as prior to their lumbar vertebroplasty or kyphoplasty. All patients had previously failed to respond to conservative therapies, including pain medication, physical therapy, braces, trigger point injection, epidural injection, and/or vertebroplasty.
Table I. The patient data
Clinically, the patients reported LBP, especially over a dorsolateral region on the iliac crest, depending on the fractured vertebrae. Physical examination demonstrated protruding spinous processes and widening of the spinous processes space (feeling for a step-off) at the fractured levels (Fig. 1a). There was deep tenderness at the junction of the lateral zygapophysial (facet) joint and proximal transverse process at the step-off level, and the patient reported pain radiating to the dorsolateral region on the iliac crest (Fig. 1b). A total of 38 patients had a single level of tenderness at the fracture level; and 18 patients had additional tenderness at the level above or below the fracture. A total of 32 patients had pain on both sides, and 14 patients had pain on one side. Levels of tenderness were documented for the dorsal ramus injections.
Fig. 1. (a) Physical examination: palpation of the spinal processes (feeling for a step-off) revealed protruding spinous process and widening spinous process space at the fracture level. (b) There was deep tenderness at the junction of the lateral zygapophysial (facet) joint and proximal transverse process at the step-off level. The patient reported pain radiating to the dorsolateral region on the iliac crest.
Dorsal ramus injections had been performed under fluoroscopic guidance, with the patient in a prone position, with a mild intravenous sedation or local anaesthetics only. The injection target was the dorsal ramus at the tenderness level. The injections had diagnostic, as well as therapeutic, purposes. Immediate pain reduction after injection indicated that the pain originated from the dorsal ramus (rami) of TLVCFs. Some patients received long-term pain relief after the initial injection. Patients whose pain reoccurred after 24 h following the initial injection underwent RFN at the same blocked nerves. During the injection or RFN procedure, patients cooperated fully with the physician to confirm the positioning of the nerve injection. When the needle or RFN probe was approaching the involved dorsal ramus, the patients experienced similar to the sharp pain that radiated to the primary painful area.
The primary dorsal ramus is located at the superior junction of the lateral facet joint and proximal superior transverse process, where is the needle entry target (Fig 2. a). When the bony contact was made with the needle and with negative aspiration of blood and spinal fluid, 0.3ml of Omnipaque 240 (GE Healthcare Ireland, Cork, Ireland) was injected to confirm that no intravenous or intrathecal spreading occurred (Fig. 2). Then, 1 ml mixture of 0.5 ml 0.25% Sensorcaine (Fresenius Kabi, USA)) and 0.5 ml/20 mg Depo-Medrol (Pfizer, USA)) was injected.
The RFN procedure was performed in a similar fashion. A 20-gauge curved tip RFN needle was used for the neuroablation. The appropriate placement of the RFN needle was confirmed by the patient’s experience of pain, which radiated to the area reported as painful when the probe approached the nerve. The parameters of neuroablation were set at the sensory level of 50 Hz, with a stimulating intensity less than 0.7 V; 20 Hz motor, with a stimulating intensity less than 1 V; and 90°C ablation, set at 2 min. After the ablation, 1 ml (of a mixture of 0.5 ml 0.25% Sensorcaine and 0.5 ml 20 mg DepoMedrol) was injected to prevent RFN-induced neuritis. During the treatment course, all patients were instructed regarding routine osteoporosis treatment and exercises (11).
Fig. 2. The fluoroscopy of the thoracolumbar spine anteroposterior (AP) view (a) and lateral view (b). The needle entry targeted at the superior junction of the lateral facet joint and the proximal superior transverse processes of T12 and L1(a), where the dorsal ramus passes. After the bony contact was made with the needle and with negative aspiration of blood and spinal fluid, 0.3 ml of Omnipaque 240 (GE Healthcare Ireland, Cork, Ireland) was injected to confirm no intravenous and intrathecal injection (a, b). The lateral view shown the needles at posterior of spinal canal (b).
Outcome assessment
All patients were asked to complete a pain diary prior to the injection, immediately after the injection, 7 days after the injection, and at each follow-up appointment. The pain diary consisted of a numerical pain scale (NPS) of 0–10 (with 0 being no pain and 10 being the most severe pain that the patient has ever experienced). Data about patient self-reporting functional levels (including self-care, daily activities, and walking), pain medication use, and complications from the procedure were also collected.
