


Miriam Grimaldi1, Guglielmo Pranteda1, Caterina Talerico2 Giulia Pranteda1 and Arianna Di Napoli2
1Dermatology Unit, and 2Department of Histopathology, University of Rome “La Sapienza”, II School of Medicine, S. Andrea Hospital, Via di Grottarossa 1035, Rome, Italy. E-mail: miriamgrimaldi@virgilio.it
Accepted January 27, 2006.
Sir,
Acquired unilateral naevoid telangiectasia (AUNT) is a rare disease predominantly affecting women in a hyper-oestrogenaemic state. In some cases hypersensitivity of oestrogen and progesterone receptors is postulated. Few cases have been reported in males, and these are usually associated with liver dysfunction and hyper-oestrogenism.
We observed a young boy with AUNT. No other disease was associated and no oestrogen and progesterone receptor abnormality was evident in the skin sample.
CASE REPORT
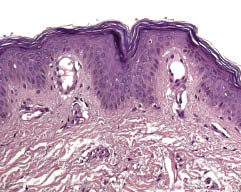
A 10-year-old boy presented erythematous-telangectasic lesions dermatomally distributed on the internal surface of the right thigh, resembling a naevus flammeus (Fig. 1). The lesions first appeared when the boy was 7 years old and progressively increased in size to the entire right thigh surface, causing no other symptomatology. His medical history was unremarkable. Physical examination revealed no other skin alteration and no clinical findings were suggestive for a hyper-oestrogenaemic state. Routine laboratory studies, liver function tests, antibodies to hepatitis A, B and C, levels of oestrogen, progesterone, testosterone and dehydroepiandrosterone were within normal limits. Abdominal ultrasonography was also normal. The histological evaluation of a lesional skin sample revealed ectasia of the superficial and medium dermal vessels, without inflammatory infiltrate (Fig. 2). An immunohistochemistry assay was performed on paraffin sections using a mouse monoclonal antibody anti-oestrogen receptor (clone ER 1D5; 1:50; citrate buffer pH 6.0; Dako Cytomation; Denmark) and a mouse monoclonal antibody anti-progesterone receptor (clone PgR 636; 1:50, citrate buffer pH 6.0; Dako) and developed by a labelled streptoavidin-biotin-kit system (Dako). Results showed that endothelial cells did not express either oestrogen or progesterone receptors.

Fig. 1. Erythematous-telangectasic lesions on the medial aspect of the right thigh.
We did not perform any treatment and the patient is still healthy, after 3 years of follow-up, without any associated pathological condition, and the skin lesions are still present and unchanged.
Fig. 2. Histopathological findings: ectasia of the superficial and medium dermal vessels (haematoxylin-eosin stain, original magnification ×20).
DISCUSSION
The pathogenesis of AUNT is not completely understood. The disease is noted more often in women in a hyper-oestrogenaemic state (pregnancy, puberty, liver disease, hormonal therapy) (1). The oestrogens could stimulate release of endothelium-derived vasodilatory substances (e.g. nitric oxide) or act directly on the vascular smooth muscle (2). Some authors suggested hypersensitivity of the oestrogen and progesterone receptors located on the surface of the endothelial cells with consequent vasodilatation (1). This hypothesis is not always confirmed by the literature data and in some reported cases, the oestrogen and progesterone receptors analysis showed no difference in the levels of receptors between involved and uninvolved skin (3).
AUNT is a rare cutaneous manifestation in males. Most reported cases are associated with chronic liver disease, alcoholic cirrhosis, liver metastases, active hepatitis C and adrenarche with or without a hyper-oestrogenaemic state. Only one report in 1979 by Jucas et al. (4) describes a young healthy boy without evidence of increased oestrogen. Our case is similar and we have performed oestrogen and progesterone receptors analysis, which gave negative results. In 1997 Taskapan et al. (5) reported AUNT in a healthy adult man without hyper-oestrogenism and receptor abnormality and suggested that the hormonal theory cannot be applied in all cases. Our case in a healthy young boy confirms this hypothesis and increases the number of cases of AUNT reported in males without associated disorders.
REFERENCES
1. Wilkin JK, Smith JG Jr, Cullison DA, Peters GE, Rodriquez-Rigau LJ, Feucht CL. Unilateral dermatomal superficial telangiectasia. Nine new cases and a review of unilateral dermatomal superficial telangiectasia. J Am Acad Dermatol 1983; 8: 468–477.
2. White RE. Estrogen and vascular function. Vascul Pharmacol 2002; 38: 73–80.
3. Hynes LR, Shenefelt PD. Unilateral nevoid telangiectasia: occurrence in two patients with hepatitis C. J Am Acad Dermatol 1997; 36: 819–822.
4. Jucas JJ, Rietschel RL, Lewis CW. Unilateral nevoid telangiectasia. Arch Dermatol 1979; 115: 359–360.
5. Taskapan O, Harmanyeri Y, Sener O, Aksu A. Acquired unilateral nevoid telangiectasia syndrome. Acta Derm Venereol 1997; 77: 62–63.
Fig. 1. Erythematous-telangectasic lesions on the medial aspect of the right thigh.

