
From the 1Department of Rehabilitation Medicine, Danderyd University Hospital, 2Karolinska Institutet, Department of Clinical Sciences, Division of Rehabilitation Medicine, Danderyd Hospital, Stockholm, 3Department of Community Medicine and Rehabilitation, Rehabilitation Medicine and 4Department of Community Medicine and Rehabilitation, Physiotherapy, Umeå University, Umeå, Sweden
Objective: To investigate the feasibility of a virtual reality exercise intervention within an interdisciplinary rehabilitation programme for persons with chronic neck pain. The effects of the intervention on symptom severity, variables related to chronic neck pain, and patients’ experience of exercises were assessed.
Methods: Nine women and 3 men participated in a 6-week virtual reality exercise intervention during an interdisciplinary rehabilitation programme. Symptom severity was rated before and after each session of virtual reality exercise, using questionnaires before and after the interdisciplinary rehabilitation programme, and questions about participants’ experiences.
Results: Neck pain symptoms increased temporarily during the exercises, but no lasting deterioration was found after the interdisciplinary rehabilitation programme. Depression, pain interference, pain control, sleep and kinesiophobia improved significantly after the programme. Participants experienced that the virtual reality exercises increased motivation to exercise and provided a focus other than pain. However, the equipment was heavy; and exercising was tiring and reminded them of their challenges.
Conclusion: This study indicates that virtual reality exercises as part of an interdisciplinary rehabilitation programme are feasible and safe for patients with chronic neck pain. Pain symptoms may increase temporarily during the exercises. Virtual reality exercises may support participants by increasing motivation to exercise and providing helpful feedback. Further research into the added value of virtual reality exercises in an interdisciplinary rehabilitation programme for patients with chronic neck pain is warranted.
Key words: neck pain; whiplash-associated disorders; virtual reality; interdisciplinary rehabilitation; exercise; feasibility.
Accepted Jun 23, 2021; Published Aug 27, 2021
JRM-CC 2021: 4; jrmcc00067
Correspondence address: Monika Löfgren, Karolinska Institutet,
Department of Clinical Sciences, Danderyd Hospital, Section of
Rehabilitation Medicine, Fotledsvägen 1, 182 88 S-Stockholm,
Sweden. E-mail: monika.lofgren@ki.se
Doi: 10.2340/20030711-1000067
Approximately 20% of the general population have such severe pain that it has a major impact on their daily life. Chronic neck pain is a common diagnosis. For treatment of chronic neck pain, current knowledge supports the use of interdisciplinary rehabilitation programmes; health professionals working in a team together with the patient. Such programmes include education, exercise and psychological intervention. It is possible that exercising with the use of virtual reality might stimulate physical activity and facilitate exercise performance through instant feedback. This study investigated the feasibility of using virtual reality exercises within an interdisciplinary rehabilitation programme for patients with chronic neck pain. The results show that it is possible and safe for patients with chronic neck pain to incorporate virtual reality exercises as part of an interdisciplinary rehabilitation programme. Neck pain symptoms may increase temporarily during the exercises, but no long-lasting deterioration in symptoms was found. No adverse effects occurred due to the interdisciplinary rehabilitation programme. Virtual reality exercises may support participants in increasing motivation and by providing helpful, direct, feedback of their performance during the exercise session.
Chronic pain is one of the most common complaints among individuals seeking contact with healthcare (1). Approximately 20% of the general population in Europe have such severe pain that it has a major impact on daily life (2), and patients with chronic neck pain are a large group (3). In a European survey, chronic neck pain was present in 8% of the population (2) and long-lasting symptoms after a whiplash injury, whiplash-associated disorders (WAD), were commonly associated with chronic neck pain (2). People with neck pain, often have symptoms such as reduced active range of motion, headache and dizziness (4).
When treating patients with neck pain there is a need to consider and target impairments of sensimotor control; disturbed proprioception (4, 5) and impaired cervical movement kinematics (5, 6). For assessment of sensorimotor control, investigation of dizziness or unsteadiness, measurement of cervical position error, postural stability and oculomotor control (7) are important. Cervical movement kinematics may be assessed by asking the patient to follow a trace with their eyes and head, e.g. a visual trace produced using a laser (8) or a computer cursor (9). Evidence for the effect of proprioceptive exercises is, however, unclear and there is a need for further studies (10, 11).
For treatment of chronic neck pain, the evidence supports the use of interdisciplinary rehabilitation programmes (IRPs), with a bio-psychosocial framework, including exercise and psychological intervention (12, 13). IRPs are developed for patients with complex needs and include a team of healthcare professionals who plan and coordinate the rehabilitation together with the patient. IRPs aim to support the patient in self-management strategies for coping with pain and disability and increasing their level of activity and participation in society (13). IRPs have been shown to positively influence the condition/situation of patients with WAD, with decreased pain, increased physical and psychological functioning, and improved quality of life (14).