Data analyses were performed using Stata v14 (StataCorp. LLP, College Station, TX, USA). The NPS before injection, immediately after injection, 7 days after injection, and at the last office visit (60-1440 days) were compared using paired t-tests. The NPS was presented as the mean (standard deviation (SD)). Differences were considered statistically significant at p < 0.05.
A total of 46 patients were included in the study (14 males, 32 females; age range 45–93 years, mean age 73 years). Of these, 45 (97.8%) patients had ≥ 50% LBP relief immediately after the injection (Table I). Twenty-one of the 45 patients underwent dorsal rami RFN at the same injected levels when their pain recurred. The other 16 patients remained pain-free throughout the entire study after their initial injection. During the follow-up period (from 60 to 1,440 days, mean 335), all of these 45 patients continued with ≥ 50% reduction in pain. The LBP intensity decreased from 7.09 of NPS (SD 0.84) before the injections to 1.39 (SD 1.5) 7 days after treatment (p < 0.00005), and to 0.96 (SD 1.36) at the last appointment (p < 0.00005) (Table II). There was no significant difference in pain reduction immediately after the injection compared with the last office visit (80% (SD 23%) vs 86% (SD 21%), p = 0.011). No patient required vertebroplasty/kyphoplasty or surgical intervention after the SDR injection or RFN. All of the 45 patients had increased levels of functioning, including self-care, daily activities and walking. Forty-one of these patients stopped taking pain medication, and 4 decreased their usage of pain medication. One patient (2.2%) did not respond to the injection. There were no complications associated with the injections or RFN.
Table II. Comparison of pain level (numerical pain scale of 0–10)
LBP caused by osteoporosis-induced TLVCFs is a debilitating medical condition that remains a therapeutic challenge. The goals of intervention are to alleviate pain, help patients return to their normal activity, stabilize the fracture, and prevent complications. Current treatments include pain medication, activity modification, physical therapy, thoracolumbar orthosis, spinal injection, spinal fusion, and treatment for primary osteoporosis (1, 2). However, for many of these patients, these modalities do not provide effective pain relief. In recent decades, vertebroplasty and kyphoplasty have become popular therapies to alleviate TLVCF-induced LBP (3, 4). However, there is a lack of evidence to prove that vertebral augmentation can provide effective relief of back pain (2). There are reports of serious adverse effects with this treatment, such as pulmonary embolism, neurological deficits, infection, rib fractures, and adjacent-level TLVCFs (2). Part of the challenge is that we do not fully understand the mechanism of LBP after TLVCFs. Van Dieën hypothesized that the endplate fracture in TLVCFs is the cause of LBP (12). Conversely, Kherad et al. found that only 50% of patients with TLVCFs presented with back pain, while the other 50% never had back pain. (13).
One of this article authors (L.Zhou) participated in 9 thoracolumbar dorsal rami cadaver studies in China (10, 14). The anatomy of the thoracolumbar SDR is described in this paper in order to help understand the causes of LBP (10, 14–16). The dorsal root ganglion divides into 2 branches at the lower thoracic and upper lumbar spine. The ventral branch travels anteriorly and laterally; forming the nerve or lumbar plexus, which innervates the lower ventral trunk and anterior thigh (Fig. 3d). The dorsal branch, also called the primary dorsal ramus, travels posteriorly, laterally, and caudally, surrounding the anterior lateral facet joint. It then enters the superior border of the transverse process through an anatomical foramen bounded by the anterior aspect of the superior articular facet joint and the intertransverse ligament. This anatomical location is the target of the primary SDR injection or radiofrequency neurolysis. The primary dorsal ramus then divides into the medial, lateral branches and, in some cases, intermediate branches (15). Both medial and lateral branches are a mixture of sensory and motor fibres (Fig. 3a–d). In some cases, either the primary dorsal rami, or medial, or lateral rami give out an intermediate branch. The intermedial branches form intersegmental communicating loops and innervate muscles (15), which is less clinically relevance. The detail of the intermediate branch anatomy is therefore not described in the paper.
