
1Department of Rehabilitation, Kikuno Hospital, Minamikyuusyuu City, Kagoshima, Japan
2Department of Rehabilitation Medicine, The University of Tokyo, Tokyo, Japan
3Center of Medical Education Faculty of Health Sciences, Ryotokuji University, Urayasu City, Chiba, Japan
Objective: To investigate the factors predicting oral feeding ability following acute stroke.
Methods: This retrospective study compared patients admitted to a stroke care unit in 2 groups: an oral intake group and a tube feeding group. The groups were evaluated for 28 items and initial blood investigation tests, and the results compared. Logistic regression analysis was used to identify the clinical variables significantly associated with oral feeding ability.
Results: A total of 255 stroke patients (162 in the oral intake group and 93 in the tube feeding group) were admitted to the stroke care unit. Significant differences were observed between the 2 groups for 20 items. Logistic analysis found that the following variables were significant in the prediction model: age, date of initiation of oral feeding, stroke recurrence/patient deterioration during hospitalization, and date of initiation of occupational therapy.
Conclusion: Factors associated with achieving oral intake among stroke care unit patients were: young age at time of admission; starting oral intake early; no stroke recurrence/patient deterioration during hospitalization; and achieving rehabilitation of daily activities early during the physical function recovery stage.
Key words: acute-stage stroke; oral intake; stroke care unit; predictors.
Accepted Nov 17, 2021; Published Dec 20, 2021
JRM-CC 2021; 4: jrmcc00074
Correspondence address: Toshiyuki Ikegami, Department of Rehabilitation, Kikuno Hospital, 897-0215 3815 Kawanabe-cho, Minamikyuusyuu City, Kagoshima, Japan. E-mail: toshi.ikegami27@gmail.com
Doi: 10.2340/20030711-1000078
A stroke care unit is a hospital ward specializing in acute-stage stroke. Length of stay in the SCU is short. While some SCU patients achieve oral feeding ability by the time of hospital discharge or transfer to another hospital, others do not. In the acute phase of stroke, swallowing status must be confirmed early in order to enable optimum nutritional management. Therefore, this study investigated and clarified factors predicting oral intake ability/incapacity in stroke patients admitted to the SCU. Stroke patients were divided into 2 groups: those who were able to achieve nutrition by oral intake only and those who could not achieve oral intake. Information was obtained from electronic medical records, and several items and data from the initial blood test were compared, and significant differences were found. Of the 255 patients included in the study, 162 had achieved nutrition by oral intake. This study found 4 factors associated with achieving oral intake in SCU patients. It was suggested that if the age of onset of stroke is young, the nutritional status at the time of onset is good, the condition does not worsen during hospitalization, and rehabilitation for daily living can be started early, oral intake may be possible before hospital discharge.
Stroke is the leading cause of neurogenic dysphagia, and often leads to aspiration pneumonia. After a cerebrovascular accident, the incidence of dysphagia has been reported as 22−65% of cases (1, 2), and even up to 37−78% of cases (database review) (3). The chance of developing dysphagia is > 50% within the first 72 h after stroke (4). Dysphagia resolves spontaneously in many survivors of acute stroke, while, in some, it resolves slowly (4, 5). Since half of acute stroke patients recover from neurogenic dysphagia spontaneously within 14 days while the other half stay chronic. The various effects of early intervention in patients with acute stroke have long been reported (6–8). There is emerging evidence that early detection of dysphagia in acute stroke patients not only reduces complications, but also shortens the length of hospital stay and overall healthcare expenditure (7, 8). Evaluation of swallowing status is recommended after hyperacute treatment (7, 8). Moreover, management of swallowing, dehydration, and nutritional status is critical in patients with acute stroke who are admitted to the stroke care unit (SCU) (9).
In the acute situation, medical professionals rely on bedside screening tests to determine swallowing status (10). Numerous screening tools have been developed to facilitate safe nutritional management of patients in the acute phase of recovery after stroke; however, there are few current screening protocols that offer high specificity and sensitivity in predicting aspiration risk, with the Yale Swallow Protocol having a specificity of 64% and sensitivity of 100% (10, 11). In the acute phase of stroke, swallowing status must be confirmed early in order to enable optimum nutritional management. In addition to bedside screening of swallowing, it is necessary to determine which factors enable oral intake. Predictors that affect the resumption of oral intake in stroke patients are older age, lower body mass index (BMI), and higher white blood cell count (WBC)(12). In addition, factors related to the recovery of complete oral intake in patients with post-stroke syndromes, such as signs of liquid aspiration and instrumental assessments, such as videofluoroscopic swallow evaluation, are important in predicting complete oral intake (13). Although previous studies have reported on the prognosis of oral intake related to factors in stroke patients in the subacute period or during the course of recovery, the factors facilitating oral intake after acute stroke remain ambiguous. The aim of this study was to investigate the factors predicting oral feeding ability in stroke patients admitted to the SCU.
