


Finn Schultz Larsen1, Lene Simonsen2, Anita Melgaard2, Katja Wendicke2 and Anne S. Henriksen2
1Dermatology Clinic, Fredericia, and 2LEO Pharma A/S, Industriparken 55, Ballerup, Denmark
To relieve the dryness of atopic dermatitis skin, a lipid formulation of fusidic acid and betamethasone 17-valerate (Fucicort® Lipid cream) was developed as an additional treatment option to the established Fucicort® cream. The two formulations were compared in patients with clinically infected atopic dermatitis. A total of 629 patients were randomized to twice daily double-blind treatment for 2 weeks with either Fucicort® Lipid cream, Fucicort® cream, or the new lipid cream vehicle. Clinical assessment was based on a Total Severity Score of the eczematous lesions. Bacteriological samples were taken at inclusion and at subsequent visit(s) if clinically infected lesions persisted. At the end of treatment, the mean reduction in Total Severity score was 82.9% in the lipid cream group, 82.7% in the cream group, and 33.0% in the vehicle group. The percentage of patients with a successful bacteriological response was 89.7%, 89.6% and 25.0%, respectively. Thus, the clinical and anti-bacterial effect of the lipid cream was found to be similar to that of the established cream formulation, and significantly better than that of the vehicle. The new lipid formulation, therefore, offers an efficient, safe and well-tolerated alternative for the short-term treatment of clinically infected atopic dermatitis. Key words: lipid formulation; infected eczema; randomized controlled trial; combination therapy.
(Accepted May 23, 2006.)
Acta Derm Venereol 2007; 87: 62–68.
Finn Schultz Larsen, MD, PhD, Dermatology Clinic, Dronningensgade 72, DK-7000 Fredericia, Denmark. E-mail: finn.schultz.larsen@dadlnet.dk
Atopic dermatitis (AD) is one of the most common skin diseases in childhood, and the management of AD is a continuous challenge to the general practitioner as well as to the dermatologist (1). Colonization of the eczematous lesions with Staphylococcus aureus is common, and the bacterium is known to exacerbate and maintain skin inflammation by secretion of super-antigens (2, 3).
In clinically infected AD, topical treatment combining an antibiotic and a corticosteroid has been demonstrated to be superior to treatment with corticosteroids alone (4, 5). Hjorth et al. (6) and Ramsay et al. (7) have studied the combination of the antibiotic fusidic acid and the corticosteroids betamethasone 17-valerate and hydrocortisone acetate, respectively. Both studies clearly demonstrated that combination therapy is more effective than monotherapy. Moreover, several studies have confirmed that the combination of fusidic acid and betamethasone 17-valerate is similarly clinically effective as other combinations of corticosteroids and antibiotics (8–11). A simple cream formulation (Fucicort®, also known as Fucibet® in some European countries) combining the two drug substances has been used in clinically infected AD for more than a decade.
In the management of AD it is important to offer effective treatments that relieve the dryness of the eczematous skin. The patient’s need for emollients may vary with age, skin type, stage and type of eczema, climate and individual preferences. For those with dry skin, a lipid cream may especially be preferable because of its emollient properties, but without the greasiness of ointments. Therefore, a new formulation based on the efficient combination of fusidic acid and betamethasone 17-valerate was developed in a more lipid-rich formulation in order to satisfy the different needs and preferences of the patients.
The aim of the present study was to compare the efficacy and safety of fusidic acid and betamethasone 17-valerate combined in a new lipid formulation (Fucicort® Lipid cream) to the established formulation (Fucicort® cream) in patients with clinically infected AD. It is the overall goal that the new lipid cream will offer an alternative treatment option, increasing patient satisfaction, and thus become a valuable alternative in the management of clinically infected AD.
Materials and methods
This was an international, multicentre, prospective, randomized, double-blind, three-arm, parallel-group, active and vehicle-controlled, comparative phase III study conducted in six European countries and involving 49 centres. The protocol was approved by all relevant health authorities and ethics committees, and all patients gave signed informed consent. The study was conducted to conform to the principles of the Declaration of Helsinki.
Patient selection
Out-patients of either sex, aged 6 years or older, who had a clinical diagnosis of infected AD were enrolled. The study period was from March 2001 to May 2002. The diagnosis of clinically infected AD was based on a clinical evaluation. The diagnosis of AD was according to the criteria of Hanifin & Rajka (12). The patients enrolled had a target lesion of at least 4×4 cm with a minimum score of “1” for each of the items scored (see Clinical Assessments). Females of childbearing age had a negative pregnancy test and agreed to use an adequate method of contraception during the study.
Patients were excluded if they had a known or suspected history of allergy to any of the ingredients of the trial medication, had current signs of viral or fungal infection, had skin lesions such as scarring and hyperpigmentation that could confound the assessment, or if they had received systemic immunosuppressives, oral steroids, UVB within the previous 2 weeks, PUVA or antibiotics within the previous 4 weeks, or any other topical therapy (except group I and II corticosteroids, and emollients) within the previous week. Planned exposure to sun, UVA or UVB, current participation in other clinical studies, the use of unregistered drugs within the previous month, suspected risk of protocol non-compliance, pregnancy, and breast-feeding were additional exclusion criteria.
Treatment assignment
Patients were randomized in the ratio 3:3:1 to the following treatment groups: (I) fusidic acid (20 mg/g) and betamethasone 17-valerate (1 mg/g) in the new lipid cream (Fucicort® Lipid cream, LEO Pharma, Ballerup, Denmark); (II) fusidic acid (20 mg/g) and betamethasone 17-valerate (1 mg/g) in the cream (Fucicort® cream); and (III) the new lipid cream vehicle (not commercially available). Treatments were assigned according to a pre-planned computer-generated randomization schedule. The study was considered as double-blind even though it was possible to distinguish between the lipid cream and the cream formulation. To prevent identification of the different formulations, the investigational products were packed in identical packaging.
The treatment was applied twice daily to all the eczematous areas, except on the face. If relevant, a group I topical steroid (Mildison®, Yamanouchi Pharmaceutical Co., München, Germany) was allowed for treatment of facial lesions. An emollient cream (Locobase®, Yamanouchi Pharmaceutical Co.) could be used as needed outside the treatment areas.
Clinical assessments
Patients were assessed at inclusion (visit 1), and again after one (visit 2) and 2 weeks (visit 3) of treatment. In patients who reported treatment-related adverse events, a follow-up contact was arranged 2 weeks later.
At inclusion, a target lesion of at least 4×4 cm was selected. The severity of the following signs: erythema, oedema/papulation, oozing/crusting, and excoriation was assessed on a 4-point scale ranging from “absent” to “severe involvement”, and a Total Severity Score (TSS) (maximum score 12) was calculated based on these signs. The TSS of the target lesion was reassessed at visits 2 and 3. In order to reduce inter-personal variability, the same investigator assessed the patient at each visit, if possible.
At visits 2 and 3, both the investigator and the patient recorded the overall treatment efficacy of the whole treatment area (i.e. excluding the face) relative to baseline on a 6-point scale: “worse”, “unchanged”, “minimal improvement”, “moderate improvement”, “marked improvement”, or “complete clearance”. Patients with “marked improvement” or “complete clearance” were defined as responders. Finally, the patients’ cosmetic acceptance of the trial medication was recorded at visit 2 using a 4-point scale ranging “unacceptable”, “acceptable”, “good”, and “very good”.
Compliance with trial medication was recorded at visits 2 and 3, and the total amount of trial medication applied during the treatment period was determined by assessing the weight of return medication.
Microbiological assessments
A microbiological swab was taken from the target lesion at inclusion and at the end of treatment by rubbing the swab on the surface of the lesion. The swabs were immersed in a transport medium and sent to a central laboratory for investigation (GR Micro, London, UK). The presence of S. aureus and beta-haemolytic streptococci was detected by conventional methods. In vitro susceptibility of the isolates to penicillin, erythromycin, gentamicin and oxacillin (for methicillin) was determined by the standard disc diffusion procedure according to the methods recommended by the Clinical Laboratory Standards Institute (CLSI) (13). If an intermediate classification was obtained for oxacillin against S. aureus, the oxacillin-salt agar test was performed. As CLSI does not provide criteria for testing susceptibility of beta-haemolytic streptococci to gentamicin, all beta-haemolytic streptococci were reported as resistant to gentamicin.
For fusidic acid, the minimum inhibitory concentration (MIC) of S. aureus and beta-haemolytic streptococci was determined by a microdilution broth method using CLSI methodology (14). Since there are no CLSI criteria for defining resistance to fusidic acid, the following interpretations were used to define susceptibility to fusidic acid; susceptible: MIC <2 mg/l; intermediate: MIC=2 mg/l; and resistant: MIC ≥4 mg/l.
The bacteriological treatment response was defined as “successful” in patients who at visit 1 had pathogens on the target lesion and had either the baseline pathogen eradicated or no visible target lesion (presumptive eradication) at the end of treatment. Patients in whom pathogens persisted were classified as “failures”.
Statistical methods
All randomized patients who gave informed consent constituted the intention-to-treat (ITT) population. The per protocol (PP) population was defined by exclusion of patients from the ITT population who provided no efficacy data following start of treatment, who did not take any trial medication, were known to have taken the wrong trial medication, or who did not fulfil the disease definition criteria as defined by the inclusion criteria. Furthermore, patients’ data were completely or partially excluded from the PP analysis set if the trial medication had been inappropriately used, if other medication that could affect the disease had been used, if the interval between visits 1 and 2 was more than 10 days, or if the interval between visits 1 and 3 was more than 21 days. The safety population comprised all patients who had used the trial medication and provided safety data.
As recommended by the ICH E9 guideline (15), primarily the PP population was used to compare the efficacy of the two active formulations as the study was designed to show non-inferiority of Fucicort® Lipid cream to Fucicort® cream. Based on a non-inferiority margin of 10%, a power of 80% and a 2.5% significance level for the one-sided test, 270 patients were required in each active treatment arm assuming no true difference between the formulations and a standard deviation of 40% for the primary response criterion. The ITT population was used to compare the efficacy of the Fucicort® Lipid cream and the lipid cream vehicle as this part of the study was designed to detect superiority of the active formulation. With 90 patients in the vehicle group, the comparison between active and vehicle would have at least 80% power to detect a difference of 15% at a 5% significance level (two-sided) assuming a common standard deviation of 40%.
In both comparisons, the primary response criterion was the percentage reduction in TSS of the target lesion. The analysis was done by analysis of covariance with treatment group and centre as design variables, and with baseline TSS as covariate. In the event of missing data, the “last observation carried forward”-approach was used. SAS software (16) was used for the statistical analysis.
Results
Demographics and baseline characteristics
The ITT population comprised 629 patients (275 patients in Fucicort® Lipid cream group, 264 in Fucicort® cream group, and 90 in the vehicle group) (Table I). Recruitment per centre ranged from 1 to 35 patients.
In total, 15 patients were excluded from the PP population: 9 patients provided no efficacy data, 2 violated the study period, 2 took prohibited medication, one did not fulfil the protocol inclusion criteria with respect to presence of disease, and one did not use the trial medication. Therefore, the PP population comprised 614 patients (274 patients on Fucicort® Lipid cream, 254 patients on Fucicort® cream, and 86 patients on vehicle treatment).
Table I. Baseline characteristics of atopic dermatitis (AD) patients in the intention-to-treat (ITT) population
| Fucicort® Lipid cream (n=275) | Fucicort® cream (n=264) | Lipid cream vehicle (n=90) | |
| Male | 114 | 124 | 45 |
| Female | 161 | 140 | 45 |
| Age (years, mean ± SD) | 24.8 ± 14.7 | 26.1 ± 14.3 | 26.7 ± 15.2 |
| Duration of AD (years, mean ± SD) | 15.2 ± 12.5 | 15.6 ± 12.3 | 18.2 ± 13.3 |
| TSS (mean ± SD) | 8.3 ± 1.9 | 8.2 ± 1.7 | 8.2 ± 1.7 |
| No (%) of patients with: | |||
| Erythema | |||
| Slight | 19 (6.9) | 16 (6.1) | 3 (3.3) |
| Moderate | 150 (54.5) | 158 (59.8) | 57 (63.3) |
| Severe | 106 (38.5) | 90 (34.1) | 30 (33.3) |
| Oedema | |||
| Slight | 54 (19.6) | 62 (23.5) | 22 (24.4) |
| Moderate | 164 (59.6) | 153 (58.0) | 48 (53.3) |
| Severe | 57 (20.7) | 49 (18.6) | 20 (22.2) |
| Oozing | |||
| Slight | 65 (23.6) | 62 (23.5) | 19 (21.1) |
| Moderate | 141 (51.3) | 139 (52.7) | 53 (58.9) |
| Severe | 69 (25.1) | 63 (23.9) | 18 (20.0) |
| Excoriation | |||
| Slight | 68 (24.7) | 61 (23.1)a | 24 (26.7) |
| Moderate | 137 (49.8) | 147 (55.7) | 50 (55.6) |
| Severe | 70 (25.5) | 55 (20.8) | 16 (17.8) |
aOne patient had no excoriation.
