
1Department of Cardiology and 2Department of Physiotherapy, The University of Hong Kong-Shenzhen Hospital, Shenzhen, Guangdong, China
Case report: We report the effect of a 6-week outpatient (phase II) cardiac rehabilitation in a 38-year-old man with post-stented coarctation of the aorta, moyamoya disease and hypertension. The cardiac rehabilitation programme comprised physiotherapist-guided aerobic exercises, resistance training and relaxation exercises. Clinical and functional assessment was performed before and after the cardiac rehabilitation programme.
Discussion: There is a lack of recommendations to guide cardiac rehabilitation in patients with coarctation of the aorta. This case not only had coarctation of the aorta, but also had moyamoya disease and hypertension. A cardiac rehabilitation programme after surgery provided meaningful improvements in all outcomes, including exercise capacity, clinical outcomes, quality of life and depression symptoms. Systematic cardiac rehabilitation was found to be feasible in this patient with coarctation of the aorta, and may have the potential to benefit more patients.
Conclusion: Cardiac rehabilitation resulted in significant clinical and functional improvements in this case with coarctation of the aorta following surgery. Guidelines should be implemented to provide safe and effective cardiac rehabilitation in such patients. Furthermore, large-scale studies are needed to evaluate the clinical benefits of structured cardiac rehabilitation in patients following cardiac surgery.
Key words: outpatient cardiac rehabilitation; coarctation of the aorta; moyamoya disease; exercise capacity.
Accepted Sep 7, 2021; Published Oct 15, 2021
JRM-CC; 4: jrmcc00070
Correspondence address: Cong Chen, The University of Hong Kong-Shenzhen Hospital, Haiyuan Road No.1, Futian District, Shenzhen City, Guangdong Province, China. E-mail: chenc6@hku-szh.org
Doi: 10.2340/20030711-1000069
This case report describes the effect of a 6-week outpatient cardiac rehabilitation in a 38-year-old man with coarctation of the aorta, moyamoya disease and hypertension. The cardiac rehabilitation programme comprised physiotherapist-guided aerobic exercises, resistance training and relaxation exercises. Clinical and functional assessment was performed before and after the cardiac rehabilitation programme. There is a lack of recommendations to guide cardiac rehabilitation in patients with coarctation of the aorta. Cardiac rehabilitation provided significant clinical and functional improvements, including exercise capacity, clinical outcomes, quality of life and depression symptoms, in this patient with coarctation of the aorta following surgery. Systematic cardiac rehabilitation was found to be feasible in this patient with coarctation of the aorta, and may have the potential to benefit more patients. Guidelines should be implemented to provide safe and effective cardiac rehabilitation in such patients.
A 38-year-old man, with a clinical history of refractory hypertension (grade 3) for 10 years, was diagnosed with coarctation of the aorta (CoA) by digital subtraction angiography measurement in 2018. In addition, he had underlying atherosclerosis (cerebral artery and carotid artery), aortic valve insufficiency (mild) and moyamoya disease. Surgery was performed to dilate the narrowing area, by implanting a 3.4-cm covered CP stent (NuMED, CVRDCP8Z34, NY, USA) (CP) stent and a 20-mm balloon into the aorta, which lead to a normal blood flow through the artery. The patient was referred to our cardiac rehabilitation (CR) clinic 6 weeks after surgery, reporting general malaise, low exercise tolerance and anxiety. Detailed information about the risks of exercise training was provided and written consent was obtained before commencing CR. In order to develop a personalized exercise prescription, the patient underwent clinical examination, including a 6-min walk test, cardiopulmonary test (CPET), echocardiography, 24-h ambulatory electrocardiograph, physical therapy and nursing evaluation, a series of intake evaluations, including medical and dietary intake and body fat assessment. Exercise intensity was planned based on the initial results of all evaluations. The rehabilitation goals were for the patient to increase his aerobic capacity and resume normal activities for a full return to living and work.
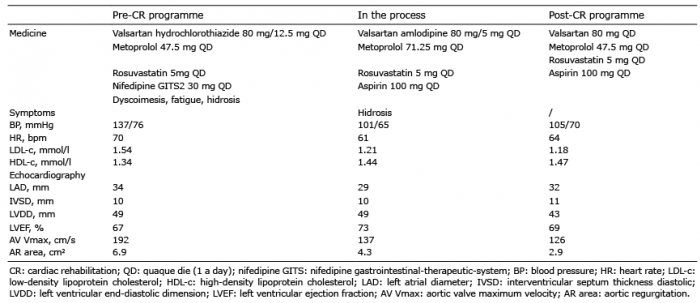
At the end of the CR programme, changes in the patient’s characteristics and medical treatment were observed (Table I). Improvement in CPET and physical assessment results are shown in Table II. Psychology questionnaires, including world health organization quality of life-bref (WHOQOL-BREF) and patient health questionnaire-9 (PHQ-9) were adopted. WHOQOL-BREF scores were 20 in physical domain, 22 in psychological domain, 10 in social domain, and 34 in environmental domain, which changed to 25, 23, 10, and 33 at the end of the CR programme, respectively. PHQ-9 depression test questionnaire scores decreased from 8 to 1, indicating a lower risk of depression.