This retrospective study included patients discharged from the SCU from 1 September 2015 to 30 September 2018. The study was approved by the medical ethics committee of Chiba Hokusoh Hospital Research Ethics Committee, Chiba, Japan.
Inclusion criteria were: stroke patients admitted to the SCU; and onset of stroke within 48 h prior to admission.
Exclusion criteria were: death; cerebral aneurysm; subarachnoid haemorrhage; brain tumour/meningioma; head trauma; transient cerebral ischaemic attack/suspected cerebrovascular disease; subdural blood; carotid artery stenting/carotid endarterectomy; history of cancer or cancer treatment, history of Trousseau syndrome; convulsions/epilepsy; need for surgery; peripheral nervous system diseases (trigeminal nerve, acoustic nerve, facial nerve); inspection hospitalization; stroke onset while in another hospital; and others (onset of stroke > 48 h prior to admission, strokes which could not be classified). In addition, if the number of items in the initial blood investigation at admission was insufficient, the patients were excluded.
The patients’ clinical data were obtained from electronic medical records, and common variables that may predict dysphagia were selected with reference to previous studies (14). Blood investigation results were obtained at the time of the first hospitalization. A total of 28 variables were recorded, including: age; sex; height; bodyweight; body mass index (BMI); outcome; length of hospitalization; Japan Coma Scale (JCS) (15); type of stroke; site of lesion; need for brain surgery; endovascular treatment; use of recombinant tissue-type plasminogen activator; history of previous stroke, respiratory disease, heart disease, previous kidney disease, and diabetes; need for dialysis; stroke recurrence/patient deterioration during hospitalization; development of aspiration pneumonia during hospitalization; oral feeding starting day; the starting day of swallowing evaluation; videofluorographic examination of swallowing (VF) during hospitalization; and the status of aspiration. The dates of initiation of physical therapy, occupational therapy, and speech language-hearing therapy, as determined by the doctor, were recorded. The severity at first admission was assessed using JCS. Initial swallowing evaluations were performed by doctors or nurses, and repetitive saliva swallowing test and 3-mL water swallowing test were used for screening (16, 17). Oral intake was started if the patient had a profile of 4 or higher, mainly on the 3-mL water swallowing test. Based on the results of the swallowing evaluation, the doctor made a decision and started oral intake. At the start of oral intake, the physician, nurse, and speech-language-hearing therapist evaluated the intake situation, and the physician determined whether oral intake should be continued or interrupted based on the status of cough and respiratory changes. Patients with a 3-ml water swallowing test profile of 3 or less were subject to VF, but there were cases in which VF was not implemented because the stability of the patient’s general condition and their ability to achieve a sitting position were prioritized.
Patients who met the criteria were divided into 2 groups. Patients in these groups were discharged via the SCU and were identified by their nutritional status at discharge. The oral intake group was defined as able to obtain nutrition orally, and the tube feeding group was defined as able to obtain nutrition by tube feeding only or by a combination of tube feeding and oral feeding.
Statistical analyses
Statistical analyses were performed using IBM Statistical Package for Social Sciences ver.25.0 (SPSS, Chicago, IL, USA). A p-value < 0.05 was considered statistically significant. The categorical variables were expressed as frequency and compared using the χ2 test. Continuous variables were expressed as mean and standard deviation (SD) and compared using the Mann–Whitney U test. Continuous variables were analysed by Pearson’s correlation analysis and Spearman’s correlation analysis. Logistic regression analysis was performed to identify the clinical variables that were significantly associated with oral feeding ability in patients with acute stroke. The dependent variable in the logistic regression analysis is the availability of oral feeding ability (yes/no). A regression model using increasing variables by likelihood ratio was used to identify independent predictors of oral feeding ability. Categorical and continuous variables that were significant (p < 0.05) were included in the model as the desired predictors.