Exercise is an important intervention in an IRP (12, 13). Persons with neck pain are recommended exercises targeting the specific impairments; cervical range of motion (ROM) (3), neuromuscular control and movement control (3, 7, 10, 15), postural stability (16), cervical position sense (16), movement sense (16) and head–eye coordination (including gaze stability) (16). Exercises in virtual reality (VR) have been shown to engage people with different chronic conditions, to stimulate increased physical activity, to improve exercise compliance and effectiveness (17, 18) and to increase patient satisfaction (19). One advantage of VR is that it directs attention to an external stimulus, rather than to the body (20), which has been shown to be effective in improving motor learning and performance (21). Training with VR improves pain (22), balance and function regarding mobility and speed in neck movements (19). A recent systematic review (24) concluded that VR improves general health, balance, pain intensity and disability in patients with chronic neck pain compared with conventional proprioceptive training, both at short- and long-term follow-up. Although these results are promising, there is a lack of high-quality studies (23) and studies investigating the feasibility of physical exercises in VR for chronic neck pain in a clinical context. Since IRP is a common treatment in patients with chronic neck pain, the feasibility of use of VR exercise interventions during IRP needs exploration. In addition, there is scarce knowledge of the patients’ experiences of exercising in VR and how this affects symptoms.
The objective of this study was to assess the feasibility of using VR exercises during an IRP for patients with chronic neck pain, by testing equipment and assessing symptoms and functioning. The specific aims were to assess symptom severity before and after each VR exercise; to investigate outcomes related to chronic neck pain after participating in the IRP; and to explore the participants’ experience of the VR exercises and equipment.
Participants
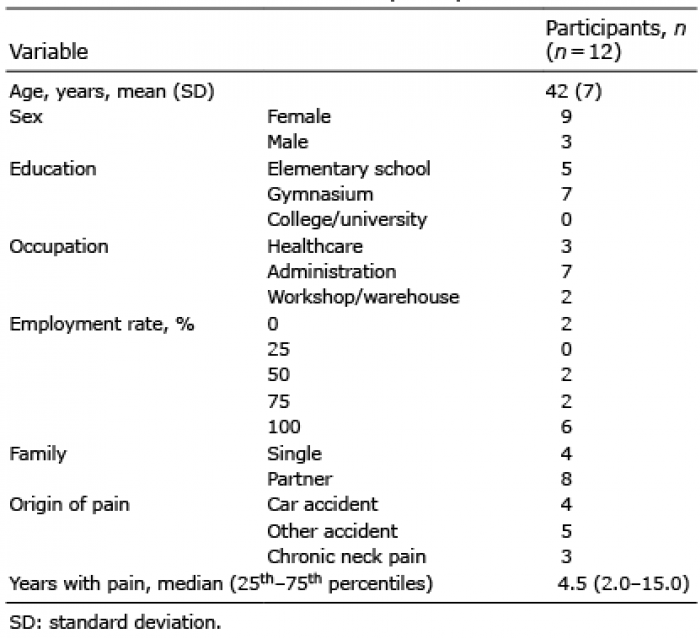
All 15 patients with chronic neck pain who were admitted to the IRP during the period October 2017 to May 2018, and who fulfilled the inclusion criteria, were invited to participate. Inclusion criteria were: age 18–65 years, with chronic neck pain, and participating in the IRP. Exclusion criteria were: WAD with confirmed neurological symptoms, extensive psychiatric problems, drug abuse and lack of knowledge of Swedish. One subject declined to participate prior to the first assessment and 2 discontinued the IRP due to long commuting distance and work situation (see Fig. 1). A final total of 12 patients was included in the study (Table I). Their mean age was 42 years, and 9 were female (75%). The median time with pain was 4.5 years and in 9 participants the cause of neck pain was WAD.
Interdisciplinary rehabilitation programme
The patients were referred to the IRP by their primary care physician. The IRP aimed to facilitate acceptance of the current situation and promote successive return to activities and participation in society. Initially, the patients were assessed by a team, comprising a physician specializing in pain and rehabilitation medicine, a psychologist, an occupational therapist, a physiotherapist, a social worker, and a nurse.
Table I. Baseline characteristics of participants
Fig. 1. Study flow chart, showing the interdisciplinary rehabilitation programme (IRP) (team assessment, interdisciplinary rehabilitation programme (IRP) introduction, comprehensive IRP and evaluation after IRP), assessments and drop-outs. Assessment before IRP: assessments before and after virtual reality exercise sessions when the participants rated the severity of symptoms on a numerical rating scale (NRS). Participants also answered questionnaires before the IRP (the Euro-Qual 5-dimension scale (EQ-5D index and visual analogue scale (VAS)), the Hospital Anxiety and Depression Scale (HADS), the Insomnia Index, the Tampa Scale of Kinesiophobia (TSK) and the Neck Disability Index (NDI). Assessments during the IRP: the participants rated symptom severity before and after the VR exercises twice/week with a NRS: pain, dizziness, nausea, body fatigue, mental fatigue, stress, relaxation, and assessments after IRP, which were the same as before IRP, plus interviews regarding the participants’ experiences of exercising with virtual reality (VR)
After assessment, the patients took part in the IRP introduction (Fig. 1), 1 day a week for 3 weeks. They then participated in the comprehensive IRP for 6 weeks, 3 days a week (Fig. 1), between 09.00 h and 15.00 h. The IRP included education about pain physiology and mechanisms related to chronic neck pain, coping with pain, self-management, the relationship between pain, bodily signs/bodily signals, behaviour and emotions, how to balance between activity and rest, relaxation, recovery, body awareness, physical activity, ergonomics, and information on social rights. Each group comprised 8 patients. Each day of the IRP included physical activity, such as training in the gym, cardio training, stability training, walking, Nordic walking, and pool training.
Virtual reality exercise intervention including exercise levels
The VR exercises were performed according to the RecoVR®, an intervention developed in collaboration between the University Department of Rehabilitation Medicine, Danderyd Hospital, Stockholm, Sweden, the Department of Innovation in the Stockholm region and the company Evado, Luleå, Sweden (see Appendix I).
