
1Basalt, Vrederustlaan 180, 2543 SW, Den Haag, Amsterdam, The Netherlands
2Livit Orthopedie, Kabelweg 40, 1014 BB, Amsterdam, The Netherlands
Pain, stiffness and joint deformity can result in significantly reduced hand function in people with osteoarthritis. Characteristic finger deformities in osteoarthritis are swan neck deformity and boutonnière deformity. Several studies have reported that an orthosis decreases pain and increases function during daily activities for patients with arthritis. The aim of this study was to review patient-reported outcomes of current conservative therapeutic management with silver ring splints (silversplints) for patients with osteoarthritis of the hand. There was a 76% improvement in overall daily functioning and a 74% reduction in pain. Several questions concerned daily activities with different types of hand function and with different types of grip and use of fingers. The results show a major improvement in both the more open grip of the hand and activities requiring fine motor skills. The ability to use force with the hand, even when wearing an orthosis, is an important result. Patients who experienced “no problems or minor problems” had significantly increased functioning in several activities of daily living, but the largest improvement in functioning was seen in “household chores” (243%), “opening jars” (150%) and “lifting groceries” (143%). Overall, silversplints appear to serve as a suitable support for the joints in osteoarthritis of the hand, providing pain relief by preventing the joint from moving through its full range of motion. Use of silversplints to treat patients with osteoarthritis of the hand should be considered as a useful, non-surgical method.
Key words: osteoarthritis; hand deformities; arthritis; splint; orthotic devices.
Accepted Apr 20, 2021; Published May 21, 2021
JRM-CC 2021; 4; jrmcc00060
Correspondence address: Jan Willem van der Windt, HQ, Livit Orthopedie, 1014 BB Amsterdam, The Netherlands. E-mail: jwindt@livit.nl
Doi: 10.2340/20030711-1000060
This study of patient-reported outcome measures regarding the use of silversplints for osteoarthritis of the hand provides insight into the additional care and quality of life provided by the use of an orthopaedic medical aid. The aims of this study are to measure the effectiveness of silversplints in daily life and to validate the efficacy of using orthopaedic medical aids. Between October 2018 and June 2020, a total of 2,231 patients with osteoarthritis were provided with silversplints and were asked about the effectiveness of the splints 3 weeks after they first started wearing them. This large-scale study found that the use of silversplints contributed to overall daily functioning, reduced pain, and increased the possibility of performing daily activities. Silversplints appear to serve as a suitable support for joints, providing pain relief and freedom of movement, but preventing the joint from moving through its full range of motion.
Osteoarthritis (OA) is a clinical syndrome characterized by joint pain, stiffness and functional impairment. OA of the hand usually occurs in the carpometacarpal joint of the thumb (CMC-I, 21%), the proximal interphalangeal joints (PIP) and the distal interphalangeal joints (DIP, 35%) (1, 2). In addition, 50% of patients with DIP involvement also have proximal interphalangeal (PIP) joint involvement (3).
The prevalence and incidence of OA are significantly higher for women than for men, and increase with age. The majority of people older than 55 years have radiological features of OA of the hand and/or wrist, with 20% experiencing clinical symptoms (4, 5). Most patients report an increase in pain symptoms over a period of 2 years, but OA of the hand does not always develop progressively. As the disease progresses, the grip strength begins to deteriorate. Mechanical factors, such as abnormal loading of the joint (trauma), heavy labour, joint instability and obesity can increase the risk of OA.
Symptoms of OA can be controlled by interventions aiming at self-management, avoiding excessive joint loading and by giving pain medication, corticosteroid injections in the joint and hand therapy (1, 2).
Several studies have reported that an orthosis decreases pain and increases function during daily activities for patients with arthritis. (6, 7, 8, 9) Orthosis for OA are frequently used to decrease pain, minimize deformities, decrease inflammation, decrease stress to the joints, provide support for increased function and assist with joint stability (10, 11). A silver ring splint (silversplints) can serve as a suitable support for the joint, providing pain relief. Wearing silversplints restricts movement, preventing the joint from moving through its full range of motion (7, 12, 13).