The medial branch travels from the superior border of the transverse process posteriorly, caudally, and medially, and enters the groove formed by the transverse process and the lateral aspect of the superior articular process (Fig. 3c and d). This is the location of the medial branch block. After giving out a small branch to innervate the inferior aspect of the facet joint, the medial branch extends caudally to innervate 1–2 lower levels of the facet joints (Fig. 3a–d). The medial branches also supply the multifidus muscles, interspinous ligament, and interspinal muscles (10, 14, 15).
The lateral branch, a large branch of the dorsal ramus, exits from the osseous groove of the superior transverse process and travels caudally, laterally, and dorsally. It gives off branches, which supply the iliocostal and longissimus muscles. The main lateral branch then pierces the thoracolumbar fascia to innervate the subcutaneous tissues and skin. The T12 and L1 lateral dorsal rami innervate the dermatome of the dorsolateral region on the iliac crest and the anterior superior iliac spine. The L2 and L3 lateral dorsal rami innervate the middle iliac crest and the buttocks (Fig. 3a and b) (10, 14–16).
Fig. 3. Dorsal rami dissections. (a) and (b) Posterior view of the right T12, L1, L2, L3, L4 spinal dorsal rami nerves. The medial branches (M) innervate the zygapophysial (facet) joints (Z) and the tissue medial to the facet joint line. The lateral branches (L) innervated the tissue lateral to the facet joint line. The T12 and L1 lateral branches terminate in the lateral gluteal region, and L2, L3 and L4 lateral branches terminate in the medial gluteal area. (c) The primary dorsal ramus (D) emerges from the neural foramen, dividing into the medial (M) and the lateral (L) branches at the upper margin of the transverse process (T) is seen in a close-up view. The medial branch then descends in the groove between the superior articular processes of the facet joint (Z) and the root of the transverse process. (d) Drawing of close-up view of the primary dorsal ramus. Ventral branch (V). In some cases, either the primary dorsal rami, or medial, or lateral rami give out an intermediate branch. The intermedial branches form intersegmental communicating loops and innervate muscles, which is less clinically relevant. Therefore, the detail of the intermediate branch anatomy is not described in this fig.
The medial branches of the dorsal ramus supply the tissues from the midline to the facet joint line. The lateral branches innervate the tissues lateral to the facet joint line (10, 14, 16).
Since the SDR crosses the facet joints and transverse processes, any biomechanical stress to the facet joint and transverse process will irritate the dorsal rami, resulting in LBP in the distribution of the dorsal rami. Vertebral body wedge deformity and instability secondary to osteoporotic TLVCFs can cause stretching tension of the SDR, which induces LBP. Hoshino et al. found that the severity of back pain is directly associated with the angular deformity and instability within the affected vertebral body (17). The painful area of TLVCFs may not occur at the fractured level, but at the areas innervated by the involved SDR. This phenomenon is similar to sciatic pain caused by lumbar herniated disc. The patient has LBP with radiation to the leg. Friedrich et al. found that 80% of patients with osteoporotic TLVCFs reported that their pain referred mainly to the lumbosacral and gluteal areas (18). Kim et al. reported that patients with TLVCFs experienced pain at the iliac crest and buttocks (19), which are innervated by the T12 and L1 lateral branches.
If the patient presents paraspinal muscle spasm, the medial branch of the dorsal ramus is involved. If the pain is at the lateral low back, dorsolateral region on the iliac crest or buttock, the lateral branch is affected. When the patient presents with paraspinal muscle spasm and pain at the dorsolateral region on the iliac crest, the primary dorsal ramus is involved. In the current study, pain caused by osteoporotic TLVCFs was seen at the medial branch/ lateral branch or both medial and lateral branches. The pain can be on one or both sides.
During physical examination, the physician can normally feel a protruding spinous process or a widening spinous process space at the fracture level by palpation (10). There is a site of deep tenderness at the junction of the lateral facet joint and proximal transverse process at the same level as the fracture. This deep tenderness can radiate to the area of the patient’s primary complaint. In some cases, patients experience the deep tenderness at the adjacent upper and/or lower vertebra to the fracture, because the compression deformity can irritate the dorsal rami of the adjacent vertebra. The deep tenderness levels are the targets for SDR injection.