The VR exercises were visualized via a mobile phone placed in VR glasses, with a total weight of 0.5 kg (Fig. 2). The exercises were guided by an experienced physiotherapist and took approximately 10 min to perform, the whole session lasted approximately 20 min. The participant performed small, careful movements of the head, including flexion, extension and rotations involving mainly the upper cervical parts.
Fig. 2. Virtual reality (VR) glasses. Photograph: Johan Adelgren Danderyd Hospital, with permission
In the VR programme the movements were visualized to the participant via a disc, which moved according to the movements of the participant’s upper cervical spine. The VR programme was providing them with immediate feedback on their neck movements, by showing with a line how well their own movements followed the suggested path of movement. The movements were digital recorded and analysed by the VR-programme.
A menu of choices of exercises and within each exercise was displayed on the VR screen. The participant navigated and made choices, e.g. level of exercise and type of environment, by looking at the desired alternative and, at the same time, touching a control on the side of the VR glasses. The participant could choose depiction of different natural environments or of being in an empty room, and could choose from different background sounds (e.g nature, music, or silence).
During the exercises the participant sat in a quiet room on a stool with a cushion shaped like a wedge at an adjustable table, with the instruction to sit in a neutral position with relaxed shoulders and 90° flexion of the elbows, with the forearms resting on the table. The table was adjusted based on the participant’s height.
The VR intervention comprised 3 exercises:
1 Full range of motion of the neck in rotations, flexion and extension by moving a disc via movements of the head and eyes in different predetermined directions. There was no pre-programmed time, and the participant chose the pace.
2 Tracking the disc moving in a predetermined path; a horizontal figure-of-8, without moving outside the path (Fig. 3). The pre-programmed time for this exercise was approximately 40 s.
3 Starting with the head in a neutral position, finding the disc, when it appears in different places on the screen, by glancing with the eyes and moving it back to a centred position using their eye gaze , until the head is in the neutral position again. The pre-programmed time for this exercise was approximately 20 s/task.
Fig. 3. Exercise 2: Tracking the disc with the eyes, by moving the upper cervical spine, in a predetermined path; a horizontal figure-of-8, without moving outside the path. The text in the figure (varv ½) indicate the number of rows completed (1) and total numbers of rows to do (2).
Exercises 2 and 3 included 7 different levels, where level 1 was easiest and level 7 the most difficult. A higher level of difficulty was characterized by increased range of motion, faster movement speed and longer performance time. The level was increased when the participant completed an exercise without augmented pain and fatigue.
The VR exercise intervention was introduced at a separate meeting (session 1) and then performed twice a week for 6 weeks during the intensive part of the IRP, in accordance with a standardized protocol (sessions 2–13) that was individually tailored to each participant. The final exercise session was performed during the final assessment at the end of the IPR (session 14).
The participant performed the exercises in numerical order, commencing at the lowest level in exercises 2 and 3. The increase in level was individualized during the continuous follow-up process between the participant and the physiotherapist. The participant could stop at any time during the exercise session. The physiotherapist checked that the participant performed the exercise correctly and maintained the correct posture. Instructions were provided as needed throughout the training period.
Symptom severity before and after each session of virtual reality exercise
Symptoms common in chronic neck pain and WAD include neck pain, dizziness, nausea, body fatigue, mental fatigue, stress and difficulty relaxing. A questionnaire with a numerical rating scale (NRS) with the end points “no symptoms” and “worst possible symptoms” for each of those symptoms was answered by the participants before and after each of the 14 sessions of VR exercise.
Questionnaires with variables related to chronic neck pain: Swedish Quality Registry for Pain Rehabilitation and Neck Disability Index
As part of the clinical routine all the participants completed the Swedish Quality Registry for Pain Rehabilitation (SQRP) forms (24) prior to the IRP and before discharge. The SQRP forms consist of standardized, reliable and valid measures recommended to describe the health status of patients with chronic pain and to follow up outcomes of pain rehabilitation. The forms included questions about demographic background and for the evaluation of pain treatment (25), as follows:
Hospital Anxiety and Depression Scale (HADS), comprising 14 questions that provide answers to 2 different subscales for anxiety and depression (26).
Self-assessment of psychosocial and behaviour-related consequences of prolonged pain, with 4 subscales from the Multidimensional Pain Inventory (MPI) (supporting, punishing, solicitous, and distracting responses of significant others), scored on a 7-point scale, higher scores indicating higher level of responses from significant others on each subscale, respectively (27).
Health-related quality of life, as measured by the EuroQol-5 Dimensions (EQ-5D); the EQ-5D consists of 5 questions, which estimate physical/psychological function, as well as activity, and a health barometer. A weighted index of quality of life is produced based on the answers to the questions (28).
Sleep problems, as measured by the Insomnia Severity Index (ISI), a screening for people with insomnia, comprising 7 questions scored from 0 to 5. Higher scores indicate more severe sleep problems (29).
Kinesiophobia as measured by the Tampa Scale of Kinesiophobia (TSK). The TSK measures perceived fear of (re)injury and movement on a 4-point scale; higher scores indicate greater fear of movement (30).
In addition to the SQRP, the patient completed the Neck Disability Index (NDI) prior to the IRP and at discharge. The NDI consists of 10 questions scored from 0 to 5; higher scores indicating higher self-rated disability due to neck pain (31).
Participants’ experiences; interviews
The first author (MG), a physiotherapist, who was not involved in the IRP, interviewed the participants with open questions on the final exercise session before discharge. The questions concerned the VR equipment, the VR environment, different aspects of the VR exercise intervention, the experiences of exercising with VR (positively and negatively), and how the exercises affected symptoms.
The participants’ answers were written down during the interview. MG analysed the text with a deductive approach, by categorizing the content in themes and summarizing the themes.
Data analyses and statistical analysis
Since all data were considered as non-parametric, Wilcoxon signed-rank test and Friedman’s test were used for analysis. The rating of symptom severity before and after each exercise session was analysed with the Wilcoxon signed-rank test. The overall difference between all the ratings of pain and dizziness before and after the exercise, respectively session sequence numbers 1–14 before and session sequence numbers 1–14 after was analysed with Friedman’s test. Ratings of symptom severity were also analysed visually via curve diagrams of all 12 exercise sessions, with 1 diagram for the ratings before the exercise and 1 for the ratings after the exercise, with 1 curve representing each participant (the first and last sessions were excluded, as the participant followed a standardized protocol affecting the levels reached). The NDI and the SQRP questionnaires were analysed from before to after the IRP with the Wilcoxon signed-rank test. For statistical significance a level of p ≤ 0.05 was chosen. SPSS for Windows version 22.0 (SPSS Inc. Chicago, IL, USA) was used for all statistical analyses.
Ethics considerations
All participants were informed orally and in writing about the VR exercises and the study, and gave their written consent. The study was approved by the Regional Ethical Review Board in Stockholm (D-nr 2016 71700-31/4).
Feasibility
The participants performed and completed the VR exercises according to the IPR plan, thus confirming the feasibility of use of the VR exercises during the IRP in the clinical setting.
Level of virtual reality exercise reached at each session
The level of difficulty reached by each participant for exercises 2 and 3, respectively, and that obtained between sessions 2 and 13 is shown in Table II. The level of exercise varied between exercise sessions, and most participants increased their level to a higher degree of difficulty during the exercise period (Table II).
Sessions 1 and 14 were performed according to a standardized protocol, with the level of difficulty for the exercises set out in a specific order. This protocol was found to affect the levels reached; therefore, these 2 exercise sessions were excluded from the analysis.
Table II. Level reached by each individual in exercises 2 and 3 in exercise sessions 2–13. The exercises comprised 7 levels; level 1 was the easiest and level 7 the most difficult. A higher level of difficulty was characterized by increased range of motion, faster movement speed, and longer performance time
Symptom severity before and after each virtual reality exercise
Seven symptoms that are common in neck pain were rated before and after each session of VR exercise. Among the participants, dizziness (12 out of 12 exercise sessions) and pain (6 out of 12 exercise sessions), increased significantly during the VR exercises (Table III). The other symptoms (nausea, bodily fatigue, mental fatigue, stress and tiredness) increased significantly during a few sessions (3 or fewer), whereas the feeling of difficulty relaxing decreased during a few sessions.
Table III. Ratings of dizziness and pain, median values and range of 25th and 75th interquartile range (IQR) on the numerical rating scale (NRS) (scale steps 0–10, 0 indicating no symptom, 10 indicating worst possible symptom), before and after each exercise session.
Symptom severity, changes in dizziness and pain from assessments 1 to 14
No significant change over time was seen in ratings of symptom severity from before to after the IRP (assessments were made before and after each of the 14 sessions) regarding dizziness (before first exercise session, assessment 1, compared with before last exercise session, assessment 14: (p = 0.70)) (after assessment 1 compared with after assessment 14: (p = 0.64)) or pain (before assessment 1 compared with before assessment 14: (p = 0.73)) (after assessment 1 compared with after assessment 14 (p = 0.77)).
Individual curves illustrating ratings of dizziness and pain
Individual curves from before and after exercise illustrate the variation in each participant’s ratings of dizziness (Fig. 4) and pain (Fig. 5).
Most participants rated dizziness at a low level before exercise (Fig. 4a), with a small increase after exercise (Fig. 4b). Four participants (1001, 1004, 1006, 1010) rated no dizziness either before or after exercises, therefore their ratings are not visible in the diagrams. The ratings of 2 participants (1002 and 1007) show dizziness at a constant high level both before and after the exercises.
Fig. 5 shows the ratings of pain, which for most participants vary between high and low ratings before (Fig. 5a) as well as after the exercises (Fig. 5b). Three participants rated pain as constant, on a high level both before and after the exercises, indicating (1002, 1004, 1007) a stable pattern of more severe pain.
Two participants (1002 and 1007) rated constantly high levels of both pain and dizziness.
Fig. 4. The individual ratings of dizziness (scale steps 0–10, 0 indicating no symptom, 10 indicating worst possible symptom) (a) before and (b) after the 12 exercise sessions during the 6 weeks IRP. ID number indicates the number and colour in the diagram of each individual participant.
Fig. 5. The individual ratings of pain (scale steps 0–10, 0 indicating no symptom, 10 indicating worst possible symptom) (a) before and (b) after the 12 exercise sessions during the 6 weeks IRP. Key indicates the ID number and colour on the diagram of each individual participant.