The aims of this study of patient-reported outcome measures (PROM) for use of silversplints for OA of the hand were to measure the effectiveness of silversplints in daily life and to validate the efficacy of using orthopaedic medical aids.
PROM research is a method for measuring health in terms of physical and/or mental well-being and functioning in daily life for patients. PROM studies of orthopaedic medical aids still play a minor role in improving patient care and only a limited number of studies have been published. The Dutch National Healthcare Institute made an online toolbox available (14), which served as a guideline for the design of this study (15). In this study the following patient-reported outcomes (PRO) were defined:
Statistical analysis
To improve quality, information is needed about health prior to and after an intervention. This study compared feedback from customers about function gained with and without silversplints. There are no standard or target values that could be used in the study, as there are no comparable studies regarding to the effectiveness of these orthopaedic aids.
Between October 2018 and June 2020, a total of 2,231 patients with OA were provided with silversplints. They were asked about the effectiveness of the splints 3 weeks after they first started wearing them. The questionnaires were sent by email. Only one email was sent to the patients and participation was voluntary. The questionnaire contains 10 questions, each using a qualitative ordinal 5-point scale in terms of limitations in performing a certain task or activity. Patients had to report limitations with and without using silversplints. Age and sex were also surveyed.
Descriptive statistics are the basic measures used to describe this survey data. They consist of summary descriptions of frequency and percentage response distributions, and for measure of central tendency the mode is used (17).
With a population size of 6,500 patients who started using silversplints in the Netherlands in the study period and a confidence level of 95%, a margin of error of 3% was calculated. This expresses the amount of random sampling error in the results of a survey.
All silversplints were provided by Livit Orthopedie, a Dutch provider of orthotic and prosthetic services and products. The silversplints are made by highly qualified silversmiths, partnered with hand specialists to produce custom-made medical aids. The diagnosis of OA was confirmed by a medical doctor (MD) for all patients. Diagnosis was mostly made on the basis of X-rays and/or magnetic resonance imaging (MRIs), in some cases it was based on the experience of the MD. Patients throughout the Netherlands in various institutions, ranging from university hospitals and rehabilitation centres to nursing homes, were included in this study. As such, the population of this study can be considered representative of users of silversplints in the Netherlands.
Technical information
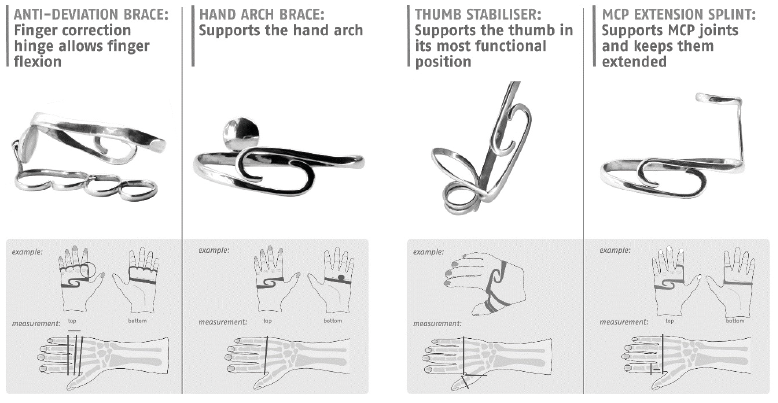
Silversplints are a combination of oval rings made of high-quality sterling silver, which combines adequate strength and rigidity with an attractive appearance. Silversplints are custom made from 925 silver, a hypoallergenic material with antibacterial properties. The material is durable and well protected from wear and tear. Silver does not block skin pores or prevent perspiration, which could result in odour and skin rashes. The devices have no rough edges, allowing the patient to move their hand/fingers as freely as possible, without causing skin irritation or pressure points. The thumb section of silversplints for the wrist/hand is optimally adjusted to the needs of the patient, allowing for pen grip, tweezer grip or key grip. Silversplints are easy to clean, can be used in warm water and rarely cause any skin allergy. (10) (Fig. 1 and Fig. 2)
Fig. 1. Example of silversplints for the hand. (Source: Livit Silversplint catalogue).
Fig. 2. Example of silversplints for the finger. (Source: Livit Silversplint catalogue).
The response rate of this patient-reported outcome study was 38%; 850 of the 2,331 patients completed the questionnaire. All responses could be used. For this study, the 95% confidence interval for the outcome results was –3 to +3%.
Online survey response rates vary greatly depending on the target audience and the nature of the research. The mean response rate for e-mail surveys fluctuates between 25% and 33% (QuestionPro, Dallas, USA). No reminder e-mails were sent to the patients in this study.
Of the respondents 45% were 65 years or over, and 85% were 50 years or over. These patients are in the age range of active people. This age range also matches the greatest prevalence and incidence rates of OA; the majority of people older than 55 years have radiological features of OA of the hand. The majority of respondents in this study (94%) were women.
The results are presented separately for each question asked.
Overall daily functioning
Fig. 3 shows the results change in overall daily functioning. Seventy-six percent of respondents reported that their overall daily functioning improved (some, significantly and very significantly improvement) after they started wearing silversplints. Forty-seven percent of respondents reported that their functional status improved significantly to very significantly, in contrast to 24% who experienced no change or deterioration. No difference was reported between the use of silversplints for the finger or hand or wrist. Seventy-seven percent of respondents with a silversplint for the finger experienced improved daily functioning, for the respondents with a hand/wrist silversplint the experienced improved daily functioning was 75%.
Fig. 3. Results of question: How has your overall daily functioning changed since you started wearing your silver splint?
Pain reduction
Pain reduction is the main reason for wearing or prescribing a wrist orthosis. A wrist orthosis immobilizes, supports and stabilizes the wrist. Theoretically, this should help to reduce the inflammatory process and relieve capsules and ligaments. This should lead to a reduction in pain symptoms.
This study found that the pain and the stress on the wrist are reduced. Fig. 4 shows the results change in pain symptoms. The group using silversplints showed an improvement in pain symptoms of 74%. Forty-three percent reported that their pain symptoms had changed significantly to very significantly, in contrast to 26% who experienced no change or an increase in pain. Again, no difference was reported between the use of silversplints for the finger or hand/wrist.
Fig. 4. Results of question: How have your pain symptoms changed since you started wearing your silversplint?
Daily activities
Several questions were asked concerned daily activities with different types of hand function and different types of grip and use of fingers.
The results show a major improvement (Fig. 5), especially in activities requiring fine motor skills or the more open grip of the hand, for instance when opening a jar or lifting groceries. For opening a jar, the proportion of patients experiencing major problems decreased from 44% without a silversplint to 26% when using a silversplint. In addition, the proportion of patients who were unable to open a jar decreased from 23% to 13%. This question was asked to gain insight into a cylindrical grip with and without an aid. For lifting groceries the proportion of patients experiencing no problems or minor problems increased from 21% without the aid to 51% when wearing a silversplint. This question was asked in order to gain insight into the hook grip and generation of strength with and without the aid. The ability to use force with a hand, even when wearing an orthosis, is an important result. The results for these activities when wearing the silversplint are therefore encouraging.
Fig. 5. Results of questions related to daily activities.
Activities requiring fine motor skills, such as writing, buttoning clothes and using a phone, showed major improvements. The proportion of patients experiencing no problems or minor problems with writing increased from 34% to 60% when using silversplints. Holding a pen means a patient can hold a small, thin object and use it with fine motor skills. This question was asked to gain insight into the pen grip with and without an aid. Silversplints seem to contribute positively to these skills. For buttoning clothes, the results are similar; as the proportion of patients experiencing no problems or minor problems increased from 34% to 63% when using silversplints; an increase of 85%. This question was asked in order to gain insight into the tweezer grip with and without an aid. With a silversplint, more than half of patients had no problems with operating or using a mobile phone, a very important activity in modern life. Combining it with the group of patients with minor problems this proportion increases to 80%.
With silversplints the open hand grip (e.g. as used when holding a book) improved; the proportion of patients who did not experience any problems increased from 17% to 42%, an increase of 147%.
Table I shows the results when the patients with “no problems and minor problems” are combined in a single group for each activity with and without the use of silversplints.
Table I. Improvement in functional status according to activity type
Table II shows the results when the patients with “major problems or unable” are combined in a single group for each activity with and without using silversplints.
Table II. Improvement in functional status according to activity type
Wearing an orthosis for OA of the hand during periods of acute inflammation is designed to reduce joint friction and prevent excessive joint loading by reducing joint motion. Although critics of immobilization report that maintenance of normal tissues require movement, excessive mobilization of unstable arthritic joints can promote further instability. Several studies have reported that an orthosis decreases pain and increases function during daily activities in patients with arthritis (6, 7, 9, 18).
In this PROM study 76% of the patients reported that the overall daily functioning improved when wearing a silversplint. This was just 3 weeks after the patients started to wear the silversplints, which suggests that other beneficiary factors, such as hand therapy or medication did not contribute to this result. The study did not include registration of the use of pain medication, which might have influenced the results. It would be interesting to determine why 24% of the patients did not experience improvement or even deterioration.
Over the past decades, many surgical and non-surgical interventions have been developed to treat CPC-I OA and OA of the hand, with non-surgical interventions, such as splints and hand therapy, being particularly common. The effectiveness of these interventions, however, was quite unknown due to sparse research and studies with varying outcomes.
Tsehaie, affiliated with the Xpert Clinic and Rotterdam’s Erasmus MC, was the first to research the effect of these non-surgical interventions on a large scale, studying 809 patients with CPC-I OA. Patients in this study reported feeling a mean of 39% less pain than before treatment (the pain score decreased from 90 to 55) (19, 20). In this study 74% of the patients reported a significant or very significant decrease in pain, when wearing silversplints for at least 3 weeks. However, 20% experienced no change. The follow-up was short and, since this is a PRO study, no data were available concerning rejection of the silversplints in the group of patients who experienced deterioration of pain after wearing the silversplint.
The results of this study show a major improvement in both the more open grip of the hand and activities requiring fine motor skills. To be able to use force with a hand, even when wearing an orthosis, is an important result. The results for these activities when wearing the silversplint are therefore encouraging. However, no data were recorded regarding how many silversplints a patient was wearing, on which hand (dominant or not dominant) or which kind of silversplint was used (for the fingers or wrist). These aspects could have an influence on functioning with the splints.
The effect of the silversplints was measured after wearing the orthosis for 3 weeks; hence the effects start quite quickly. This may provide support for use of an orthosis in cartilage protection, especially when an orthosis repositions and aligns the joint appropriately. It would be interesting to determine whether the improvement lasts over time.
In a comparative study, silversplints led to equal functional results compared with thermoplastic orthoses, but they were valued more highly on aspects of comfort and cosmetics (21–25). However, in the current study patients were not asked to value these aspects. It would be of interest to study these aspects, since the silversplints were custom made and small details could change the outcome of functioning with this orthosis.
This large-scale PROM study into the effectiveness of silversplints for patients with OA of the hand shows that the use of silversplints contributed to overall daily functioning, reduced pain and increased the possibility of performing activities. Deformities as a result of OA include a mallet finger deformity at the DIP joint and lateral deviation or boutonnière deformities at the PIP joint. Osteoarthritis of the CMC-I joint is usually associated with more functional impairments than PIP or DIP OA. In all cases silversplints appear to give suitable support to the joints, providing pain relief and freedom of movement, but preventing the joints from moving through their full range of motion. The follow-up time in this study was short; it would be of interest to determine whether the improvement in daily activities with use of silversplints lasts over time.
This study was supported by Livit Orthopedie, the Dutch premier provider of orthotic and prosthetic services and products. Providing customer care across The Netherlands with a network of 500 customer locations, 450 staff and 1 production location.
The authos have no conflicts of interest to declare


 Click to show fullsize
Click to show fullsize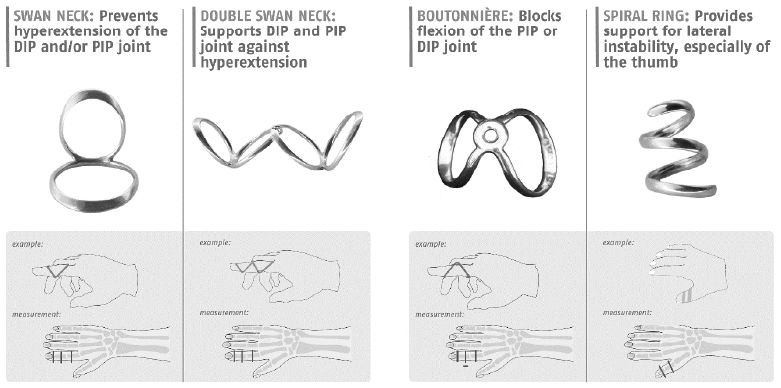 Click to show fullsize
Click to show fullsize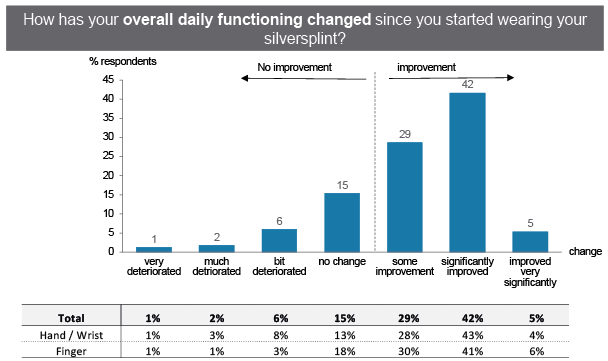 Click to show fullsize
Click to show fullsize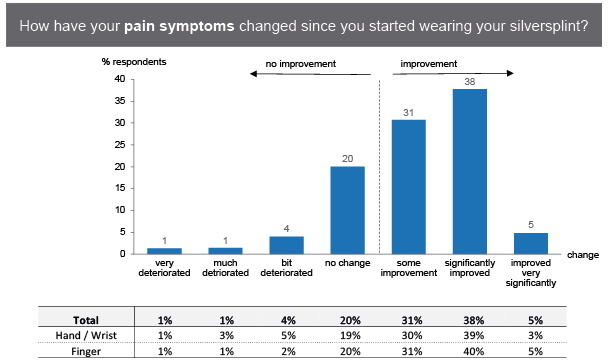 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize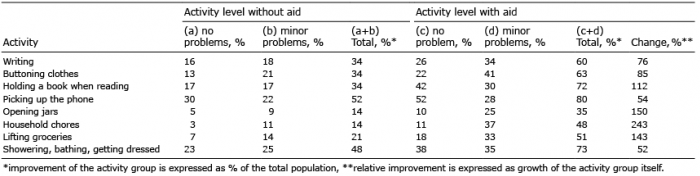 Click to show fullsize
Click to show fullsize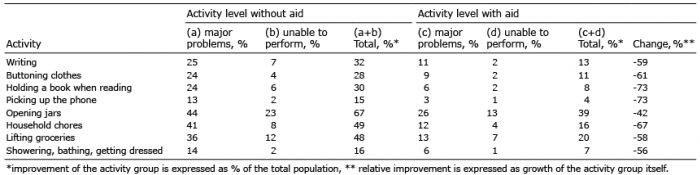 Click to show fullsize
Click to show fullsize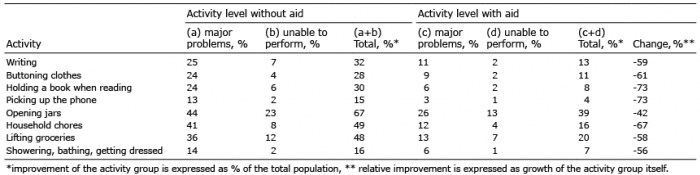 Click to show fullsize
Click to show fullsize