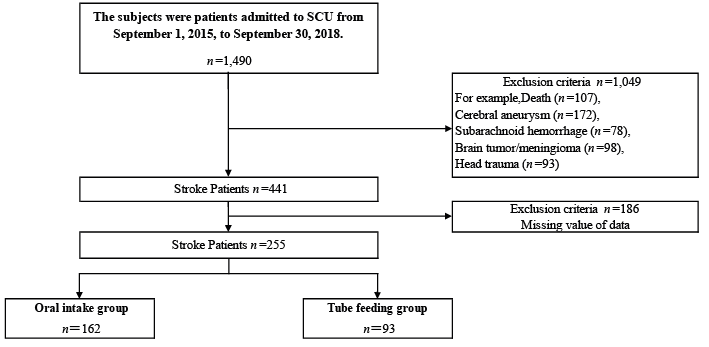
A total of 255 patients fulfilled the study criteria. Of these, 162 (63.5%) were in the oral intake group and 93 (36.5%) in the tube feeding group. A flow chart of the patient selection process is shown in Fig. 1. Exclusion criteria are shown in Table I. Problems with oropharyngeal swallowing before stroke onset were not considered in the exclusion criteria because this data were not available. There were significant differences in 20 variables between the oral intake and tube feeding groups (Table II). The mean number of days required to achieve oral intake in the oral intake group was 4.0 ± 5.3 (median 2 days; range 0−31 days), while that in the tube feeding group was 15.2 ± 12.3 (median 11 days; range 1−54 days). In the tube feeding group, of the 10 patients (10.8%) who underwent VF, 3 (3.2%) developed aspiration. The variables that correlated well with the date of initiation of oral feeding were the number of days of hospitalization (r = 0.52, p <0.01) and the dates of initiation of swallowing evaluation (r = 0.62, p < 0.01), occupational therapy (r = 0.41, p < 0.01), and speech-language-hearing therapy (r = 0.56, p <0.01).
Fig. 1. Patient selection flow diagram. SCU: stroke care unit.
Table I. Exclusion criteria diagnosis (n = 1,049)
Table II. Comparison of 28 variables between oral intake group and tube feeding group
The mean length of hospitalization was 28.5 ± 9.5 days in the oral intake group and 36.2 ± 13.2 days in the tube feeding group. Based on JCS, there were 44 patients (27.2%) with clear awareness in the oral intake group and 33 patients (35.5%) with severe grade 3 in the tube feeding group. In addition, 17 patients (18.3%) in the tube feeding group required brain surgery. In the tube feeding group, stroke recurrence/patient deterioration during hospitalization was noted in 18 patients (19.4%), and aspiration pneumonia during hospitalization developed in 13 patients (14%). Rehabilitation interventions were initiated in the form of physical therapy (1.4 ± 0.7 vs 2.1 ± 1.8 days), occupational therapy (4.9 ± 4.5 vs 6.7 ± 6.2 days), and speech-language-hearing therapy (5.7 ± 4.7 vs 10.5 ± 10.2 days) in the oral intake and tube feeding groups, respectively.
The results of the initial blood investigations at the time of admission are shown in Table III. There were significant differences in 11 parameters between the 2 groups. The albumin (Alb) level tended to be lower in the tube feeding group (3.9 ± 0.3 g/dl) than in the oral intake group (4.1 ± 0.3 g/dl). BMI also tended to be lower in the tube feeding group. The D-dimer level was significantly different between the oral intake (1.0±0.7 μg/ml) and tube feeding (1.8 ± 1.8 μg/ml) groups. The number of patients with atherothrombosis and cardioembolic stroke were 27 (16.7%) and 33 (20.4%) in the oral intake group and 9 (3.5%) and 30 (32.3%) in the tube feeding group, respectively. The parameters that correlated well with age were the Alb levels (r = −0.446, p < 0.01), alanine aminotransferase levels (r = −0.434, p < 0.01), red blood cell (RBC) count (r = −0.465, p < 0.01), and D-dimer levels (r = 0.447, p < 0.01). The parameters that correlated well with bodyweight were RBC count (r = 0.471, p < 0.01), haemoglobin levels (r = 0.477, p < 0.01), and haematocrit levels (r = 0.47, p < 0.01). The parameter that correlated with BMI was RBC count (r = 0.408, p < 0.01). The patients in the tube feeding group were older (74.2 ± 11.6 years) than those in the oral feeding group (66.5 ± 13.2 years), while the bodyweight and BMI of the tube feeding group were less than those of the oral feeding group.
Table III. Comparison of blood test results admission between oral intake group and tube feeding group
Logistic analysis found 4 variables to be significant in the prediction model: age, date of initiation of oral feeding, stroke recurrence/patient deterioration during hospitalization, and date of initiation of occupational therapy (Table IV). As inferred from the logistic regression analysis, stroke recurrence/patient deterioration during hospitalization correlated significantly with oral intake (odds ratio 9.332; 95% CI 1.871−46.537; p = 0.006).
Table IV. Logistic regression analysis
This study investigated the factors correlated with oral intake in patients discharged from the SCU. The main findings were: (i) the median period of initiation of oral feeding was 2 days in the oral intake group, (ii) the hospital stay was shorter in the oral intake group than in the tube feeding group, (iii) the BMI of the tube feeding group was lower than that of the oral intake group, and (iv) stroke recurrence during hospitalization and acute deterioration were strongly associated with nutritional management by oral intake before discharge.
Oral intake should start as early as possible after a stroke. This is similar to studies performed in patients with pneumonia (18). However, a higher incidence of pneumonia has been observed in patients with dysphagia who undergo oral intake than in those who undergo tube feeding (19). Based on these findings, it is crucial to determine the presence of dysphagia early after admission to the SCU. The variables that correlated with the initiation of oral intake were: duration of hospital stay; date of evaluation of swallowing; and the dates of initiation of occupational therapy, and speech-language-hearing therapy. The frequency of performing VF tests and that of examining aspiration status was low. In the current scenario, screening tests are relied upon in the acute phase (10, 20). Development of a unified screening and evaluation protocol for swallowing function in the acute phase is warranted.
The tube feeding group tended to have a more extended hospital stay. Possible causes were the low level of consciousness, the incidence of stroke recurrence/patient deterioration during hospitalization, and concurrent aspiration pneumonia. It is speculated that alterations in these conditions tend to delay interventions (occupational therapy and speech-language-hearing therapy). It has been reported that 44.7% of stroke patients have moderate to severe consciousness disorders (21), which are associated with swallowing functions (22). The dates of initiation of oral feeding and evaluation of swallowing function correlated well with oral feeding. Hence, combination of the evaluation of consciousness level and swallowing function is important in the acute phase of stroke, and consciousness-level arousal is important at the start of oral feeding or swallowing training.
It has been reported that stroke patients in the acute phase are more likely to develop dehydration and tend to have poor nutritional status (9). Previous studies have reported poor clinical and functional outcomes in patients with ischaemic stroke with poor hydration status on admission (23, 24). The data from the current study show that patients who were able to start oral feeding before discharge had better nutritional status than those in the tube feeding group. There was no difference in the hydration status on admission between the 2 groups. However, the D-dimer level was higher in the tube feeding group, and the rate of cardiogenic cerebral embolism was 32.3%. The D-dimer level is reported to be associated with dehydration on admission (25), as well as with the aetiology of stroke, the size of the damaged area, and the severity of acute stroke (26, 27). From the correlation between age, weight and BMI, it is inferred that patients who were older at the onset of stroke had a lower body weight and a lower BMI, and these factors tended to delay oral intake.
Four items were listed in the predictive model that allowed oral intake until discharge. Of these, stroke recurrence/patient deterioration during hospitalization had a significant association. This is because recurrent strokes and acute deterioration of symptoms are more likely to lead to a reduction in the level of consciousness (28, 29). In the case of young patients, it is possible that oral intake can start early after admission to the SCU. Furthermore, if patients undergo no stroke recurrence/deterioration during hospitalization and their physical condition recovers to an extent that rehabilitation of daily activities can be started early, it is suggested to secure nutrition by oral intake before discharge from the SCU in the acute phase.
This study examined the factors enabling nutritional support by oral intake in patients with acute stroke admitted to the SCU. The study has several limitations. First, JCS was used to evaluate the consciousness level at the first visit, and the adoption criteria from the Glasgow Coma Scale (GCS) and National Institutes of Health Stroke Scale (NIHSS) were not clear. It was up to the discretion of the attending physician to decide whether to include the details of GCS or NIHSS. Secondly, the study did not investigate the level of consciousness and swallowing functions on the day of oral feeding. The level of consciousness was considered to be a factor in deciding whether oral intake was possible; however, the details remain unclear. Finally, interpretation of the results was limited by the relatively small sample size and retrospective analysis. A large number of patients were excluded according to the exclusion criteria, and a large proportion of blood investigation results was missing. A future prospective study on the progress from admission to the SCU until discharge, detailing the level of consciousness and swallowing function, and the assessment of blood investigations over time will help to determine the ability to start oral feeding after acute stroke.
This study examined the factors associated with achievement of nutritional status through oral intake in patients admitted to the SCU. Patients who achieved oral intake were young at the time of admission, could start oral intake early, had no stroke recurrence/patient deterioration during hospitalization, and could develop rehabilitation of daily activities early during the physical function recovery stage. Oral feeding may help in ensuring good nutritional status before discharge in these patients.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize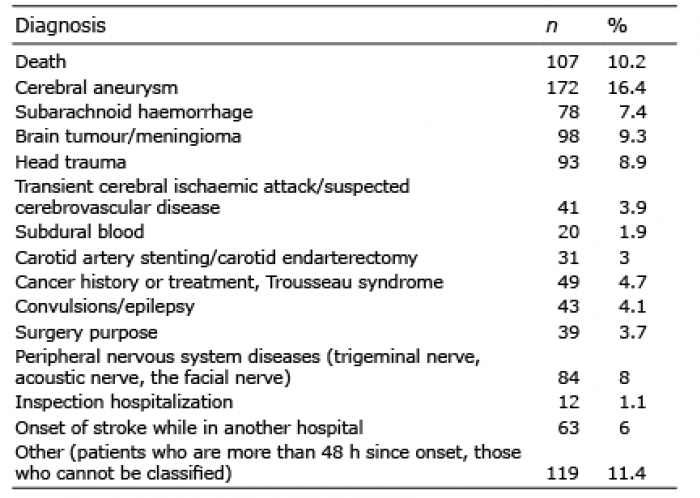 Click to show fullsize
Click to show fullsize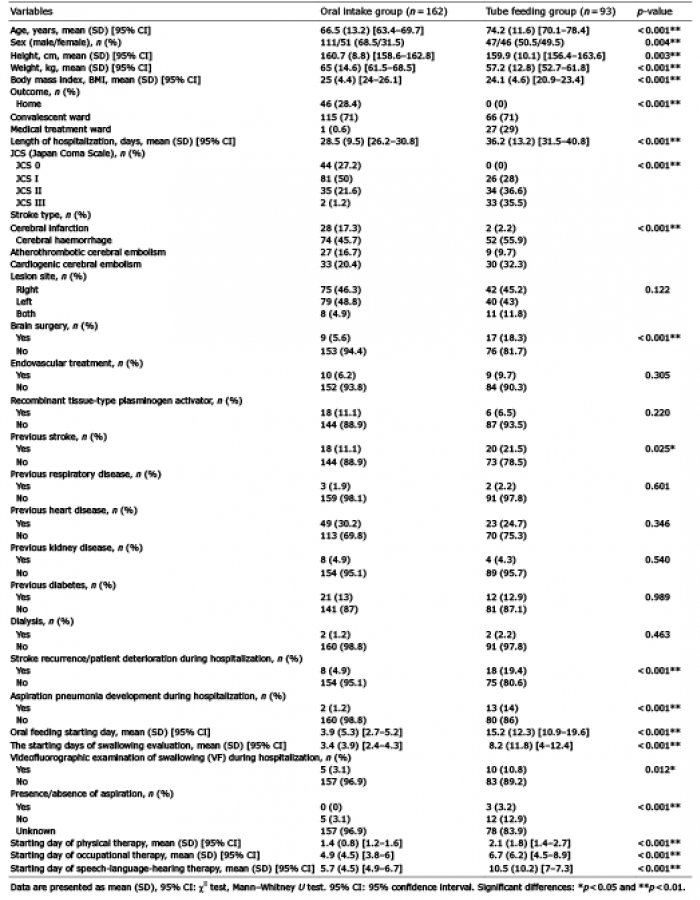 Click to show fullsize
Click to show fullsize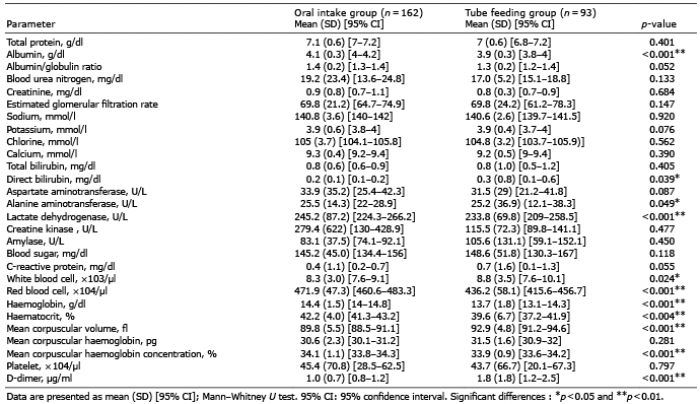 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize