


It is tacitly assumed that a positive patch test reaction is not affected by adjacent negative tests. However, despite its fundamental importance for the interpretation of test reactions this assumption has not been proven. To test this assumption, special TRUE-test® strips were prepared containing placebo, nickel sulphate and fragrance mix as the only allergens, separated by distances of 1 cm and 7 cm and blinded to the investigators. Patients were synchronously tested with two strips. Out of 493 patients tested in 6 centres, the 93 with positive reactions to nickel sulphate only were evaluated. No relevant difference was found between positive nickel reactions in the two different distances to a negative fragrance patch test. We conclude that a positive patch test reaction is not affected by adjacent negative patch tests, which therefore can be neglected for the interpretation of positive reactions. Key words: patch test methods; contact sensitivity; diagnosis of contact sensitization.
(Accepted February 8, 2006.)
Acta Derm Venereol 2006; 86: 345–347.
Jochen Brasch, Department of Dermatology, University of Schleswig-Holstein, Campus Kiel, Schittenhelmstr. 7, D-24105 Kiel, Germany. E-mail: jbrasch@dermatology.uni-kiel.de
Patch testing is the established method to prove contact sensitization (1). Routinely used standard patch test series usually comprise 20–30 different allergens that are synchronously attached with commercially available test systems (2, 3). This means that a patch test with a distinct allergen is usually surrounded by one or more neighbouring patch tests with other allergens within a short distance. Such adjacent tests are not considered to be relevant because it is generally felt that positive patch test reactions are not significantly modified by neighbouring patch tests, especially not by negative ones. Although this assumption occurs to be obvious, evidence-based medicine requires that a matter of such basic importance for the interpretation of patch test results is verified by valid methods. Therefore, we have addressed this question with a prospective double-blind randomized multicentre study using standardized patch tests strips containing fields with nickel sulphate and fragrance mix separated by exactly defined distances.
MATERIALS AND METHODS
Six centres of the German Contact Dermatitis Research Group contributed to this double-blind study with approval from the local ethics committees. Patch test patients older than 17 years were enrolled after giving informed consent. Exclusion criteria were any kind of immunosuppressive medication, treatment of the back with ultraviolet-light or corticosteroids within 4 weeks prior to testing, inflammatory dermatoses of the back, any major general disease, and pregnancy.
Special TRUE-test® strips were prepared and supplied for this study by MEKOS Laboratories AS (Hillerød, Denmark). In principle their construction was identical to that of commercially available TRUE-test®-strips (4). Corresponding to the latter, the test fields were arranged in one vertical line, each test field covering a square area of 0.81 cm2, and with 1 cm distance between neighbouring fields. However, each study strip comprised six test fields only (fields 1–6, consecutively numbered from the top of the strip downwards), and only three of them were provided with customary TRUE-test® allergens – either nickel sulphate (0.20 mg/cm2) or fragrance mix (0.43 mg/cm2). Each patient was simultaneously tested with two strips attached to the left and right side of the back. One of the two strips was provided with nickel sulphate in field 1 and 6 and additionally with fragrance mix in either field 2 or 5; the other one was provided with fragrance mix in field 1 and 6 and additionally with nickel sulphate in either field 2 or 5. The study strips were attached vertically, with field 1 on top. No other patch tests were allowed within a distance of 10 cm of the study strips. Patients and investigators were blinded as to which of the two strips attached contained which allergens and which fields of the strips were test fields or placebo fields. The described arrangement of test fields ensured that each patient was tested with one nickel field in a distance of 7 cm to a fragrance field, with one fragrance field in a distance of 7 cm to a nickel field, and with two nickel and fragrance fields separated by a distance of 1 cm (one such pair of neighbouring patches on each strip).
Patch testing was done according to the guidelines of the German Contact Dermatitis Research Group (5) and to common rules (6). The study strips were attached for 2 days and reactions were read on day 2 and day 3; negative (–): no visible reaction; questionable (?): erythema, no infiltration; follicular (f): only discrete follicular papules in the test area; weak (+): erythema, infiltration, slight papules possible; moderate (++): erythema, infiltration, papules, vesicles; strong (+++): erythema, infiltration, confluent vesicles. The reading on day 3 was used for all evaluations.
For further evaluations, only those patients who had at least one positive reaction in any of the three nickel fields and who had no positive reaction to fragrance mix were included. To compare the strengths of reactions, numerical values were allocated as follows to distinct reactions: 0 to negative reactions; 0.5 to questionable, irritant and follicular reactions; 1 to + reactions; 2 to ++ reactions; and 3 to +++ reactions. The sign test was used for statistical evaluations, p<0.05 was considered to indicate a statistically significant difference.
RESULTS
A total of 493 patients (60.5% women and 39.5% men) were tested from April 2002 to March 2004. The mean age of the test patients was 50 years; 66 patients (13.4%) had a history of atopic dermatitis. One hundred patients had at least 1 positive reaction to nickel sulphate, 12 patients had at least 1 positive reaction to fragrance mix, 7 patients had at least 1 positive reaction to both allergens and 93 patients had at least 1 positive test reaction to nickel sulphate but no positive reaction to fragrance mix.
Based on 93 patients with a positive nickel patch test, and assuming that a neighbouring fragrance test would significantly shift the result in at least one-third of these patients, the power would be 0.86 to detect such a difference at the 5% significance level by non-parametric testing.
Each patient had been tested with one nickel test field in a distance of 7 cm to a fragrance test field and with two nickel test fields in a distance of 1 cm to a fragrance test field (one on each side of the back). Taking all patients together, the total number of weak positive reactions, moderate positive reactions, and strong positive reactions to nickel was not dependent on the distance to the fragrance mix test field (Table I). Furthermore, the intra-individual differences (∆ strength) between the reaction strength of the nickel reaction with 7 cm distance to a fragrance test field and the mean strength of the two nickel reactions with 1 cm distance to a fragrance mix test field in the same patient showed no significant trend to be either positive or negative (Fig. 1).
Table I. Mean distribution of positive patch test reactions to nickel sulphate, according to reaction strength and distance to a negative fragrance mix patch test. Data are based on 93 patients with at least one positive nickel patch test and no positive reaction to fragrance mix (expressed as % of 493 patients)
| Nickel reaction | Distance 7 cm | Distance 1 cm (left side of back) | Distance 1 cm (right side of back) |
| + | 31 (6.3%) | 30 (6.1%) | 29 (5.9%) |
| ++ | 40 (8.1%) | 42 (8.5%) | 38 (7.7%) |
| +++ | 12 (2.4%) | 12 (2.4%) | 11 (2.2%) |
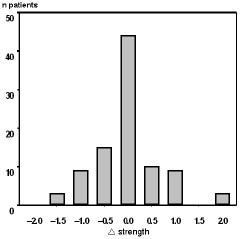
Fig. 1. Distribution of patients according to differences between the strength of their positive reaction to nickel sulphate situated in a distance of 7 cm to a negative fragrance mix patch test (strength Ni7cm) and the mean reaction strength of their nickel reactions situated in a distance of 1 cm to a negative fragrance patch test on the left side and the right side of the back (mean strength Ni1cm): ∆ strength = (strength Ni7cm) – (mean strength Ni1cm). Data are based on 93 patients with at least 1 positive nickel patch test and no positive reaction to fragrance mix.
DISCUSSION
Nickel sulphate and fragrance mix were chosen for this study because they are the two contact allergens of standard patch test series that most frequently yield positive reactions (7, 8). Furthermore, there is no cross-reactivity between both substances (3, 9) and patch tests with both substances have a good reaction index, positivity ratio and reproducibility (10–14). The TRUE-test® system was chosen because it guarantees an optimal standardization of test material and highly reproducible reactions (15, 16). The special TRUE-test® strips prepared for this study ensured that the defined distances between test fields were exactly observed and that reading was blinded.
There was no relevant difference between positive reactions obtained with nickel sulphate patches placed in a distance of 7 cm to a negative fragrance mix patch test and positive reactions to a nickel sulphate patch test placed in a distance of only 1 cm to a negative fragrance mix patch test. This result was found when the reactions of all patients were pooled for evaluation (Table I), and it was confirmed when the intra-individual differences of the strengths of nickel reactions with different distances to negative fragrance patch tests were analysed (Fig. 1). Our results therefore clearly indicate that a negative patch test with fragrance mix has no major influence on an adjacent positive patch test with nickel sulphate.
This confirmation that a negative patch test is not a relevant source of “danger signals” (cytokines etc.) interfering with a neighbouring positive patch test reaction is an essential precondition for the common practice to simultaneously attach multiple patch tests separated by only short distances. Our study was performed with the two most important contact allergens. We cannot exclude, of course, that other allergens may give results divergent from what we found for nickel and fragrance mix; however, we do not see a convincing reason for such a different outcome.
We would also have liked to analyse the influence that a positive reaction to fragrance mix might have on simultaneous positive nickel patch tests located in a short and long distance to it. However, with only 7 patients responding with positive reactions to nickel sulphate and to fragrance mix as well, such an analysis was not possible with our data. Therefore, we cannot clarify whether a positive patch test reaction can modify a neighbouring positive patch test reaction to another allergen. Previous studies indicated that this might be the case under certain circumstances (17, 18), although strong reactions to high concentrations of nickel did not enhance the response to an adjacent lower nickel concentration (19). It remains a challenge for future studies to find a definite answer to this question.
REFERENCES
1. Belsito DV. Patch testing: after 100 years, still the gold standard in diagnosing cutaneous delayed-type hypersensitivity. Arb Paul Ehrlich Inst Bundesamt Sera Impfstoffe Frankf a.M. 1997; 91: 195–202.
2. Marks JG, Belsito DV, DeLeo VA, Fowler JF, Fransway AF, Maibach HI, et al. North American Contact Dermatitis Group patch-test results, 1996–1998. Arch Dermatol 2000; 136: 272–273.
3. Brasch J, Uter W, Geier J, Schnuch A. Associated positive patch test reactions to standard contact allergens. Am J Contact Dermatitis 2001; 12: 197–202.
4. Fischer T, Kreilgaard B, Maibach HI. The true value of the TRUE test for allergic contact dermatitis. Curr Allergy Asthma Rep 2001; 1: 316–322.
5. Schnuch A, Aberer W, Agathos M, Brasch J, Frosch PJ, Fuchs T, et al. Leitlinien der Deutschen Dermatologischen Gesellschaft (DDG) zur Durchführung des Epikutantests mit Kontaktallergenen. Hautarzt 2001; 52: 864–866.
6. Wahlberg JE. Patch Testing. In: Rycroft R J G, Menné T, Frosch P J, Benezra C, eds. Contact dermatitis. Berlin: Springer-Verlag 1992: p. 239–268.
7. Schnuch A, Geier J, Uter W, Frosch PJ, Lehmacher W, Aberer W, et al. National rates and regional differences in sensitization to allergens of the standard series. Population-adjusted frequencies of sensitization (PAFS) in 40,000 patients from a multicenter study (IVDK). Contact Dermatitis 1997; 37: 200–209.
8. Schnuch A, Lessmann H, Geier J, Frosch PJ, Uter W. Contact allergy to fragrances: frequencies of sensitization from 1996 to 2002. Results of the IVDK. Contact Dermatitis 2004; 50: 65–76.
9. Brasch J, Schnuch A, Uter W. Strong allergic patch test reactions may indicate a general disposition for contact allergy. Allergy 2006; 61: 364–369.
10. Brasch J, Geier J, Henseler T. Evaluation of patch test results by use of the reaction index. An analysis of data recorded by the Information Network of Departments of Dermatology (IVDK). Contact Dermatitis 1995; 33: 375–380.
11. Geier J, Uter W, Lessmann H, Schnuch A. The positivity ratio – another parameter to assess the diagnostic quality of a patch test preparation. Contact Dermatitis 2003; 48: 280–282.
12. Belsito DV, Storrs FJ, Taylor JS, Marks JG, Adams RM, Rietschel RL, et al. Reproducibility of patch tests: a United States multicenter study. Am J Contact Dermatitis 1992; 3: 193–200.
13. Brasch J, Henseler T, Aberer W, Bäurle G, Frosch PJ, Fuchs T, et al. Reproducibility of patch tests. J Am Acad Dermatol 1994; 31: 584–591.
14. Bourke JF, Batta K, Prais L, Abdullah A, Foulds IS. The reproducibility of patch tests. Br J Dermatol 1999; 140: 102–105.
15. Lachapelle JM, Bruynzeel DP, Ducombs G, Hannuksela M, Ring J, White IR, et al. European multicenter study of the TRUE TestTM. Contact Dermatitis 1988; 19: 91–97.
16. Brasch J, Henseler T, Aberer W, Fuchs T, Hoeck U,
Kreilgård B. Patch testing of nickel sulfate and potassium dichromate with a standardized ready-to-use test system
gives highly reproducible results. A double blind multi-center study. Acta Derm Venereol 2001; 81: 122–124.
17. Moss C, Friedmann PS, Shuster S, Simpson JM. Susceptibility and amplification of sensitivity in contact dermatitis. Clin Exp Immunol 1985; 61: 232–241.
18. Brasch J, Kreilgård B, Henseler T, Aberer W, Fuchs T, Pflüger R, et al. Positive nickel patch tests do not intensify positive reactions to adjacent patch tests with dichromate. Contact Dermatitis 2000; 43: 144–149.
19. Andersen KE, Lidén C, Hansen J, Vølund Å. Dose-response testing with nickel sulphate using the TRUE test® in nickel-sensitive individuals. Multiple nickel sulphate patch-test reactions do not cause an “angry back”. Br J Dermatol 1993; 129: 50–56.
A Multicenter-study by the German Contact Dermatitis Research Group
Jochen Brasch1, Michael Weichenthal1, Christiane Szliska2, Harald Löffler3, Patrick Koch4, Jürgen Grabbe5, Vera Mahler6, Bo Kreilgård7 and Ulla Hoeck7
Departments of Dermatology, 1University of Schleswig-Holstein, Campus Kiel, Kiel, 2Krankenhaus Bethesda, Freudenberg, 3University of Marburg, Marburg, 4University of Saarland, Homburg/Saar, 5University of Schleswig-Holstein, Campus Lübeck, Lübeck, 6University of Erlangen, Erlangen, Germany, and
7MEKOS Laboratories AS, Hillerød, Denmark