Based on our hypothesis of back pain caused by dorsal rami involvement secondary to the compression fracture, injecting these nerves should provide both diagnostic information and therapeutic pain reduction. Injection with a combination of local anaesthetic and a low dosage of steroid is used to inhibit C-fibre transmission and provide prolonged peripheral nerve block (20). In the current study, 45 of 46 patients (97.8%) experienced more than 50% pain reduction, which lasted more than 6 h after injection. Sixteen of these 45 patients received permanent pain relief after the initial injection. In order to achieve long-term pain relief, 29 patients required RFN after their initial pain reduction had worn off. Of the 45 patients who experienced more than 50% pain reduction, all improved their self-care, daily activities, and walking. Of these patients, 41 stopped taking pain medication and 4 decreased their usage of pain medication after the injections or RFN.
Dorsal ramus injection is an effective alternative to vertebroplasty or kyphoplasty, because it has a high success rate, low risk of complications, and lower medical cost. Saracen (21) reported that, in 616 patients treated with vertebroplasty, 41.7% experienced complications, such as local cement leakage, paravertebral vein embolism, intradiscal or spinal canal leakage, and pulmonary embolism. Robinson (22) found that 20 of 102 patients with kyphoplasty developed complications of new fractures in adjacent levels, cement extravasation, infection, spinal stenosis, and bleeding. Injection of the primary dorsal ramus targets the lateral facet joint and proximal transverse process, but not the neuroforamen. Therefore, complications, such as epidural bleeding, nerve injury, epidural punch, and epidural leakage, which occasionally occur during interlaminar or transforaminal epidural injection, are unlikely to occur during SDR injection. SDR injection is minimally invasive and a tolerable procedure. The procedure can be performed under local anaesthesia by a physician without special training (10). However, the physicians performing vertebroplasty or kyphoplasty require special training. The medical costs of vertebroplasty or kyphoplasty are high (23). The costs in the USA of SDR injection are approximately $500–550 (US dollars), and neuroablation is approximately $800–850 per level (24). However, the costs of vertebroplasty are $3,000 to $6,000 per level (25).
Prior to the current study, there are no publications reporting SDR injection that relieves LBP caused by osteoporosis-induced TLVCFs. Ergin performed a transformational epidural injection to relieve severe back pain caused by cement leakage during a kyphoplasty procedure (26). The injection target was the ventral rami. We consider SDR injection to be a superior approach compared with transforaminal epidural injection, as discussed above.
Spinal dorsal ramus injection and radiofrequency neurolysis are effective and accurate therapies for low back pain caused by osteoporosis-induced thoracolumbar vertebral compression fractures.
A limitation of this study is its small size and retrospective nature. Randomized control studies with larger groups are needed to further confirm the accuracy and efficacy of this treatment.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize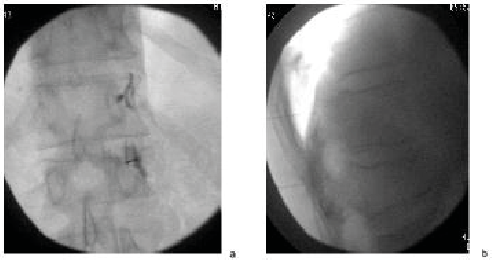 Click to show fullsize
Click to show fullsize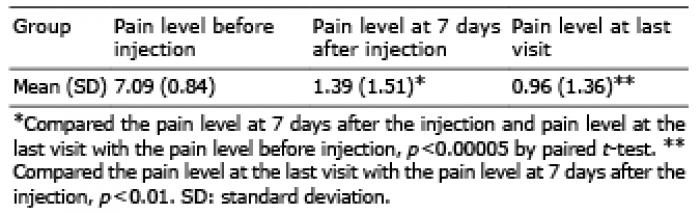 Click to show fullsize
Click to show fullsize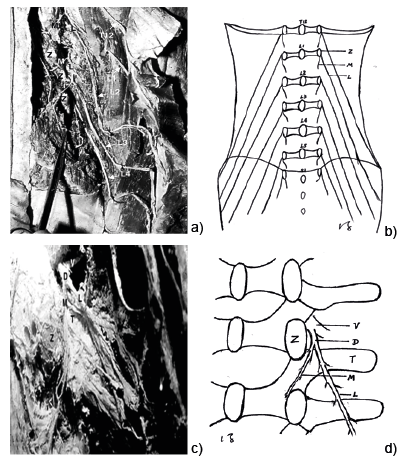 Click to show fullsize
Click to show fullsize