
1Medical Simulation Center, Jichi Medical University, Tochigi, Japan
2Department of Electrical Engineering and Electronics, Aoyama Gakuin University, Kanagawa, Japan
3Rehabilitation Center, Jichi Medical University Hospital, Tochigi, Japan
4Department of Surgery, Jichi Medical University, Tochigi, Japan
Objective: To evaluate the acceptability of using a static wearable chair for patients requiring rehabilitation.
Methods: The acceptability of use of a static wearable chair during rehabilitation was assessed via static balance and subjective evaluation of 7 healthy subjects and 3 patients during standing training. Participants performed 1 standing task in free mode (in which the knee could bend freely) and 1 in support mode (in which the user could sit on the wearable chair with the knee slightly bent) for 3 min. For balance evaluation, the skeletal coordinates were measured. For subjective evaluation, a visual analogue scale questionnaire was administered before and after each task.
Results: Balance assessment revealed that patients had less head sway during support, whereas subjective evaluation showed that the device support created a positive psychological state in terms of stability, comfort, satisfaction, interest in usage, and motivation for rehabilitation. However, patients reported feeling strangeness, fear, or restraint during support.
Conclusion: The static wearable chair improved the static balance of 3 patients and created a more positive psychological state. Use of the device is considered acceptable for use with rehabilitation patients. However, patients might feel strangeness, fear, and restraint during support. Familiarization with the static wearable chair may make it more acceptable among rehabilitation patients.
Key words: exoskeleton device; activities of daily living; ergonomics; equipment safety; user-centred design.
Accepted Oct 1, 2021. Published Nov 8, 2021.
JRM-CC 2021; 4: jrmcc00072
Correspondence address: Yoshitaka Maeda, 3311-1, Yakushiji, Shimotsuke-shi, (Kinen-tou 7th floor), Tochigi, Japan, 329-0498. E-mail: y-maeda@jichi.ac.jp
Doi: 10.2340/20030711-1000071
Wearable chairs allow users to sit in a chair at any time, wherever they are. This study evaluated the acceptability of using a wearable chair for rehabilitation patients, using balance and subjective evaluation. The study included healthy subjects and 3 patients requiring rehabilitation. The participants performed 1 standing task in free mode (in which the knee could bend freely) and 1 in support mode (in which the user could sit on the wearable chair with the knee slightly bent) for 3 min. Patients were likely to have less head sway with the support of the device. Subjective evaluation revealed that the device support created a positive psychological state in patients in terms of stability, comfort, satisfaction, interest in usage, and motivation for rehabilitation. However, patients were likely to feel strangeness, fear, and restraint during support. Accordingly, familiarization with the wearable chair may make it more acceptable among rehabilitation patients.
Wearable chairs are effective for professionals who require prolonged standing, as they allow users to sit at any time, wherever they are. Many exoskeleton-type chairs have been developed (1, 2), including chairs with hydraulic cylinders to support knee-joint flexion while sitting (2). The use of wearable chairs has been suggested to improve quality of work, by maintaining postural stability while effectively reducing musculoskeletal stress in industrial workers (3).
Recently, a wearable chair, the Archelis® (Archelis Inc., Yokohama, Japan)(Please see video of Archelis), was developed and marketed in Japan, with the aim of reducing the discomfort caused by prolonged standing, which affects the lower limbs of surgeons. This device statically supports a near-standing posture (4). This feature facilitates its acceptability among surgeons and nurses (5). Unlike many wearable chairs, Archelis® does not have a power source or control system; therefore, it is expected to be widely applicable in different work settings.
Patients requiring rehabilitation are at high risk of falling during standing training. When a patient is fatigued during rehabilitation, careful assistance from a physical therapist (PT) or occupational therapist (OT) is necessary. The prevention of falls is a physical burden to both the patient and the PT/OT (6). Therefore, this study aimed to investigate the applicability of Archelis® in rehabilitation patients during standing training. If Archelis® is used, it can easily support the patient in a near-standing position when the patient is fatigued. Furthermore, we hypothesized that Archelis® would be highly acceptable among rehabilitation patients because of its lightweight design and its ability to improve physical balance. To test this hypothesis, this study examined the acceptability of using a static wearable chair among patients, using static balance assessment and subjective evaluation.
