
1Department of Rehabilitation, Kunshan Rehabilitation Hospital, Kunshan, China
2Department of Nursing, Jen Ching Memorial Hospital, Kunshan, China
3Department of Science and Technology, Nanjing First Hospital, Nanjing Medical University, Nanjing, China
In China, the stable type of fifth metatarsal base fracture is usually treated by rehabilitation methods after the limbs have been fixed for approximately 4 weeks. A 37-year-old woman fractured her fifth metatarsal base, with a stable fracture type. From the second day of the fracture onward, she agreed to participate in rehabilitative treatment that did not involve surgery or long-term fixation. Fourteen days after the fracture, the patient was able to bear 100% of her body weight and stand for 20 min in a normal posture with supportive elbow crutches. She was able to return to work with double elbow crutches after 25 days. On the 30th day after the fracture, the patient was able to walk 300 m outdoors without any walking aids and with no discomfort. Two months after the fracture, the patient went jogging and was participating in all of her normal daily activities. This case shows that, for stable type fractures of the fifth metatarsal base, rehabilitation starting on the second day after the fracture can help accelerate the patient’s return to normal physical activities.
key words: fracture; fifth metatarsal base; rehabilitation
Accepted Jul 24, 2021; Published Sep 10, 2021
JRM-CC 2021; 4: jrmcc00068
Correspondence address: Aicui Lin, Nanjing First Hospital, Nanjing Medical University, Changle Road 68#, Nanjing, Jiangsu, 210006, China. E-mail: linaicui@126.com
Doi: 10.2340/20030711-1000068
In China, the stable type of fifth metatarsal base fracture is usually treated by rehabilitation methods after the limbs have been fixed for approximately 4 weeks. A 37-year-old female agreed to undergo rehabilitation treatment, without surgery or long-term fixation, from the second day of the fracture onward. Fourteen days after the fracture, the patient was able to bear 100% of her body weight and stand for 20 min in a normal posture with supportive elbow crutches. She was able to return to work with double elbow crutches on the 25th day. On the 30th day after the fracture, the patient was able to walk 300 m outdoors without any walking aids, and with no any discomfort. Two months after the fracture, the patient went jogging and was participating in all of her normal daily activities.
Fractures of the fifth metatarsal bone are one of the most frequent fractures to the foot and ankle (1). Such fractures are considered to be relatively innocuous (2, 3). Some surgeons prefer an open reduction and internal fixation (4–7) for fractures of the fifth metatarsal. In China, for the stable type of fifth metatarsal base fractures, orthopaedists perform surgery and often fix the foot with a slight eversion angle by cross-joint cast for 4 weeks, which is considered to be conservative treatment. However, rehabilitation physicians prefer to fix the foot in a neutral position, and rehabilitation therapy of the stable type of fifth metatarsal base fractures often begins 4 weeks after orthopaedic fixation, in consideration of safety. To the best of our knowledge, this case is the first report describing early rehabilitation training for a patient with a fifth metatarsal base fracture in China.
Case information
On 10 June 2019, a 37-year-old female nurse injured her left foot when she was descending a stairway. Because she could not move the injured foot, X-ray imaging was performed immediately. The X-ray showed fractures of the fifth metatarsal base (Fig. 1). After diagnosis by an orthopaedist (works in Jen Ching Memorial Hospital), her foot was fixed in the functional position with a cross-joint brace, with the ankle slightly everted. Local cooling was applied. Drugs for promoting blood circulation and removing blood stasis, as well as painkillers, were used. The orthopaedist asked the patient to return for further consultation on the 4th day, in order to determine whether surgery was necessary. However, the patient transferred to Kunshan Rehabilitation Hospital.
Treatment and results
Day 1 post-fracture. Rehabilitation treatment was initiated after obtaining informed consent,. The injured left foot was protected with a brace, and the patient was asked to lie on a bed, with her injured foot raised to the same level as her heart. Continuous local cooling was applied. Pain and swelling were monitored continually and minimized by the use of various treatments.
Day 2 post-fracture. The injured left foot was continually maintained in a raised position at the same height as that of the heart. Fifteen minutes local cooling was applied with intervals from 0.5 to 1 hour. Pain and swelling were continually monitored. With the protection of a brace, the patient was instructed to engage the ankle joint in dorsiflexion and plantar flexion. The patient was then trained to perform isometric contraction when dorsiflexion and plantar flexion of the metatarsophalangeal joint were performed, 10 times/set, 3 sets/day. Flexion and extension resistance movement of the knee joint was performed, 10 times/set, 3 sets/day. Bedside sitting training lasted only 10 min, with the injured limb on a platform to avoid the discomfort of foot drop. Because the patient was not confident about performing the bedside sitting training, and had not had good rest after the injury, the bedside sitting training was stopped, and the therapy was changed to lying on the bed.
Day 3 post-fracture. There was 2 × 6 cm ecchymosis under the skin on the lateral side of the injured foot. Local slight swelling was observed around the ecchymosis without pain. Kinesio tape was applied from the calf to the foot, and taped in the shape of a claw on the back of the foot. The injured foot was continually raised to heart level, but local cooling was stopped. Because the patient reported a significant sensation of swelling in the ankle joint when plantar flexion occurred and a stretched feeling when dorsiflexion occurred, passive movement of the ankle was performed to stretch the triceps and prevent the triceps from contraction. The strength of the stretch was based on patient feedback regarding the sensation. The training lasted 2 min/set, with 5 sets/day. Active dorsiflexion training without ankle resistance was performed 5 s/time, 10 times/set, and 3 sets/day. Weightless standing training with a hand-held walker lasted 10 min. The patient did not report any discomfort. X-ray imaging did not show any change (Fig. 2).
Fig. 1. X-ray on day 1 after the injury. Fig. 2. X-ray on day 3 post-fracture.
Day 4 post-fracture. The ecchymosis under the skin reduced, then thermotherapy was applied. Weightless standing training lasted 10 min. Under guidance from a therapist, therapy was implemented for 2–3 min with 5 min rest, 5 times/day, consisting of the patient standing with a hand-held walker while bearing 10% of her weight. To prevent displacement of the fractured section, the ankle was placed in a neutral position, and the heel became the load-bearing part of the foot. The patient did not report any discomfort.
Days 5–8 post-fracture. The patient performed a full range of active movements of the left ankle joint, knee joint, and hip joint, 10 times/set, and 3 sets/day. Balance training and extended standing to build endurance were practiced with a hand-held walker. With the protection of the hand-held walker, the patient practiced indoor walking. The training time was gradual, and eventually was extended from 20 min. On day 8 post-fracture, the patient was able to bear 50% of her body weight in a normal stressed position and gave a 1-h job-related lecture while standing, with no obvious discomfort.
Days 9–15 post-fracture. The patient performed a full range of resistance exercises of the left ankle joint, knee joint, and hip joint, 10 times/set and 3 sets/day. When the patient was able to independently and safely walk with a hand-held walker, standing balance training and walking training under partial body weight load with bilateral elbow crutches was practiced. The training time was gradually extended from 10 min. Left lower limb weight-bearing training and endurance training was implemented. On the 14th day, the patient was able to bear 100% of her body weight and stand for 20 min with a normal posture using elbow crutches (Fig. 3).
Days 16–20 post-fracture. The patient practiced balance with elbow crutches, 5 min/set and 5 sets/day. Weight-bearing exercises during different parts of the walking cycle lasted 20 min every day. Outdoor walking training was performed with double elbow crutches, and the walking distance was gradually increased from 100 m using 2-point walking. X-ray imaging after the 17th day did not show any change (Fig. 4).
Fig. 3. On the 14th day, the patient was able to bear 100% of her body weight and stand for 20 min with normal posture using elbow crutches. Fig. 4. X-ray imaging of the patient on the 17th day post-fracture.
Days 21–25 post-fracture. The patient practiced moving up and down stairs with elbow crutches. Walking endurance training with double elbow crutches and on different types of outdoor ground surfaces was performed. The patient returned to work with double elbow crutches on the 25th day (Fig. 5).
Days 26–55 post-fracture. From the 26th to the 30th day, the patient’s training transitioned from walking with double elbow crutches to walking without crutches. On the 30th day, the patient was able to walk 300 m outdoors without walking aids and with no discomfort. Because it was necessary for the patient to travel to another city, the therapist performed functional assessment of the patient and assessed the walking circumstances and distance that would be required, and then engaged the patient in 5 days of proprioception training of the ankle, 20 min/day; independent walking balance training, 10 min/day; and walking endurance training, 30 min/day. On the 35th day, the patient travelled independently and with no discomfort (Fig. 6).
Fig. 5. The patient was able to return to work with double elbow crutches on the 25th day. Fig. 6. The patient travelled independently and unassisted on the 35th day, with no discomfort.
Proprioception training of the ankles, fast response training in the standing position, curve walking training with different interfaces and obstacles, and fast turn-back training were carried out from the 36th day. On the 55th day, no joint abnormalities were detected during the rehabilitation assessment, the strength of all the muscles reached to grade 5, and daily activities and ability to participate in sports were restored. Professional rehabilitation training was then stopped.
Third months from post-fracture. The patient went jogging, and resumed all of her daily activities. X-ray imaging on the 80th day after the injury did not show any abnormalities of the fracture (Fig. 7).
One and a half years after post-fracture. The patients had an X-ray examination and X-ray imaging showed that the fracture line had healed (Fig. 8).
Fig. 7. X-ray on the 80th day post-fracture. Fig. 8. X-ray 1.5 years post-fracture.
Immobilization and bed rest after fracture may lead to deep vein thrombosis, pulmonary embolism (8), and joint stiffness (9). Joint stiffness occurs because of the long immobilization time required due to the fracture site, as well as relative joint adhesion and ligament contracture. Because lengthy fixation with a cast can lead to joint stiffness and a poor functional outcome after the injury (9), modern rehabilitation practices advocate early intervention. Moving the ankle after bone breakage in the foot is very important to prevent ankle bone stiffness, muscle contracture, atrophy, and improve the functioning of the ankle (10). However, in China, the rehabilitation treatment provided to patients with this type of injury is conservative for medical safety. In this case, the patient received rehabilitation training at the early stage of injury.
The patient received early fixation when the affected limb was in the inflammatory phase, and subsequent active and passive joint activity promoted blood circulation, accelerated the exudation of inflammatory substances and absorption of necrotic tissues, and reduced oedema and adhesion. In the next phase of rehabilitation, the therapist trained the patient so that there was no pain, and weight-bearing in the early stage can prevent adhesions of joints and excessive contracture of ligaments, which are factors that are important to the recovery of joint mobility. After that, the daily activities and functional training assisted by the walking device prevented the disuse of local muscles and loss of strength, which accelerated the rehabilitation.
The limitation of this case report is that the rehabilitation programme was used with only 1 patient with a stable type fracture of the fifth metatarsal base; further research is necessary to determine the wider scope of application this rehabilitation.
The rehabilitation process used in this case showed that, with a stable type fracture of the fifth metatarsal base, rehabilitation could be carried out successfully starting from the second day after the fracture, and it assisted in accelerating the rehabilitation of the foot.
The authors thank LetPub (www.letpub.com) for linguistic assistance during the preparation of this manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize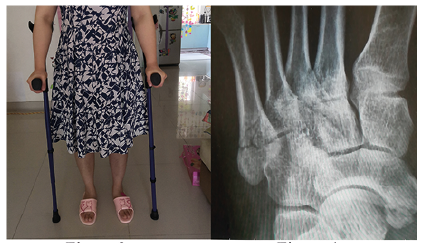 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize