


Jon Anders Halvorsen1, Trine Brevig2, Torkild Aas3, Anne Grete Skar4, Ellen Margrethe Slevolden1 and Harald Moi5
Departments of 1Dermatology, 2Pathology, 3Paediatrics, and 4Microbiology, Ullevaal University Hospital, Oslo, Norway, and 5Olafia Klinikken, Oslo, Norway
Genital ulceration is an uncommon manifestation of primary Epstein-Barr virus (EBV) infection. We present here two cases of genital ulcers probably caused by EBV. The first case is a 12-year-old girl with a genital ulcer appearing before specific EBV serology could identify a primary infection. However, serology was positive 13 days after the ulcer appeared. Polymerase chain reaction for EBV was positive in the biopsy from the ulcer as well. The second case is an 18-year-old female in whom the specific EBV serology was positive 8 days after appearance of the ulcer. The ulcers in both cases healed after 21 days. We reviewed the literature and a total of 26 cases of EBV-associated genital ulcers in females are now published. Median age of the 26 cases is 14.5 years of whom only 6 reports previous sexual contact. Mean healing time for the ulcers is 18 days. Our two cases correspond well with clinical reports of 24 EBV-associated genital ulcers in the literature. Key words: Epstein-Barr virus; genital ulcer; HHV-4; infectious mononucleosis; Lipschütz`s ulcer; ulcus vulvae acutum.
(Accepted April 12, 2006.)
Acta Derm Venereol 2006; 86: 439–442.
Jon Anders Halvorsen, Department of Dermatology, Ullevaal University Hospital, N-0407 Oslo, Norway. E-mail: jander-h@online.no
Symptomatic Epstein-Barr virus (EBV) infection is most often found in teenagers, and is characterized by tonsillitis, fever and lymphadenopathy. Hepatosplenomegaly goes along with elevated liver enzymes. Non-specific symptoms, such as headache, malaise, anorexia, myalgias and chills, are common. Nearly all acute-phase sera from patients suffering from primary EBV infection contain antibodies to EBV capsid antigen (VCA-IgM and VCA-IgG). The VCA-IgM titre peaks around the second week of illness. The VCA-IgG peaks a little later and then VCA-IgG antibodies gradually decline to levels seen in blood donors, persist for life and appear to be associated with permanent immunity. Antibodies to EBV nuclear antigen (EBNA-IgG) first begin to appear in a minority of patients in the third or fourth week following onset of an EBV infection. However, by 6 months, all convalescent patients carry this antibody, which then persists for life (1).
We herein present 2 females with genital ulcers as an abnormal presentation of EBV infection.
CASE REPORTS
Case 1. A 12-year-old girl felt ill with fever, dysuria and intense vulval pain for one day before she developed a genital ulcer (day 1). Her primary physician gave her one dose of amoxicillin. During the first visit to the hospital (day 3), she had one well-defined exudative genital ulcer sized 2×2 cm located on her left labium minus and perineum, in addition to some smaller erosions (Fig. 1). She denied any sexual genital contact previously in life. She was admitted to the hospital (day 4) because of intense vulval pain. Day 10 she developed a morbilliform rash. At this point she had tonsillitis, fever and enlarged glands in the groins. Mononucleosis was confirmed on day 13 by a positive heterophile antibody test and a positive VCA-IgM test. Duration of the ulcers was 3 weeks.
Fig. 1. Case 1: a deep pinched-out genital ulcer with adherent fibrin on day 3.

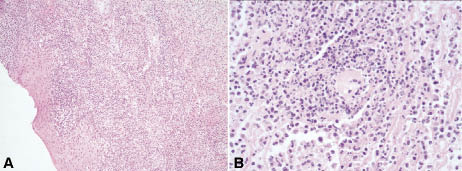
The serological findings are summarized in Table I, in addition the following tests were negative: bacterial culture from the ulcer (day 5), herpes simplex virus (HSV) culture (day 3, day 5) and culture of streptococci from the throat (day 13). Biopsy (Figs. 2A and B) from the ulcer was performed on day 5. This specimen was later found PCR positive for EBV.
Table I. Serological findings in two cases of probable Epstein-Barr-virus-associated genital ulcers
| Genital ulcer(s) appeared | VCA-IgM neg VCA-IgG neg ENBA-IgG neg | VCA-IgM pos VCA-IgG neg ENBA-IgG neg | VCA-IgM neg VCA-IgG pos EBNA-IgG pos | Negative for HSV, CMV, TP, Hep B and HIV | |
| Case 1 | Day 1 | Day 3 | Day 13 | 6 months | 6 months |
| Case 2 | Day 1 | ND | Day 9 | 6 months | 6 months |
VCA-IgM, IgM antibodies to EBV capsid antigen; VCA-IgG, IgG antibodies to EBV capsid antigen; EBNA-IgG, IgG antibodies to Epstein-Barr nuclear antigen; HSV, IgG to herpes simplex virus; CMV, cytomegalovirus antibodies, TP, Treponema pallidum antibodies; HIV, human immunodeficiency virus; Hep B, hepatitis B serology; ND, not done.
Table II. Twenty-six cases of Epstein-Barr-virus-associated genital ulcers in females
| Patient age (years) | Number of big ulcers | Sexual activity | Urinary symptoms | Genital pain | Prodromal symptoms (days) | Healing time (days) | Publication (ref) |
| 14 | ≥ 3 | OG | Yes | Yes | 7 | 14 | Brown 1977 (2) |
| 23 | ≥ 3 | OG, GG | Yes | Yes | 24 | 32 | Portnoy 1984 (4) |
| 13 | 1 | None | Yes | Yes | 8 | 19 | Groulier 1986 (15) |
| 13 | ≥ 3 | None | Yes | Yes | 0 | NR | McKenna 1994 (16) |
| 10 | 1 | None | Yes | Yes | 4 | 9 | Wilson 1993 (17) |
| 14 | 1 | None | NR | Yes | 1 | 20 | Navarro 1996 (18) |
| 13 | 1 | None | NR | Yes | 0 | 30 | Lampert 1996 (19) |
| 18 | NR | None | NR | Yes | NR | 15 | Gisserot 1997 (20) |
| 14 | 2 | None | NR | Yes | 0 | 14 | Taylor 1998 (5) |
| 14 | 2 | DG | NR | Yes | 0 | 10 | Taylor 1998 (5) |
| 13 | 1 | None | Yes | Yes | 1 | 25 | Hudson 1998) (21) |
| 51 | 2 | NR | NR | Yes | 2 | 28 | Logeart 1998 (22) |
| 16 | ≥ 3 | None | NR | NR | 0 | NR | Sisson 1998 (12) |
| 15 | 2 | None | Yes | Yes | NR | NR | Pelletier 2002 (6) |
| 17 | NR | None | Yes | Yes | 3 | NR | Pelletier 2002 (6) |
| 14 | 1 | None | NR | Yes | 5 | 14 | Svedman 2002 (23) |
| 19 | ≥ 3 | Yes | Yes | Yes | 0 | NR | Cheng 2004 (11) |
| 16 | 2 | None | Yes | Yes | 21 | NR | Cheng 2004 (11) |
| 10 | ≥ 3 | NR | Yes | Yes | NR | NR | Cheng 2004 (11) |
| 2 | 1 | NR/No | NR | Yes | 4 | 5 | Tenorio 2004 (24) |
| 18 | ≥ 3 | DG | NR | Yes | 7 | 18 | Lorenzo 2005 (13) |
| 18 | ≥ 3 | None | NR | Yes | 0 | 22 | Lorenzo 2005 (13) |
| 30 | 2 | NR | NR | No | 5 | 14 | Nicolas 2005 (14) |
| 20 | 2 | NR | NR | Yes | 6 | 10 | Nicolas 2005 (14) |
| 12 | 1 | None | Yes | Yes | 1 | 21 | Present case 1 |
| 18 | 2 | GG | No | Yes | 7 | 21 | Present case 2 |
Healing time, approximate healing time; OG, orogenital; DG, digital genital; GG, genital-genital; NR, not reported.
Fig. 2. Histology from the genital ulcer in case 1. (A) Extensive mixed inflammatory cell infiltrate in dermis (haematoxylin and eosin (H&E); original magnification ×10). (B) Inflammatory vascular reaction/leukocytoclastic vasculitis without extravasation of RBC (H&E ×40).
The course of the disease, laboratory results and the typical mononucleosis-like drug eruption appearing about 10 days after the intake of amoxillin indicates that the genital ulcer is probably caused by primary EBV infection.
Case 2. An 18-year-old female developed a genital ulcer (day 1) after having felt ill for one week, and after having had fever for 4 days. She had unprotected first-time coitus 8 weeks previously with an unknown male partner. She received benzyl penicillin for tonsillitis (day 7) and was referred from a local department of gynaecology. By day 9, two ulcers approximately one cm in diameter had developed in the posterior commisure. Mononucleosis was confirmed by a positive VCA-IgM test and the ulcers persisted for a period of 3 weeks.
The serological findings are summarized in Table I, and the following tests were negative: dark field microscopy from the ulcer (day 9), a urethral and cervical smear showed no inflammation (day 9), bacterial culture from the ulcer (day 2 normal flora), HSV culture from the ulcer (day 2, day 9), culture for Hemophilus ducreyi (day 9), DNA amplification test for chlamydia (day 9), gonococcal growth (day 9) and hepatitis C serology (day 1 and at 6 months).
No other aetiology was found, and we conclude that the ulcer is probably caused by a primary EBV infection.
DISCUSSION
In 1977 Brown & Stenchever (2) published a case of a genital ulceration associated with EBV infection. The patient was a 14-year-old girl with fever, headache, sore throat, lymphadenopathy and genital ulceration. However, the Austrian dermatologist Lipschütz (3) had previously identified an acute disease with fever, genital ulceration and lympadenomegaly in young women in 1913. This syndrome has subsequently been called Lipschütz’s ulcer or ulcus vulvae acutum. It now seems clear that at least some cases of Lipschütz’s ulcer are caused by primary EBV infection.
Medline and EMBASE search identified 24 cases of genital ulcerations associated with EBV infection in females. In Table II clinical data of 26 cases are summarized to the best of our understanding. The diagnoses have been based on heterophile antibody tests and/or specific EBV antibodies. In our first case and in 4 others, the virus has also been identified from the ulcer by PCR or culture (4–6).
All cases from the literature were females, except for a 26-year-old man; his diagnosis was based on heterophile antibody test and not on specific serology for EBV (7). Other authors have questioned whether EBV was the cause of this ulcer (8). This case is not included in Table II, and we assume that EBV-associated ulcers are predominantly found in females.
The median age of the 26 patients is 14.5 years. This correlates well with the age group that contracts infectious mononucleosis in higher socioeconomic groups in industrialized nations where more than 50% of teenagers escape the infection during childhood (9). We have also included a 51-year-old patient and a 2-year-old, in our review, as this illustrates that EBV-associated ulcers may also be found in other age groups.
Only 6 of the 26 patients reported sexual activity prior to appearance of genital ulcers. Some case reports clearly state that sexual activity has never taken place, while other state that the patient has not had any recent sexual activity. Normally, the virus seems to be transmitted by saliva, hence the name “kissing-disease”. Genital ulcers are therefore probably a manifestation of a systemic viraemia. However, both female and male genital tract may harbour EBV (10), so one cannot rule out that the virus may be transmitted sexually.
It seems that most patients develop rather large ulcers; usually with a diameter >1 cm. Eight patients had one single large ulcer. In addition, multiple smaller ulcers or erosions were also common. Three or more ulcers were reported in 8 cases. The EBV-associated ulcers are often quite deep and necrotic with purple-red irregular edges. It is important to notice that these ulcers are frequently very painful (24 patients). Not surprisingly the ulcers may cause urinary symptoms (12 patients) such as dysuria and urine retention, and sometimes the patients have received treatment for a urinary tract infection. The mean healing time of these 26 patients was 18 days, which is about the same healing time as primary herpes virus infection.
In these 26 cases, the genital ulcer was the presenting or the dominating symptom of EBV infection. However, in many cases unspecific prodromal symptoms, such as fatigue, headache and fever preceded (mean 5 days) the ulcerations. In the course of the disease, the majority of patients developed symptoms characteristic of mononucleosis, e.g. tonsillitis, lymphadenopathy and elevated liver enzymes.
Considering genital ulcerations in young women in industrialized societies, there are many differential diagnoses. Among the most likely diagnoses are HSV, candida, lichen planus, lichen sclerosus and aphthae (11). Ulcus vulva acutum is probably a rare diagnosis and might be caused by a primary EBV infection. Risk factors for sexually transmitted infections are often missing in EBV-associated ulcers. Syphilitic chancre must also be considered. The syphilitic sore, however, is often painless, in contrast to the EBV-associated ulcers. EBV-associated ulcers are characterized by pain and size >1 cm, and the patient frequently has symptoms of mononucleosis. Larger ulcers may be over-reported in the literature, so EBV should also be considered in cases of smaller, painful ulcers in the presence of other symptoms of mononucleosis and a negative HSV test.
The diagnosis of EBV-associated ulcers should be based on positive EBV serology or virus identification (e.g. PCR). However, as in our first case and three additional clinical reports (12, 13, 14), even sensitive specific serology may be negative when ulcer appears. We therefore recommend retesting of EBV serology in cases of uncertainty.
ACKNOWLEDGEMENTS
We thank Daniel de la Rosa-Carrillo, Kevin Sunde Oppegaard, Johannes Thorvaldsen, Florence Dalgard and Emilie Broquet for linguistic help.
REFERENCES
1. Andiman WA. Antibody Response to Epstein-Barr Virus. In: Rose NR, Friedman H, Fahey JL, eds. Manual of clinical laboratory immunology, 3rd edn. Washington DC: ASM, 1986: p. 509–514.
2. Brown ZA, Stenchever MA. Genital ulceration and infectious mononucleosis: report of a case. Am J Obstet Gynecol 1977; 127: 673–674.
3. Lipschütz B. Über eine eigenartige Geschwürsform des weiblichen Genitales (ulcus vulvae acutum). Arch Dermatol Syph (Berlin) 1913; 114: 363–395.
4. Portnoy J, Ahronheim GA, Ghibu F, Clecner B, Joncas JH. Recovery of Epstein-Barr virus from genital ulcers. N Engl J Med 1984; 311: 966–968.
5. Taylor S, Drake SM, Dedicoat M, Wood MJ. Genital ulcers associated with acute Epstein-Barr virus infection. Sex Transm Inf 1998; 74: 296–297.
6. Pelletier F, Leblanc L, Estavoyer J-M, Drobacheff C, Khayat AN, Laurent R. Ulcère de Lipschütz au cours d`une primo-infection à virus Epstein-Barr. Ann Dermatol Venereol 2002; 129: 905–907.
7. Lawee D, Shafir MS. Solitary penile ulcer associated with infectious mononucleosis. Can Med Assoc J 1983; 129: 146–147.
8. Bargman H. Penile ulcer and infectious mononucleosis. Can Med Assoc J 1983; 129: 1176.
9. Katz BZ. Epstein-Barr virus (mononucleosis and lymphoproliferative disorders). In: Long SS, Pickering LK, Prober CG, eds. Principles and practice of pediatric infectious diseases. 2nd edn, Philadelphia: Churchill Livingstone, 2003: p. 1059–1068.
10. Näher H, Gissmann L, Freese UK, Petzoldt D, Helfrich S. Subclinical Epstein-Barr virus infection of both the male and the female genital tract – indication for sexual transmission. J Invest Dermatol 1992; 98: 791–793.
11. Cheng SX, Chapman MS, Margesson LJ, Birenbaum D. Genital ulcers caused by Epstein-Barr virus. J Am Acad Dermatol 2004; 51: 824–826.
12. Sisson BA, Glick L. Genital ulceration as a presenting manifestation of infectious mononucleosis. J Pediatr Adolesc Gynecol 1998; 11: 185–187.
13. Lorenzo CV, Robertson WS. Genital ulceration as presenting symptom of infectious mononucleosis. J Am Board Fam Pract 2005; 18: 67–68.
14. Nicolas X, Ansart S, Jaffuel A, Deluc A, Le Berre R, Tandé D, et al. Ulcérations génitales au cours d’une primo-infection par le virus Epstein-Barr. La Revue de Médecine Interne 2005; 26: 913–916.
15. Groulier JL, Pellegrin JL, Marchal C, Massieres JP, Villanove X, Leng B. Ulcération génitale au cours d’une mononucléose infectieuse. Presse Méd 1986; 15: 2167.
16. McKenna G, Edwards S, Cleland H. Genital ulceration secondary to Epstein-Barr virus infection. Genitourin Med 1994; 70: 356–357.
17. Wilson RW. Genital ulcers and mononucleosis. Pediatr Infect Dis J 1993; 12: 418.
18. Navarro Llanos A, Doménech Climent V, Elizalde Eguinoa J, Pujol de la Llave E. Primoinfección por el virus de Epstein-Barr: una causa poco conocida de úlcera genital aguda. ¿Ulcera de Lipschütz’s¿ Rev Clin Esp 1996; 196: 570–571.
19. Lampert A, Assier-Bonnet H, Chevallier B, Clerici T, Saiag P. Lipschütz’s genital ulceration: a manifestation of Epstein-Barr virus primary infection. Br J Dermatol 1996; 135: 663–665.
20. Gisserot O, Carsuzaa F, Morand JJ, Marrot F. L’infection par le virus d’Epstein-Barr: une cause d’ulcération génitale. Sem Hôp Paris 1997; 73: 24–25.
21. Hudson LB, Perlman SE. Necrotizing genital ulcerations in a premenarcheal female with mononucleosis. Obstet Gynecol 1998; 92: 642–644.
22. Logeart I, Blondon H, Caulin C. Ulcère aigu de la vulve au cours d’une primo-infection a virus Epstein-Barr. La Presse Médicale 1998; 27: 571–572.
23. Svedman C, Holst R, Johnsson A. Ulcus vulvae acutum, a rare diagnosis to keep in mind. Eur J Obstet Gynecol Reprod Bio 2004; 115: 104–105.
24. Tenori V, Parra C, Uriz S, Castells L, Velázquez M. Febre i úlceres genitales en una nena de 2 anys. Pediatria Catalana 2004; 64: 88–89.