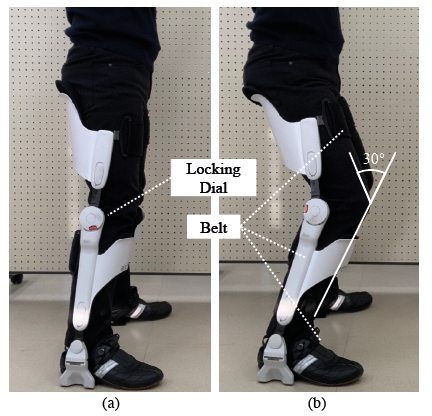
Archelis® is an exoskeleton-type wearable chair, weighing 3.2 kg per side, which is attached to a user’s feet, lower legs, and thighs with a 3-point belt. The chair does not need a power source and has a locking dial on the knee for activating the free and support modes. In free mode, the user can bend the knee freely and walk normally (Fig. 1a), but there is no assistive function for walking. In support mode, a stopper is activated at the knee joint at approximately 30° flexion, allowing the user to sit (Fig. 1b). The weight of the user is distributed and supported by the anterior lower leg and buttocks (4). The user can adjust the size of the chair to suit the length of their lower legs and thighs.
Fig. 1. Archelis®. (a) Free mode, (b) Support mode.
This study investiaged the acceptability of Archelis®, based on the acceptance behaviours of healthy subjects and patients. Three patients admitted at the Jichi Medical University Hospital (Shimotsuke, Japan) were included in the study. PTs and OTs who worked at the hospital were included as the 7 healthy subjects. Participants’ heights were in the range 160–180 cm. Details of the patients’ characteristics are shown in Table I. During the study, participants performed 1 standing task in free mode (control) and 1 in support mode. Each task was performed for 3 min.
For the objective acceptability evaluation, the static balance of subjects during the task was measured using Kinect V1 (Microsoft Corporation, Redmond, WA, USA). Since the main purpose of the Archelis® device is to assist in maintaining a near-standing posture, a static balance not involving movement was evaluated. Kinect V1 was placed 200 cm in front of the participants and 150 cm high to calculate the 3-dimensional skeletal coordinates. The standard deviation values of coordinates of the 4 median plane points of the upper body (head, shoulder centre, spine, and hip centre) during the task were calculated. Sways of the upper body points were evaluated because the lower limbs of the participants were immobilized by Archelis®.
For the subjective acceptability evaluation, participants were assessed using 15 subjective sensory parameters on a 200-mm visual analogue scale (VAS), as shown in Fig. 2. VAS assessment was conducted before and after the task, and the differences were calculated. In addition, the subjects were asked to comment on acceptability.
Based on the above-mentioned evaluations, the differences between the free and support modes were compared using the Wilcoxon rank-sum test for healthy subjects only. The patients were not statistically analysed given the low sample size. The statistical significance level was set at 5%, and MATLAB 2018b (MathWorks Inc., Natick, MA, USA.) was used for statistical analysis.
All participants provided written informed consent for participation in the study. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethical Review Committee of Jichi Medical University Hospital (A18-228). All participants were briefed on the personal information protection process, the use of Archelis®, and the risks involved.
Table I. Patient data
Fig. 2. Mean difference in the visual analogue scale (VAS) scores before and after the task in (a) healthy subjects (n = 7, error bar: standard deviation (SD)) and (b) patients (n = 3, error bar: SD). Black bars: free mode; grey bars: support mode. The score at the left-hand end of the VAS is defined as 0, the score at the right-hand end as 20, and the mean of the differences in values before and after the task is shown.
No statistically significant difference was observed in the standard deviation values of all skeletal coordinates of healthy subjects between the free and support modes. For each skeletal coordinate, the sway was greater in the support mode than in the free mode. The sway in the head was 5.3 mm greater in the support mode than in the free mode. Furthermore, the standard deviation value of the head was largest in both the free and support modes (Table II: right). The skeletal coordinates were different between patients and healthy subjects. Specifically, the head sway was 5.5 mm smaller in the support mode than in the free mode for the patients’ upper body. The standard deviation value in the head movement was the largest for both the free and support modes (Table II: left).
Regarding the subjective evaluation, the responses to 13 items in the free mode showed negative psychological states in healthy subjects (Fig. 2a). In the support mode, responses to all 15 items indicated positive psychological states. Thus, the responses indicated a more positive psychological state in the support mode than in the free mode in healthy subjects. Statistically significant differences were observed in the responses to 4 items: comfort, strangeness, stability, and weight. In the support mode, comfort and stability were especially enhanced.
The patients’ responses to 13 items in the free mode suggested negative psychological states, whereas their responses to only 9 items in the support mode suggested this (Fig. 2b). Responses to 6 items (comfort, concentration, interest, satisfaction, stability, motivation) indicated a positive psychological state in the support mode. In contrast, 3 items (strangeness, fear, and restraint) indicated a more negative psychological states in the support mode than in the free mode.
The healthy subjects reported that they felt comfortable with the support of the device, but it was heavy. They also felt a sense of backward instability and were nervous until they achieved stability. In contrast, the patients reported that their hips and knees were comfortable and the Archelis® seemed to prevent knee buckling and falling. They reported that they could also continue to stand more comfortably if they understood how to apply the centre of gravity.
Table II. Standard deviation of head movement, centre of shoulder, spine, and centre of hip (2-group comparison of healthy subjects in free mode and support mode: Wilcoxon rank-sum test)
Balance assessment revealed that the patients in this study had relatively less head skeletal sway with Archelis® support; likewise, subjective evaluation showed that the Archelis® support created a positive psychological state in terms of stability, comfort, satisfaction, interest in usage, and motivation for rehabilitation. However, the patients experienced strangeness, fear, and restraint during the support.
Healthy subjects had more sway in the support mode than in the free mode for all skeletal coordinates. One subject commented on backward instability in the support mode, suggesting that the effect of Archelis® on the stability of healthy subjects may have been limited. The joint fixation and restriction of muscle activity caused by Archelis® may interfere with the normal balance control provided by the motor system in healthy subjects.
In contrast, the rehabilitation patients showed less head sway in support mode than in free mode. A decrease in head sway may have stabilized vestibular and visual systems, making it easier for the patient to maintain balance while standing (7, 8). In addition, patients commented that Archelis® prevented knee buckling. Patients with myasthenia gravis are at risk of falling because of knee buckling, in which the knee bends unexpectedly (9). Moreover, muscle weakness is central to hereditary spastic paraplegia or myasthenia gravis, which causes poor balance (10, 11). Patients who have experienced knee buckling reportedly have a greater fear of falling (12). In assistive suits and prostheses, preventing knee buckling is considered an important design requirement (9, 13). In the free mode in Archelis®, the stopper at the knee joint is not activated; thus, the head sway was up to 2.66 times greater in the patients than in healthy adults. In contrast, the stopper was activated in the support mode, and this may have effectively prevented knee buckling and facilitated the patients’ ability to control their balance. Therefore, the head sway of patients was reduced to a maximum of 1.32 times that of healthy subjects in this mode.
The subjective evaluation results presented the patients’ responses to 6 items, which indicated a more positive psychological state in the support mode than in the free mode. However, patients experienced strangeness, fear, and restraint with Archelis® in the support mode. Because healthy subjects did not have the same psychological state, this result may be a patient-specific behaviour. Archelis® introduces a slightly bent knee posture, which may seem strange to patients with lower limb muscle weakness, as their experience in maintaining such a posture is limited. In the support mode, weight is supported by only 2 points: the anterior lower leg and the buttocks. Thus, the patients may have felt restraint at these 2 points, especially because they had little experience with this type of load on their lower extremities. Moreover, the patients could not habituate the change in the centre of gravity, and the fear they experienced may not have been alleviated upon completion of the task. A verification study indicated that assistive effect and mental burden reduction effect increased as the usage time with the assistive technology increased (14). Given that assistive devices present a novel technology, their use is associated with mental discomfort among patients (14). During the study, one patient commented that they would be more comfortable standing if they knew how to apply the centre of gravity. In our evaluation, the intensity of the negative psychological state on the physical parameters of the patient and the functional parameters of Archelis® may have reduced the beneficial effects, because the stability and static balance evaluation results were positive in the support mode.
One limitation of this study is that a typical evaluation of a wearable chair is performed by lower limb electromyography (EMG) of a healthy subject, and effectiveness is evaluated based on the decrease in the EMG values (1). Our patients had lower-limb muscle weakness. Therefore, we chose to measure skeletal sway in order to evaluate balance. Because only 3 patients were recruited for this study, statistical comparisons between the free and support modes were not possible. However, the amount of head sway is more accurate when assessing the standing balance than other parameters (8). Although the sample size was small, it is interesting that the Archelis® supported patients’ standing balance. It is also notable that the results of this study are consistent with those of the previously mentioned studies (3, 8).
In conclusion, the static wearable chair, Archelis®, tended to reduce the head sway of patients. Subjective evaluation showed that the device support created a positive psychological state in terms of stability, comfort, satisfaction, interest in usage, and motivation for rehabilitation. In contrast, patients tended to be more susceptible to feelings of strangeness, restraint, and fear while using Archelis®. Although the patients’ responses in support mode indicated a slightly more negative psychological state overall, this may be alleviated by increased familiarity with the device. It is expected that static wearable chairs will be actively introduced into rehabilitation settings in future. It is hoped that this will reduce the risk of patient falls and improve their motivation for rehabilitation, ultimately improving their activities of daily living (ADL).
The authors thank Editage (www.editage.com) for English language editing.
Funding sources. This study was supported by the MIKIYA Science and Technology Foundation.
Conflicts of interest. This study was supported by Archelis Inc., with the free use of Archelis®. This company has had no influence on the data interpretation and the final conclusions.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize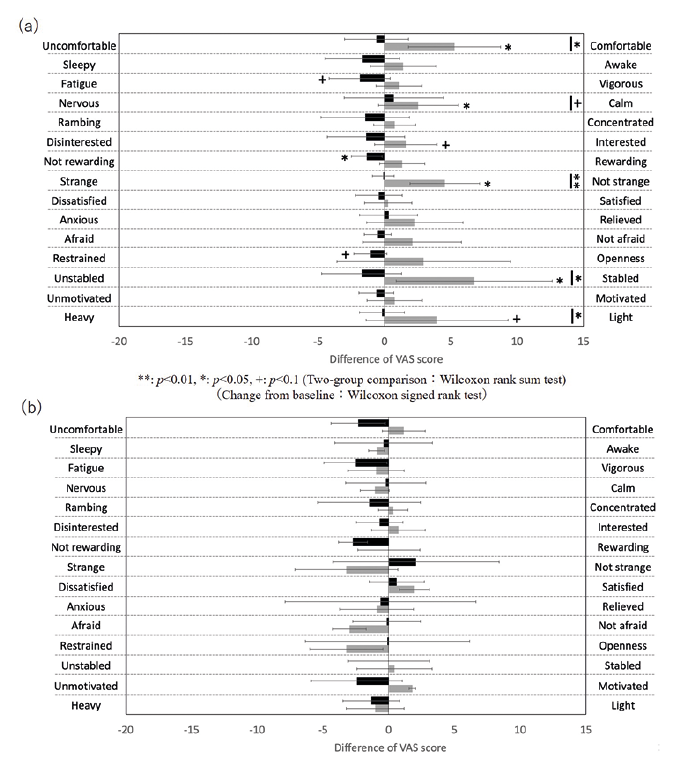 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize