
From the Intermediate Neurological Rehabilitation Unit, Trafford General Hospital, Moorside Road, Manchester, UK
Objective: Neurogenic dysphagia and other neurological manifestations are increasingly described in patients with SARS-CoV-2 (COVID-19). We report here a case of successful treatment of SARS-CoV-2-induced severe neurogenic dysphagia, using pharyngeal electrical stimulation (PES) in addition to speech and language therapy.
Methods: A 62-year-old male patient with COVID-19 pneumonitis, prolonged intubation- and stroke-related severe neurogenic dysphagia, confirmed by instrumental assessment and traditional swallowing therapies, was given novel PES treatment for 5 days.
Results: Within 8 days of completing PES, a clear improvement in dysphagia dysfunction scores (increased Dysphagia Outcome and Severity Scale (DOSS), reduced Penetration-Aspiration Scale (PAS), increased Functional Independent and Assessment Measure (FIM+FAM), and increased Functional Oral Intake Scale (FOIS)) was evident, and further significant improvement occurred in the following 2 weeks. Forty-three days post-stimulation, the patient’s diet had recovered to normal fluids and solids. Using self-administered Swallowing Quality of Life (SWAL-QoL) questionnaires, the patient reported a highly noticeable reduction in dysphagia-associated burden, a greatly decreased risk of choking when eating or drinking, developing pneumonia, and a large increase in self-confidence (total score: 11 pre-PES to 55 directly post-PES).
Conclusion: In a patient with COVID-19 presenting with stroke and intubation-related severe dysphagia, PES was safe and appeared to facilitate faster recovery.
Key words: dysphagia; PES; COVID-19; stroke
Accepted Oct 28, 2021; Published Dec 20, 2021
Jrm-CC 2021; 4: jrmcc00075
Correspondence address: Catherine Blakemore, Salford Royal Foundation Trust, Stott Lane, Salford, M6 8HD, UK. E-mail: catherine.blakemore@srft.nhs.uk
Doi: 10.2340/20030711-1000073
This case report details the rehabilitation and outcome of a 62-year-old man with severe swallowing impairment, caused by COVID-19 pneumonitis, prolonged intubation, and a stroke. Traditional swallowing therapies in addition to a novel approach using pharyngeal electrical stimulation therapy (PES) over 5 days were the chosen treatment approach. Recovery was monitored using objective instrumental assessments (i.e. fibreoptic endoscopic evaluation of swallowing (FEES) and videofluoroscopy) in addition to bedside swallowing assessments. At the start of the rehabilitation, swallowing impairment was severe, with the patient being dependent on tube feeding to meet nutrition, hydration, and medication needs. Within 43 days of commencing treatment the patient had returned to normal fluids and diet and no longer required support via a feeding tube or supplements to manage nutrition and hydration. Quality of life measures indicated significant improvement. PES treatment was safe and appeared to facilitate a faster recovery.
Neurogenic dysphagia is a neurological disorder affecting swallowing function that is extensively observed in patients after stroke, acquired brain injury, neurodegenerative disease, or long-term endotracheal intubation during hospitalization in an intensive care unit (ICU) (1). Aspiration pneumonia, the most severe complication of dysphagia, is described as one of the main causes of re-hospitalization and mortality in patients discharged from ICU (2).
Since the beginning of the SARS-CoV-2 (COVID-19) pandemic, an increasing amount of information characterizing this viral infection has been published. Approximately 20% of patients with COVID-19, especially those older than 65 years in the UK, become critically ill and require hospitalization in the ICU (3). Patients with COVID-19 present with various neurological symptoms at onset, or develop them as complications in the acute phase (4), in particular, the development of neurogenic dysphagia (5). Brugliera et al. reported dysphagia as a frequent complication of orotracheal intubation in COVID-19 cases, as more than 90% of patients admitted to a dedicated rehabilitation unit in Italy showed some degree of swallowing impairment (6). In a case series, Dziewas et al. described the COVID-19-related involvement of the peripheral and central nervous system as a key contributor to swallowing impairment and laryngeal dysfunction in survivors (7). Fibreoptic endoscopic evaluation of swallowing (FEES) and videofluoroscopy (VFS) are the gold-standard instrumental assessment methods recommended for routine clinical dysphagia assessment (8, 9). At the beginning of the COVID-19 pandemic, such aerosol-generating procedures were, however, severely restricted (10); as a consequence, many patients with dysphagia went undiagnosed for a long time or were missed.
PES has been shown to be an effective treatment for neurogenic dysphagia following stroke (11, 12), or to facilitate early weaning of patients with tracheostomy in ICU (13, 14). In addition, PES has shown promising results when used to treat dysphagia resulting from neurological pathologies, such as Guillain-Barré syndrome (15) and multiple sclerosis (16). In the largest real-word study (PHADER) to date, including over 230 patients with neurogenic dysphagia following stroke, traumatic brain injury or from another cause, PES was shown to be safe and associated with reduced dysphagia and penetration/aspiration (17). Moreover, PES has been used to safely and successfully treat dysphagia following invasive mechanical ventilation for COVID-19 (18); consequently, it has recently been added to the updated S1 guideline of the German Society of Neurology (19). We describe here a COVID-19 stroke patient with neurogenic dysphagia acquired due to stroke, prolonged endotracheal intubation, and long-term critical care stay, who was treated effectively with PES.
PES was delivered using Phagenyx®, a medical device CE-marked since 2012 (Phagenesis Ltd, Manchester, UK), designed to treat neurogenic dysphagia by stimulating sensory nerves in the oropharynx through directed electrical pulses (see technical details in Supplementary Material).
Dysphagia severity, assessment of diet and assessment of risk and functional ability were measured using: Dysphagia Outcome and Severity Scale (DOSS) (7-point scale, 7 being the best score: normal diet) (20); Penetration-Aspiration Scale (PAS) (8-point scale, one being the best score: material does not enter the airway) (21); Functional Independent and Assessment Measure (UK FIM+FAM), a scale for measuring disability in brain-injured patients (7-point scale, 7 being the highest score: complete independence, patient manages a normal diet of their choice in a reasonable period of time) (22); Functional Oral Intake Scale (FOIS) (7-point scale, 7 being the best score: total oral diet with no restrictions) (23); and International Dysphagia Diet Standardisation Initiative (IDDSI) (7-point scale, 7 for regular foods and 0 for thin drinks) (24). The assessment of Swallowing Quality of Life (SWAL-QoL) is described extensively in the Supplementary Material.
Demographic details and medical history
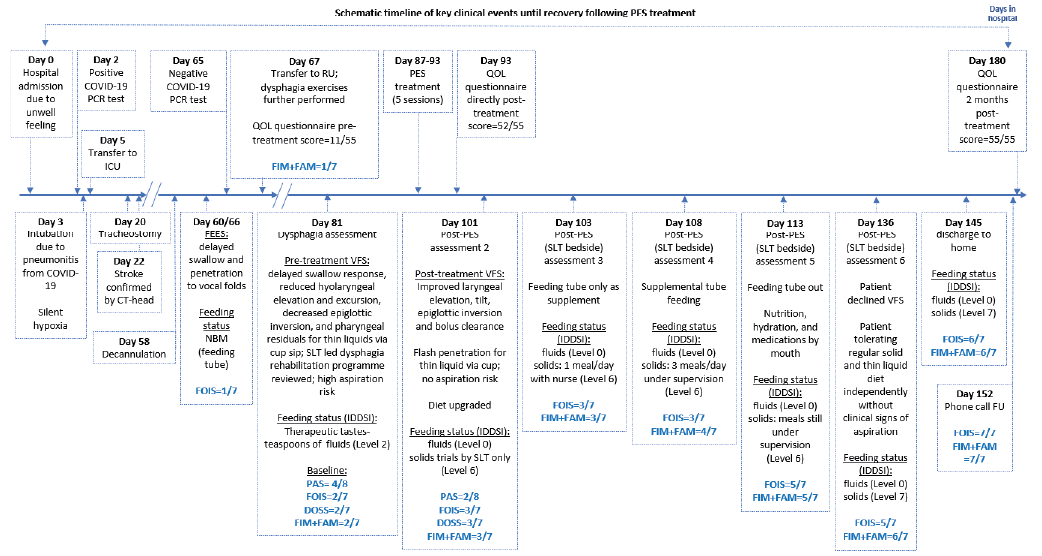
On 21 March 2020 (day 0), a 62-year-old male patient (height 195.5 cm) with a medical history of hypertensive crisis was admitted to a secondary care hospital in Manchester, UK, due to feeling unwell (Fig. 1) and on day 3, returned a positive SARS-CoV-2 PCR test result. The same day, because of silent hypoxia and respiratory insufficiency resulting in a severe pneumonitis from COVID-19, the patient was intubated and started on mechanical ventilation. Two days later (day 5), he was transferred to the ICU. At this stage, the patient had severe disability, was bedridden and incontinent, and required constant nursing care and attention (modified Rankin score 5/6 (25)). A tracheostomy was performed on day 20, followed by a slow respiratory wean. On day 22, a brain computed tomography scan confirmed a stroke (right parietal lobe infarct with haemorrhagic transformation and left side hemiparesis) following COVID-19 infection. Moreover, further evaluation showed an additional subacute infarct/encephalitis, critical illness polyneuropathy and a left internal jugular vein thrombosis. As COVID-19 treatment, the patient received ionotrope support, as well as intravenous steroids and antibiotics. Two days before transfer to a specialist inpatient neuro-rehabilitation unit (RU) on day 65, the first negative SARS-CoV-2 PCR test was returned; still, following the locally agreed protocol, the patient was isolated for a further 7 days on arrival to the unit. Further COVID-19 PCR tests routinely performed at RU on days 128, 135 and 142 returned negative.
Fig. 1. Schematic timeline of key events from hospital admission until recovery after pharyngeal electrical stimulation (PES) treatment. CT: computed tomography; DOSS: dysphagia outcome and severity scale; FEES: fibreoptic endoscopic evaluation of swallowing; FOIS: Functional Oral Intake Scale; FU: follow-up; ICU: intensive care unit; IDDSI: International Dysphagia Diet Standardisation Initiative; NBM: “nil by mouth”; PAS: Penetration Aspiration Scale; PCR: polymerase chain reaction; QOL: quality of life; RU: neuro-rehabilitation unit; SLT: speech and language therapist; VFS: videofluoroscopy.
Baseline dysphagia assessments
On day 58, the patient’s respiratory status stabilized, enabling tracheostomy decannulation. FEES performed on days 60 and 66 revealed a delayed swallow response with laryngeal penetration to the vocal folds following trials of normal fluids (IDDSI level 0) noting a high aspiration risk and a recommendation for “nil by mouth” (NBM). The patient was then transferred on day 67 to RU, where the patient’s feeding status remained NBM, receiving all nutrition and hydration through a nasogastric (NG) feeding tube (FIM+FAM swallowing item score = 1 out of 7, indicating complete dependence). Intensive dysphagia therapy performed with the speech and language therapist (SLT) between day 67 and day 81 included oral motor exercises, chin tuck against resistance (CTAR), tongue press, Masako manoeuvre and effortful swallow (26, 27).
VFS was completed on day 81 to objectively assess the patient’s swallowing function. VFS indicated the patient still had a delayed swallow response, severely reduced hyolaryngeal elevation and excursion, reduced epiglottic inversion and cricopharyngeal muscle dysfunction (reduced opening time) with noted pharyngeal residuals resulting in laryngeal penetration (PAS = 4/8) of thin liquid trials (IDDSI Level 0) both during and after the swallow with high aspiration risk (DOSS = 2/7, indicating a moderately severe dysphagia). Recommendations were to remain NBM with therapeutic trials of IDDSI Level 2 fluids via teaspoon amount with use of compensatory strategies, such as Mendelsohn manoeuvre (28) for safety (FIM+FAM swallowing item score = 2/7 (unable to receive adequate nourishment by oral feeding alone, tube feeding provides primary nutrition, oral feeding is limited, and maximum assistance needed); and FOIS = 2/7, indicating a tube dependency with minimal attempts of food or liquid). PES treatment was recommended in conjunction with the patient’s dysphagia rehabilitation programme.
PES treatment
On day 87, PES was initiated; the patient successfully completed a total of 5 treatment sessions, 10-min per session, between day 87 and day 93. The patient’s optimized stimulation levels across each PES session are shown in Table I. As the patient was anticipating some discomfort during the third consecutive PES treatment, his anxiety seems to have had some impact on his treatment tolerance. No device- or treatment-related adverse events were noted. During stimulation, the patient reported several transitory sensations: a metallic taste and a warm feeling in the throat. As is common for NG feeding tubes, some transient nasal discomfort due to catheter rigidity was also reported, which persisted until its removal.