Table I. Patient’s characteristics and treatment
Table II. Detailed data of cardiopulmonary test (CPET) and physical evaluations data
CoA is one of the most common congenital heart defects, accounting for 5–8% of all congenital heart disease (1). The prevalence of CoA is twice as common in males as in females, and is often diagnosed in children or adults under 40 years of age (2). In mild cases, patients may show no signs and symptoms in childhood. Typically, narrowing of the aorta results in arterial hypertension in the arms and low blood pressure in the lower extremities. The current case was diagnosed with CoA by digital subtraction angiography measurement at 38 years of age with a presentation of hypertension. Surgery and balloon angioplasty has been demonstrated to be effective to treat CoA. It is important that patients with CoA are followed up by a cardiologist after surgery, in order to monitor the progress of high blood pressure and risk of re-coarctation. Studies have consistently demonstrated that, following repair of isolated CoA, patients have a decreased exercise capacity and abnormal blood pressure response to exercise; these changes are not related to surgical results (3–5). Exercise is recommended as a primary prevention, to increase aerobic capacity and reduce the risk of early atherosclerosis, while severe exercise hypertension, restenosis, aortic or cerebral aneurysms are ruled out (4). Regular follow-up, including CPET, and aggressive treatment of hypertension, is strongly recommended after CoA repair, because a high number of patients display exercise hypertension (7). However, there is a lack of research regarding CR for patients who have undergone stenting for CoA. In addition, this case was further complicated by concomitant hypertension and moyamoya disease, in both of which it is necessary to control the amount of exercise, and for which there is a lack of recommendations in the current CR guidelines. Therefore, we monitored the electrocardiogram, heart rate, blood pressure and Borg scale score during each exercise rehabilitation session, and adjusted the target HR with care, based on the patient’s exercise data and physical status. The results in the current case were satisfactory, with improvements in physical, mental, biochemical and echocardiographic parameters following a well-planned CR programme. Therefore, developing good strategies for patients to adhere to the CR plan is essential.
In China, it is reported that only 24% of major hospitals provide a CR programme (6) and thus it is important to raise awareness of the benefits of CR. In addition, a systematic approach to enrolling and recruiting potential candidates following cardiac surgery is necessary, in order to implement CR widely throughout China and provide benefits to the increasing number of cardiovascular patients.
This case study found that CR resulted in significant clinical and functional improvements in an adult patient who had undergone covered CP stent implantation surgery for CoA. This case highlights the benefits of CR exercise on blood pressure control, exercise capacity, clinical outcomes, depression symptoms and quality of life. Despite the fact that these results were acquired in a short time, we expect lasting benefits of CR intervention. In addition, CR programme guidelines should be developed for the management of patients who have undergone stent implantation surgery. Finally, research into larger patient cohorts, with long-term follow-up, participating in post-cardiac operation training programmes are needed in order to raise awareness of the cost-effective benefits of CR in the clinical setting, and to help improve our knowledge of detailed physiological changes in this patient population.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize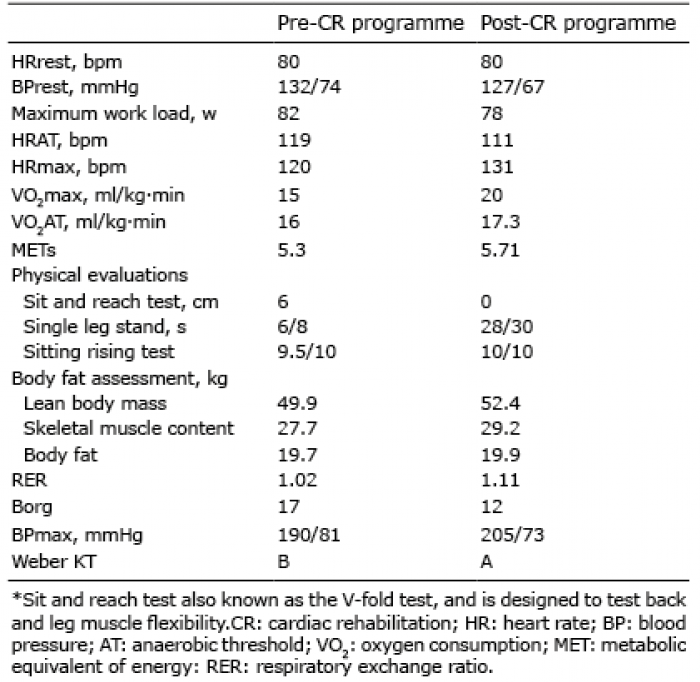 Click to show fullsize
Click to show fullsize