Questionnaires with variables related to chronic neck pain: Swedish Quality Registry for Pain Rehabilitation and Neck Disability Index
Significant improvements were seen after IRP in HADS depression (p = 0.023), MPI pain-related life interference (p = 0.019), MPI life control (p = 0.025), EQ-5D Index (p = 0.005), ISI (insomnia) (p = 0.050) and TSK (kinesiophobia) (p = 0.011) (Table IV). No change was seen in HADS anxiety, MPI pain severity, MPI affective distress, present health state (EQ-5D VAS) or NDI.
Table IV. Variables from the Swedish Quality Register for Pain (SQPR) and Neck Disability Index (NDI) before and after the interdisciplinary rehabilitation programme (IRP).
Participants’ experiences: interviews
Participants’ answers to the interview questions were summarized according to topic, and are presented below with example quotes.
Virtual reality equipment and programme design. Use of the VR equipment was perceived as both positive and negative. Positive factors were that VR added a dimension of playfulness and gaming to the exercise. VR also provided the users with the opportunity to gain direct feedback from the VR programme about individual movement quality and the level of exercise reached on each occasion. A negative factor was that the VR glasses were heavy to wear.
Good to get feedback, don’t get it without the game [woman: pain duration one year due to accident]
A little too heavy when you are already suffering from fatigue in the neck [woman: pain duration 11 years due to myalgia]
On the whole, participants described the game length as appropriate. Game length could also be experienced differently on different days, depending on how they felt.
It felt good, but on my worse days it felt too much. Overall, time is alright. The game length is OK [man: pain duration 31 years due to accident]
The environment could be perceived as beautiful and soothing, but also as somewhat boring. The participants suggested improvements, such as including more variation in the game environments.
Good environment. Soothing environment and soothing sounds. Have tried the sea and the garden [woman: pain duration 2 years due to accident]
Focus and motivation. VR training required focus and presence, which could be challenging, as maintaining focus could be a difficulty. Motivation to undertake training increased, as the VR environment provided a positive experience and feedback on performance; hence performing the exercises became more enjoyable in VR. The participants attempted to perform the exercises correctly. Motivation to achieve a better result from the exercises increased as the exercise levels increased. A belief that the training would provide a positive effect and the desire to continue with training after completion of rehabilitation was expressed. Eleven out of 12 participants reported that they would like to try the exercises again, at home, or with their physiotherapist at the clinic.
A positive experience, a more fun way to exercise instead of just sitting on a chair. Easier to do when it is so visual, a purposeful task [woman, pain duration 2 years due to accident]
Becomes more tiring afterwards, probably due to the fact that the game requires great focus and concentration which is difficult for me [woman: pain duration 16 years due to myalgia]
Symptoms, awareness and confirmation of own problems. The participants’ perceived symptoms in connection with and after exercise could be pain, dizziness, fatigue in body and mind and general fatigue. The participants explained that the increasing number of different symptoms could hinder them in undertaking exercise, or, conversely, the symptoms could disappear for a while after the training session.
More feeling of dizziness but I have dizziness anyway, also when it is difficult to find orientation points. It goes back after a little while [woman: pain duration one year due to accident]
I usually do not try to move my neck, but when I do this, I get increased pain afterwards, but it is gone after 10 to 15 min [woman, pain duration 16 years due to myalgia]
The VR training not only confirmed the participants’ problems, but also made them more aware of their problems. Their neck and back problems became more apparent, which was experienced both positively and negatively. With increased awareness, the participants also described how they adapted to find their level of training.
I’m not exaggerating my problems, I have something to work with, it is not only in my head [woman: pain duration one year due to accident]
It feels negative when you are reminded that you have problems with your neck and back [man: pain duration 2 years due to accident]
To Dare. The participants were curious about the training, and described how the exercise made them dare to stretch the boundaries and perform movements that they would otherwise avoid.
Exercising with neck movements, using the muscles I avoid using, pushes the boundaries [woman: pain duration 16 years due to myalgia]
[I] have tried to follow things at home on the TV [woman: pain duration 2 years due to accident]
To our knowledge, this is the first study to explore the feasibility of use of a VR exercise intervention during IRP for patients with chronic neck pain, including assessment of the experience of the participants. The results showed that the use of VR exercises is feasible and safe as part of an IRP for patients with chronic pain. The exercises worked well within the frame of the IRP and the patients did not report any long-term side-effects. The ratings of dizziness and pain before and after the single sessions of VR exercise showed recurrent increase in symptoms, but no long-lasting deterioration in symptoms. The participants described that the VR exercises motivated them to train, provided helpful direct feedback of their movement performance, and of the level they could manage on that specific day. The VR programme also made them aware of and illustrated their problems when they tried different levels of exercise, which confirmed the problems they experienced. Negative factors reported were the weight of the glasses, increase in symptoms, and being reminded of their current problems.
Symptom severity before and after each VR exercise
Dizziness and other symptoms, which might be regarded as vestibular, are common, and might be a severe problem for patients with WAD (4). True vertigo is rarely described in WAD (4); it is usually described as a vague unsteadiness and light-headedness. In the current study, dizziness was the most commonly increased symptom, although it occurred at a low level, during exercising, while other vestibular symptoms, including nausea, seldom increased. This result is in agreement with earlier research, in which increased neck pain, neck-related movements and activity were exacerbating factors (7).
The increase in pain during the VR exercises is understandable in the light of current knowledge about pain physiology. Several chronic pain conditions are associated with increase in pain during and after exercise, which could be explained by a lack of inhibition and enhanced excitability in central nervous system (CNS) processing of pain. The balance between inhibition and excitation in the CNS determines whether exercise will promote analgesia or promote pain (32). In chronic WAD cervical dysfunction only partly explains the symptoms, and impaired central pain processing plays a crucial role (33). Patients with WAD have demonstrated decreased pain thresholds and shown symptom flares in response to aerobic exercise. The release of endorphins and activation of other brain-orchestrated pain inhibitory mechanisms seems to be dysfunctional (34). Treatment of this patient group through exercise is a balancing act, with too little exercise averting beneficial effects and too much exercise aggravating symptoms.
In an earlier study, patients with chronic neck pain undertook kinematic training in VR, including active neck movements to increase ROM, rapid head movement between targets to facilitate rapid cervical motion control, and smooth head movement following a target to train accurate neck movement. The results showed increased function regarding mobility and speed in neck movements, and improved balance and increased patient satisfaction compared with kinematic training without VR (19). In a recently published pilot-study patients with non-traumatic chronic neck pain practiced sensorimotor training with a VR device in combination with a standard rehabilitation programme (35). The results were compared with those for patients who did not receive training with a VR device. The additional VR training showed positive effects in improving headache and the active range of movement in flexion and extension. In the current study the exercises aimed to target these functional movements, but it was not possible to measure motion control; these facilities are still in development. VR provides new opportunities in these respects and can also be used to provide feedback for correction and monitoring for the clinician (36).
Questionnaires with variables related to chronic neck pain: Swedish Quality Registry for Pain Rehabilitation and Neck Disability Index
Although this study did not explore whether VR exercises add extra benefits to the IRP for the participants, the results indicate greater improvements in HADS Depression and MPI pain-related life interference compared with a recently published follow-up study from our department of IRP for patients with WAD (37). However, the current sample is too small to make any adequate comparison. The current results, however, show that the addition of VR exercises did not adversely affect the results of the IRP. The improvements in the SQPR questionnaires after the IRP are in line with earlier research, in which IRP results in decreased pain, increased physical and psychological functioning, and improved quality of life (14, 38).
The results after the VR exercise programme are encouraging, even though the participants’ ratings of pain and dizziness deteriorated temporarily after the single VR exercises. It has been shown previously that the VR environment positively affects pain and anxiety levels in other groups of patients (39). In the current study, kinesiophobia decreased after IRP, while pain was often increased after the exercises. A possible explanation for this finding could be that, despite an increase in pain, the participants gained greater confidence in their ability to perform physical activity and neck movements.
The NDI showed no change after IRP, although some of the improved SQRP variables measure similar factors, such as the NDI (pain interference (MPI) and sleep (ISI). However, a possible explanation for this is that pain severity (MPI) did not improve, and several NDI variables relate to the impact of activities on pain severity.
Participants’ experiences: interviews
The participants reported that the VR intervention motivated them to exercise in many ways; it provided feedback, the levels encouraged them to reach a higher level, and it was important to perform the exercises correctly. The only negative effect noted was that the device was experienced as heavy, which was also observed in the study by Nusser et al. (35).
The VR environment was perceived as both calming and somewhat boring. A calm environment was one of the targets in the development of the intervention; hence natural environments were chosen. The VR environment can positively affect body temperature and pulse rate, which indicates increased relaxation and wellbeing (18). Data from the interviews and the symptom ratings both indicate that the current VR environment succeeded in creating a calm setting. Except for a few sessions, the participants did not increase their ratings of stress, tiredness, mental or bodily fatigue, despite the fact that they performed the exercises for 30 min.
Training in a VR environment has been shown to be engaging, to motivate physical activities, and to improve exercise compliance and effectiveness (18, 36). The participants in the current study reported that the VR training made them aware of their limitations, that it was possible, but difficult, to adjust the level of exercise, and it could be negative when the exercises reminded them of their own difficulties.
Methodological considerations
This study has several strengths and limitations. The agile development process and the feasibility study were conducted in a clinical context with available clinical resources. For practical reasons, the participant group in this study was small and there was no control group. To reduce risk of bias, one physiotherapist was responsible for the VR training and another applied the assessments of symptoms and the interviews for the evaluation of the VR training in the IRP. A limitation of this study is that the physiotherapist who performed the assessments was also involved as a leader of group discussions and other exercises in the IRP programme, although not in the VR exercise intervention.
A strength of this study was the clinical context. By conducting the study in an everyday clinical setting, it was possible to capture all the problems encountered in the clinic. Understanding the participants’ experiences of using the equipment, being in the VR environment, and performing the exercises was important both during development and during the study.
Some studies have demonstrated an association between range, velocity and smoothness of cervical motion and patients’ subjective reports of pain intensity and disability, and fear of neck motion (40); others have not found these associations (10). Unfortunately, these measurements were not within the scope of the current study, since the VR intervention used did not allow such data collection. These aspects are important for the future development of VR equipment.
Future research
The evidence does not clearly suggest a superior exercise intervention for patients with chronic WAD. Most studies report small effect sizes, suggesting that a small clinical effect can be expected from exercise alone (40). VR offers opportunities for the further development of devices for use in tele-medicine and the remote assessment and training of cervical kinematics in patients with chronic neck pain. VR is also easily accessible and commercially available. Further research is needed to address which patient groups could benefit from this type of training, and how the VR environment and exercises can be designed to achieve optimum treatment benefits.
Conclusion
This study indicates that performing VR exercises is feasible and safe as part of an IRP for patients with chronic neck pain. The patient’s symptoms may worsen during the exercises, which stress the importance of individual adjustments, but no long-lasting impairment would be expected. No adverse effects occurred due to the interdisciplinary rehabilitation programme. The VR exercises might support participants by increasing their motivation to exercise and providing useful feedback. However, further research is necessary in order to determine the long-term effects of the use of VR exercises in IRP for patients with chronic neck pain.
Appendix I. Development of the virtual reality exercise intervention.
Fig. 6. The agile development process of the virtual reality (VR) exercises. The same process was used in both versions.


 Click to show fullsize
Click to show fullsize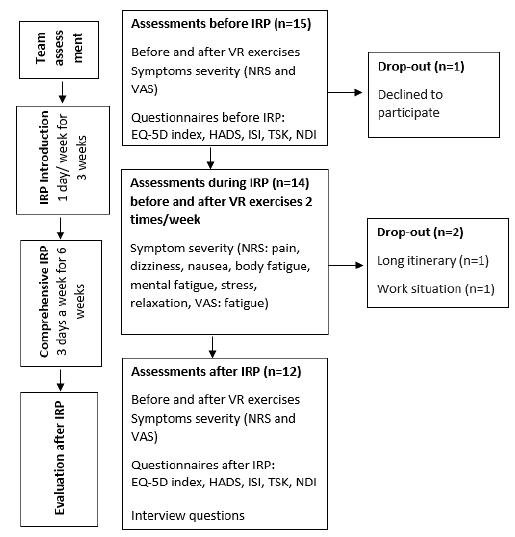 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize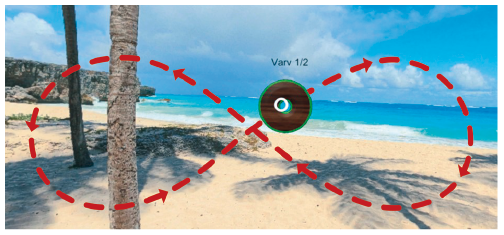 Click to show fullsize
Click to show fullsize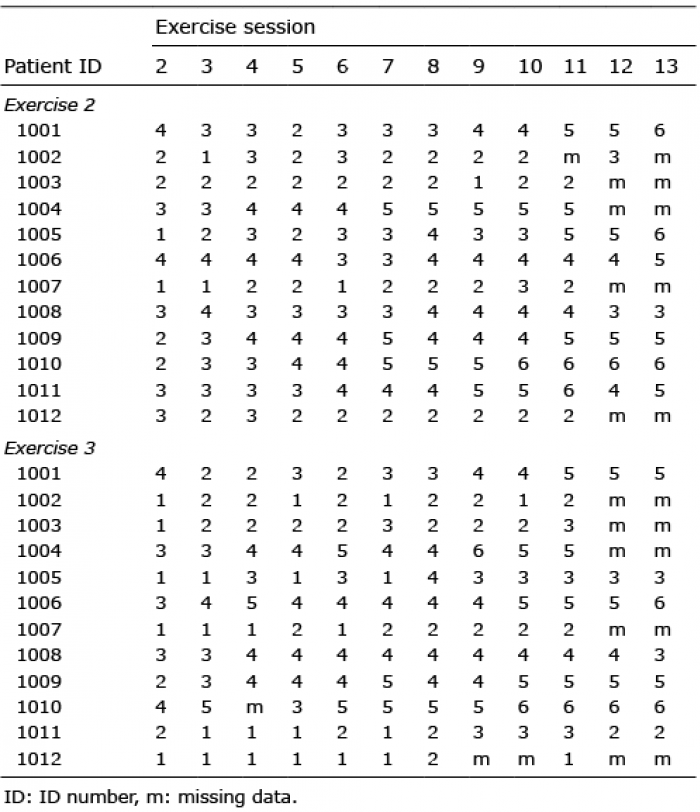 Click to show fullsize
Click to show fullsize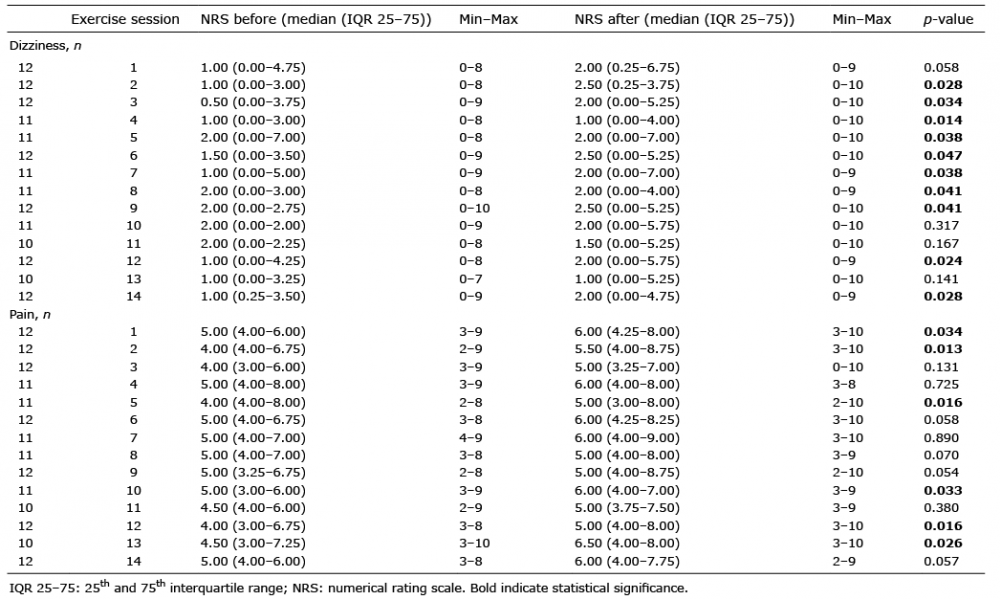 Click to show fullsize
Click to show fullsize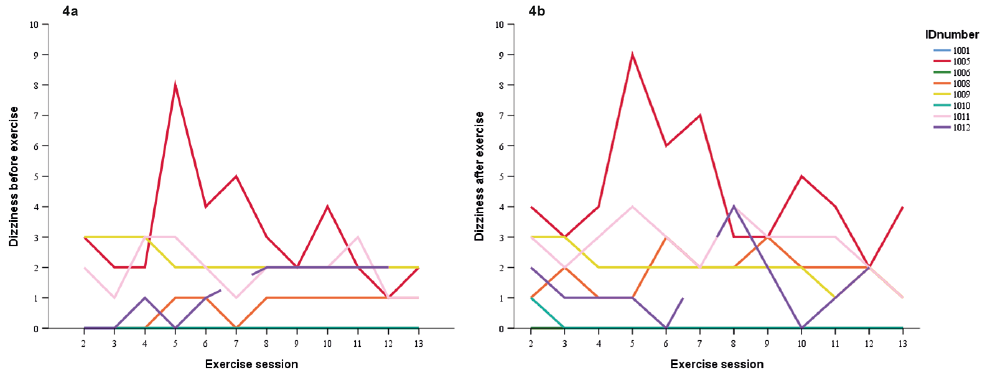 Click to show fullsize
Click to show fullsize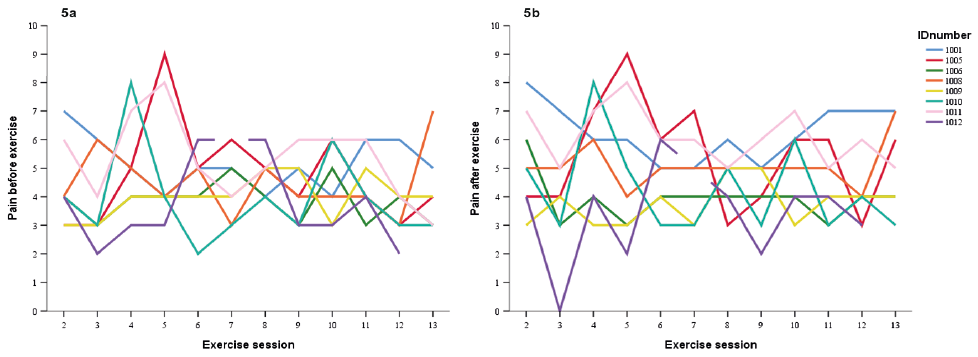 Click to show fullsize
Click to show fullsize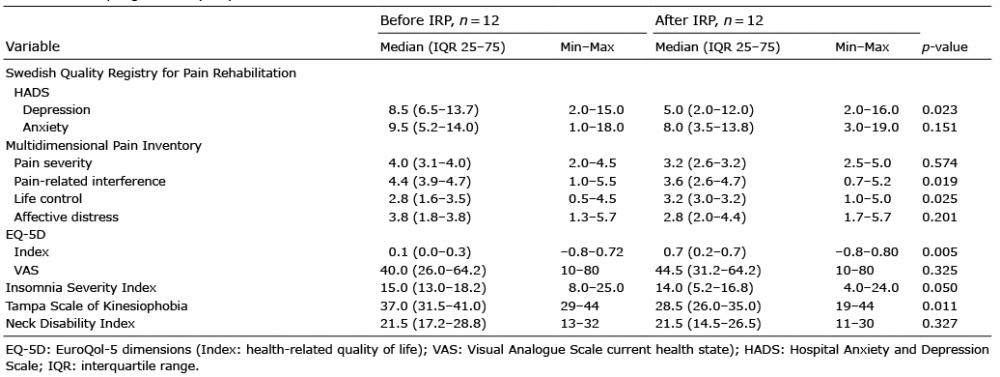 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize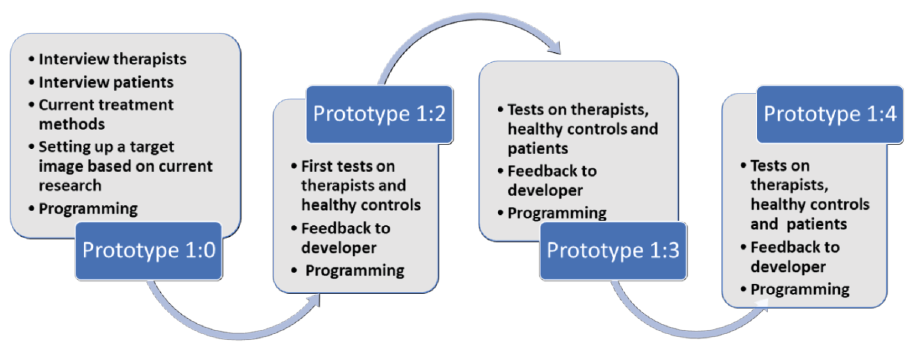 Click to show fullsize
Click to show fullsize