Table I. Pharyngeal electrical stimulation (PES) current intensities
Treatment outcome
On day 94, immediately following the final PES treatment session, the patient’s swallowing was re-evaluated via SLT clinical bedside assessment with subjectively improved laryngeal elevation (as judged via palpation) and improved stamina (as observed during therapeutic swallowing exercises). Recommendations were to remain NBM with advancement of therapeutic trials from teaspoon amounts to small cup sips of IDDSI Level 2 fluids with use of the Mendelson manoeuvre for safety (FIM+FAM = 2/7; FOIS = 2/7) (Fig. 2 and Fig. 3). Repeat VFS was performed on day 101 (8 days post-PES), revealing notably improved swallow function, as evidenced by improved laryngeal elevation and excursion, improved epiglottic inversion, enhanced crico-pharyngeal opening time with improved clearance of pharyngeal residue. Flash laryngeal penetration with spontaneous clearance (PAS = 2/8 without Mendelsohn manoeuvre: material enters the airway, remains above the vocal folds, and is ejected from the airway; 1/8 with Mendelsohn posture: material does not enter the airway) was observed following thin liquid (IDDSI Level 0) via cup sip with improved DOSS observed (3/7: moderate dysphagia). Diet recommendations were to advance to IDDSI Level 6 soft and bite sized trials and Level 0 thin liquids with use the Mendelsohn manoeuvre for continued safety. An improvement in the feeding status was thus reached: FIM+FAM (3/7: moderate assistance needed to monitor speed and amount of food intake); PAS (2/8) and FOIS (3/7: tube dependency with consistent oral intake of food or liquid). From day 103 onwards, NG feeding was maintained for nutritional support, hydration, and medication, but its use was slowly reduced, as the patient was managing one full meal per day under nurse supervision. On day 108 (15 days post-PES), his feeding status was upgraded to 3 full meals per day of IDDSI Level 6 soft and bite-sized solids and Level 0 thin liquids with use of the Mendelsohn manoeuvre and supplemental NG feeding was further reduced (FIM+FAM = 4/7, indicating primary nourishment by mouth, requirement for diet modifications and only minimal contact to control speed and amount of food intake and minimal assistance needed). FOIS remained stable (3/7) due to the patient’s behavioural and cognitive risks requiring consistent nurse supervision at meals despite improvements in swallowing function warranting a greater scoring improvement. On day 113 (20 days post-PES), the NG feeding tube was removed as the patient was orally managing nutrition, hydration, and medication (FIM+FAM = 5/7, all nourishment by mouth under supervision, requirement for a modified diet and assistance with food choices to ensure that the correct food is provided; FOIS = 5/7, total oral diet with multiple consistencies, but requiring special preparation or compensations). The patient declined VFS planned on day 136 (43 days post-PES) as he reported perception of improved swallow and admitted non-compliance with recommended compensatory swallowing strategies. SLT clinically observed patient safely tolerating normal fluid (IDDSI Level 0) and solids (IDDSI Level 7) under stable FOIS (5/7) and improved FIM+FAM to 6/7 (normal diet by mouth, but excessive time for eating or use assistive devices or strategies to clear food, e.g. multiple swallows, indicating a modified independence). Since day 94, the patient’s weight gain was 5.5 kg (total weight 86.8 kg). Upon discharge to home on day 145 (52 days post-PES), he showed a normal feeding status: IDDSI, Level 0 (fluids) and Level 7 (solids); FIM+FAM = 6/7; FOIS = 6/7 (total oral diet with multiple consistencies without special preparation, but with specific food limitations) (Figs 2 and 3). On 21 August 2020, during a routine follow-up call one week after discharge, the patient reported sitting in his garden, eating steak and chips, and drinking red wine (FIM+FAM = 7/7, indicating a normal diet of his choice in a reasonable period of time and a complete independence; FOIS = 7/7, indicating a total oral diet with no restrictions).
Fig. 2. Functional Oral Intake Scale (FOIS) Scores before and after pharyngeal electrical stimulation (PES). 7-point scale: from worst (1: severe dysphagia, nothing by mouth) to best (7: normal swallowing, total oral diet with no restriction) score.
Fig. 3. Functional Independence Measure and Functional Assessment Measure (FIM+FAM) swallowing item score before and after pharyngeal electrical stimulation (PES). 7-point scale: highest score being 7 (complete independence, patient manages a normal diet of his choice in a reasonable period) to 1 as worst score (unable to take anything by mouth, nutrition is provided by tube feeding).
Quality of life
Quality of life (QoL) was assessed using SWAL-QOL questionnaires pre-PES treatment, directly post-PES treatment and 2 months post-PES treatment; the results of this evaluation are shown in Table SI. In summary, a major QoL improvement was observed following PES therapy.
This case report describes a critically ill patient who spent more than 10 weeks in the ICU because of a COVID-19 infection and its consequence, followed by 2.5 months as an inpatient in a neurological rehabilitation unit. Since the start of the global pandemic, several publications have reported on COVID-19-positive patients having developed subsequent cerebrovascular diseases (29, 30), including patients younger than 50 years old (31). In a retrospective cohort study, approximatively 1.6% of adults with COVID-19 admitted to an emergency department or hospitalized, experienced ischaemic stroke; moreover, the likelihood of stroke was shown to be statistically higher with SARS-CoV-2 infection than with influenza infection (odds ratio (OR) 7.6) (32). It is hypothesized that increased inflammatory parameters (C-reactive protein (CRP) and D-dimer) during SARS-CoV-2 viral infection might play a role in the development of ischaemia. In addition to stroke, the current patient also developed critical illness polyneuropathy (CIP), a mixed sensorimotor neuropathy leading to axonal degeneration and reported previously following SARS-CoV-2 infection. CIP is known to be responsible for longer weaning from mechanical ventilation, generalized weakness, or distal sensory loss, and is associated, among other symptoms, with ICU-acquired dysphagia (33). Encephalitis, as reported in this case, has been also reported to be caused by SARS-CoV-2, as has the higher incidence of silent hypoxia in patients diagnosed with COVID-19 (34). In patients with severe COVID-19 infection, potential neurological aetiologies of dysphagia have been reported (7).
The severe neurogenic swallowing dysfunction in the current patient was undoubtedly related to the stroke as well as to his prolonged ICU stay (17 days endotracheal intubation followed by 38 days of tracheostomy cannulation), with instrumental and objective examinations (FEES and VFS) revealing additional pathophysiological reasons for his impaired deglutition (laryngeal oedema and granuloma). Development of swallowing dysfunction affects 50–60% of endotracheal intubation patients after extubation (post-extubation dysphagia); moreover, approximatively one-third of intubated patients presenting with acute respiratory disorders experience dysphagia symptoms persisting beyond hospital discharge. Intubation duration and length of ICU stay are independently and significantly associated with severity of dysphagia post-extubation. Dysphagia, through the associated reduced pharyngeal and laryngeal sensations, is considered as the most important risk for aspiration pneumonia, which has been associated with a longer stay in hospital, and described as a strong independent predictive factor of mortality at 30 days post-admission (35). Therefore, consistent use of accurate swallowing assessment protocols, including instrumental examinations for detection of silent aspiration, should be routinely performed in order to identify dysphagia during hospitalization (36). In patients with COVID-19, in particular, aspiration pneumonia due to dysphagia might be overlooked, leading to significant comorbidity and greater mortality.
As seen in this case report, on the seventh day following the end of PES therapy and for the first time since admission, both the patient’s swallowing and feeding status improved, as shown not only by bedside dysphagia assessments, but also on VFS. Indeed, only 10 days post-PES treatment, his feeding tube use was considerably reduced, and his diet recommendation was thus upgraded to solid food. Although PES appears to be the main driver, this marked improvement in the patients’ swallowing is probably multifactorial, with spontaneous recovery, therapeutic tastes and SLT therapies also contributing.
Patients with COVID-19 have been reported to have longer stay in ICU and more frequent need for orotracheal intubation compared with patients undergoing intubation for other pathologies (37); however, it has also been reported that patients presenting with SARS-CoV-2 infection, in general, exhibit milder degrees of swallowing impairment (38) and might therefore need fewer swallowing rehabilitation sessions to return to safe oral feeding (5). We might hypothesize that, in the stroke-related dysphagia case reported here, the mechanism of action of PES may have been due to an improved cortical and subcortical control of swallowing (reorganization of neural circuits from the damaged dominant swallowing centres to the contralateral undamaged centres (39)), resulting in improvement in the motor dysfunction of the pharyngeal swallow rather than a reawakening of the peripheral sensory network, which is the postulated mechanism of action in patients following prolonged mechanical ventilation. Indeed, given the low thresholds of PES used to treat this patient, this seems more plausible; however, effects on the peripheral sensory network cannot be ruled out, since measurements of salivary Substance P, a neurotransmitter known to enhance the swallow and cough reflexes and shown to be increased following PES (40), were not performed. Aoyagi et al. suggested that glossopharyngeal and vagal neuropathy might have elicited dysphagia following COVID-19 (41). Prolonged intubation of acute and critical care patients has been shown to alter the mechanoreceptors and chemoreceptors of pharyngeal and laryngeal mucosae, while also causing muscle atrophy and loss of proprioception (42).
Considering the ongoing COVID-19 pandemic, any treatment facilitating a rapid improvement in ICU patients’ condition and their transfer to normal, or rehabilitation departments should be welcome. However, precautionary steps should be observed in order to reduce the risk of SARS-CoV-2 transmission during dysphagia diagnostic assessments and therapeutic procedures, as these are considered to be aerosol-generating procedures (10, 43). The European Society for Swallowing Disorders recently published recommendations on the management of dysphagia in patients with COVID-19 (44); dysphagia intervention strategies using algorithms have also been developed for the therapy of patients with COVID-19 (45). Because of the risk and complications of oropharyngeal dysphagia in patients with COVID-19, some authors have recommended a mandatory post-extubation bedside dysphagia screening performed by SLTs, as well as early therapeutic interventions (46).
This may be especially relevant in patients with COVID-19 with intubation-related dysphagia in whom recovery times are prolonged because of impaired swallowing, which may be quickly and easily resolved through PES therapy. Indeed, as reported by this patient shortly after the last PES session, he experienced a greatly increased self-confidence and improvement in mental health, as well as a significantly reduced psychological burden of dysphagia on his life. The fear of pneumonia expressed by the patient (answered “strongly agreed”) on day 67 upon admission to RU is understandable, given his prolonged intubation following COVID-19-related pneumonitis. Dysphagia is an already well-known reason for anxiety and depression in affected patients (47).
Koestenberger et al. described the benefit of using PES in ICU patients who are still orally intubated; this may be a further option to potentially reduce the dysphagia risk associated with long-term ICU-stay, avoid the placement of, and/or speed up the removal of the tracheal cannula (14). It is likely that PES stimulation may be started sooner and concomitantly with dysphagia exercises. Indeed, PES treatment might have been beneficial to this patient prior to tracheostomy placement; however, even if considered appropriate, the PES device was unfortunately not available in the National Health Service (NHS) acute unit where the patient was initially located, but rather was first administered in the neurorehabilitation setting of a different hospital. In such tracheotomized stroke patients, especially, PES is indicated and recommended to treat dysphagia, and should therefore be made available more widespread throughout the NHS (19).
In conclusion, this case report describes a COVID-19 and acute stroke survivor presenting with severe neurogenic dysphagia due to prolonged intubation and stroke, who was safely and successfully treated with PES, in addition to a standard SLT-led dysphagia rehabilitation programme. In consideration of the immense pressure on the ICU and other hospital services, particularly in times of crisis as in the current global COVID-19 pandemic, rapid identification and effective treatment may allow more rapid safe discharge of neurogenic dysphagia patients out of the ICU and hospital, freeing up vital resources and building patients self-confidence, and therefore self-engagement in their own rehabilitation.
Medical writing assistance was provided by Florence Boulmé, PhD.
The authors have no conflicts of interests to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize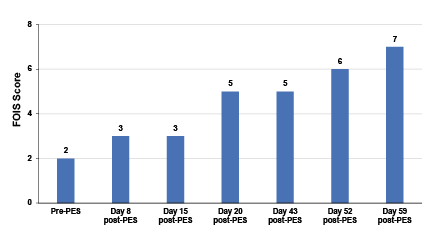 Click to show fullsize
Click to show fullsize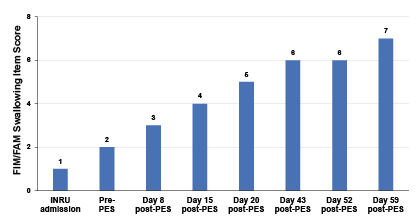 Click to show fullsize
Click to show fullsize