TSS: Total severity score, SD: standard deviation.
The safety population comprised a total of 620 patients (274 patients on Fucicort® Lipid cream, 258 patients on Fucicort® cream, and 88 patients on vehicle treatment) as 1 patient did not take trial medication and 8 patients did not provide safety data due to withdrawal after visit 1. A total of 45 patients who contributed to the baseline data were withdrawn during the study: 10 (4%) in the Fucicort® Lipid cream group, 18 (7%) in the Fucicort® cream group and 17 (19%) in the vehicle group. For 12 patients (13%) in the latter group, the reason for leaving the study was insufficient effect of the lipid cream vehicle alone.
At baseline, the treatment groups were well matched for age, sex, duration of AD, TSS, and severity of the individual signs of AD (Table I).
Efficacy
Fucicort® Lipid cream vs. Fucicort® cream. The mean percentage reductions in TSS of the target lesion from baseline to end of treatment in the PP population were 82.9% in the Fucicort® Lipid cream and 82.7% in the Fucicort® cream group (Fig. 1). The estimated difference was 0.23% with 95% confidence interval (95% CI) ranging from –3.83 to 4.30 (test for inferiority; p<0.001). This is well within the predefined 10% non-inferiority limit. Thus, the clinical effect of the two products was found to be similar. The same analysis on the ITT population showed similar results (data not shown).
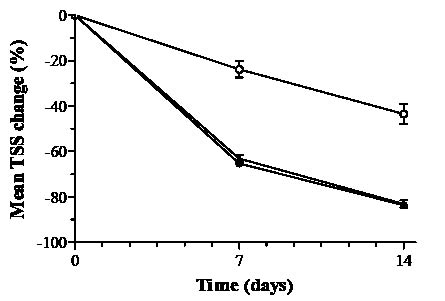
Fig.1. Mean percentage changes in total severity score (TSS) of the target lesion after treatment with Fucicort® Lipid cream (), Fucicort® cream(), or lipid cream vehicle () (mean ± SE).
According to the investigators’ overall assessment of efficacy, 83.5% of the patients in the Fucicort® Lipid cream group and 84.0% in the Fucicort® cream group were responders at end of treatment (PP population). The difference between the proportion of responders in the active treatment groups was –0.5% (95% CI –6.8 to 5.8).
The patients’ overall assessment of efficacy revealed similar results as 82.1% of the patients in the Fucicort® Lipid cream group and 84.0% in the Fucicort® cream group were responders at end of treatment (PP population). The difference between the proportion of responders in the active treatment groups was –2.0% (95% CI –8.4 to 4.5).
Fucicort® Lipid cream vs. lipid cream vehicle. The mean percentage reductions in the TSS from baseline to end of treatment in the ITT population were 82.7% in the Fucicort® Lipid cream group and 33.0% in the vehicle group (Fig. 1). The estimated treatment difference was 48.3% (95% CI 41.0–55.7, p < 0.001) demonstrating a statistically significant superior effect of the lipid cream as compared with vehicle. The same analysis on the PP population showed similar results (data not shown).
According to the investigators’ overall assessment of efficacy, 83.6% of the patients in the Fucicort® Lipid cream group and 30.7% in the vehicle group were responders at end of treatment (ITT population). The difference between the proportion of responders in the lipid cream group and the vehicle group was 52.9% (95% CI 42.3–63.5, p <0.001) in favour of Fucicort® Lipid cream.
The patients’ overall assessment of efficacy at end of treatment revealed similar results as 82.1% of the patients in the Fucicort® Lipid cream group and 29.6% in the vehicle group were responders (ITT population). The difference between the lipid cream and the vehicle was 52.6% (95% CI 42.0–63.1, p < 0.001) in favour of Fucicort® Lipid cream.
Compliance
Compliance with the trial medication was acceptable, in the sense that medication was used as prescribed during the treatment period in 86.9% of the patients given Fucicort® Lipid cream, in 88.4% of the patients given Fucicort® cream, and in 86.4% of the patients given the lipid cream vehicle. The mean use of trial medication was 51.6 g of Fucicort® Lipid cream, 50.3 g of Fucicort® cream, and 51.5 g of the lipid cream vehicle.
Cosmetic acceptance
The patients’ assessment of the cosmetic acceptance of the trial medications was similar in the two active treatment groups, 86.8% of the patients treated with Fucicort® Lipid cream considered the product to have good or very good cosmetic acceptance compared with 85.5% of the patients treated with Fucicort® cream. In the vehicle group, 69.3% of the patients treated with the vehicle rated it as having good or very good cosmetic acceptance.
Bacteriology
S. aureus alone, or together with beta-haemolytic streptococci, was isolated from the lesions of 416 patients (66.1%) at visit 1, whereas beta-haemolytic streptococci were found alone in only 5 patients (0.8%). The susceptibility of the S. aureus isolates to the antibiotic tested is shown in Table II. The resistance to penicillin among the isolates was 77%, and the erythromycin resistance was 20%. The overall susceptibility to fusidic acid was around 90%, but varied from country to country (77.4% in Denmark to 97.1% in Finland).
The percentages of patients with a successful bacteriological response were similar in the two active treatment groups: 89.7% for the Fucicort® Lipid cream and 89.6% for the Fucicort® cream (PP analysis). For the comparison between active treatment and the vehicle, a successful bacteriological response of 87.8% was obtained for the Fucicort® Lipid cream and 25.0% for the vehicle (ITT analysis set). The estimated difference between the Fucicort® Lipid cream and the vehicle group was 62.9% (95% CI 52.0–73.7, p < 0.001).
Table III shows the bacteriological response in patients infected with fusidic acid susceptible isolates at baseline. Active treatment successfully eradicated fusidic acid susceptible isolates in 94.1% of patients. Vehicle treatment was similarly successful in 35.2%. Fusidic acid intermediate/resistant isolates were detected after treatment in 7 patients (2.3%) given active treatment and in one patient (1.9%) given vehicle.
Table II. Antimicrobial susceptibility of S. aureus isolates in all countries at the beginning of the study (n = 426)
| Antimicrobial agent | Number of isolates (%) | ||
| Susceptible | Intermediate | Resistant | |
| Fusidic acid | 388 (91.1) | 10 (2.3) | 28 (6.6) |
| Penicillin | 99 (23.2) | 0 (0) | 327 (76.8) |
| Methicillin | 421 (98.8) | 0 (0) | 5 (1.2) |
| Erythromycin | 335 (78.6) | 5 (1.2) | 86 (20.2) |
| Gentamicin | 411 (96.5) | 1 (0.2) | 14 (3.3) |
Table III. Susceptibility of S. aureus to fusidic acid at end of treatment in patients infected with susceptive isolates at baseline (all strains were susceptible at baseline)
| Susceptibility at end of treatment | No pathogens n (%) | Susceptible n (%) | Intermediate/resistant n (%) |
| Active treatment group (n = 303) | 285 (94.1%) | 11 (3.6%) | 7 (2.3%) |
| Vehicle treatment group (n = 54) | 19 (35.2%) | 34 (63.0%) | 1 (1.9%) |
Safety
Adverse events were reported by 37 of the 274 patients (13.5%) in the Fucicort® Lipid cream group, by 27 of the 258 patients (10.5%) in the Fucicort® cream group, and by 19 of the 88 patients (21.6%) in the vehicle group. There were no statistically significant differences between the active treatments or between the lipid cream and the vehicle in the incidence of adverse advents.
Lesional or perilesional adverse drug reactions were reported by 7 patients (2.6%) in the Fucicort® Lipid cream group, by 4 patients (1.6%) in the Fucicort® cream group, and by 12 patients (13.6%) in the vehicle group (Table IV). Significantly fewer adverse drug reactions were recorded in the lipid cream group compared with the vehicle group (p < 0.001). The most frequently reported adverse drug reactions were pruritus and skin burning sensation, as coded according to the Medical Dictionary for Regulatory Activities. A total of 5 patients ceased treatment due to unacceptable adverse events; 1 given the Fucicort® Lipid cream (erythema) and 4 given the vehicle (itching/burning, skin pain, and contact dermatitis).
Table IV. Adverse drug reactions reported
| Fucicort® Lipid cream (n=274) | Fucicort® cream (n=258) | Lipid cream vehicle (n=88) | |
| Contact dermatitis | 0 | 0 | 1 |
| Dry skin | 0 | 0 | 1 |
| Erythema | 1 | 0 | 0 |
| Prurigo | 0 | 0 | 1 |
| Pruritus | 2 | 0 | 6 |
| Skin burning sensation | 3 | 3 | 4 |
| Skin irritation | 0 | 1 | 0 |
| Skin tightness | 0 | 0 | 1 |
| Skin pain | 0 | 0 | 1 |
| Urticaria | 1 | 0 | 0 |
| Total no. of reactions | 7 | 4 | 15 |
| Total no. of patients (%) | 7 (2.6%) | 4 (1.6%) | 12 (13.6%) |
Discussion
This study has demonstrated that short-term treatment with Fucicort® Lipid cream and Fucicort® cream are similarly effective in the management of clinically infected AD. A large group of patients was enrolled and the desired number of patients was randomized to the three treatment groups. The study population was representative of out-patients with clinically infected AD. The symptoms of clinical infection were presence of weeping discharge on acute eczematous lesions resulting in an oozing and crusting appearance (17). The diagnosis of infection was based on the investigator’s clinical judgement, whereas the diagnosis of AD was made according to the criteria of Hanifin & Rajka (12). The treatment groups were comparable in respect of demographic variables and clinical and bacteriological findings. The response criteria employed were appropriate, compliance with trial medication was good, and few patients were lost to follow-up. The mean TSS on entry was 8.3 (range 4–12) indicating that the study population represented a wide clinical spectrum of out-patients with AD.
Both active treatments reduced the TSS by around 83% at the end of treatment. An equally rapid onset of action was observed in both groups during the first week of treatment, as demonstrated by the two-thirds reduction in the TSS. The new lipid cream was significantly more effective than the vehicle. Both the investigators’ and the patients’ assessment of the overall clinical response confirm the similar efficacy of the two active treatment formulations. In addition, the cosmetic acceptance of both active treatments was equally high. Our clinical results are in accordance with previous studies. Hjorth et al. (6) assessed the clinical efficacy in 81 patients in a double-blind left/right comparison of the combination of the antibiotic fusidic acid and the corticosteroid betamethasone 17-valerate by means of symptoms score, and demonstrated a reduction of 75% for the combination therapy. Furthermore, in 46 patients (out of the 81 evaluated) the investigator judged that therapy was more effective on one side compared with the other, and in 32 of these 46 patients, combination therapy was statistically significantly more effective (6). Also, in the study by Javier et al. (8), treatment with the fusidic acid/betamethasone cream proved effective in 85% of the cases. Wilkinson et al. (11) found a success rate of 95% in a similar group of patients given the same treatment.
In our study, the bacteriological cure rate was 90% in both active treatment groups compared with 25% in the vehicle group. Our results on bacterial eradication are in agreement with the retrospective analysis of eight clinical studies performed by Menday & Noble (10), who reported a bacteriological efficacy of 89.6% in 364 patients. In addition, in the study by Hjorth et al. (6), the bacteriological cure rate was assessed. In 51 patients bacteria were found at the first visit, 44 of them having S. aureus isolated from the lesions. After 7 days of treatment, the number of Gram-positive cocci was reduced by 81% by the combination therapy, and by 66% by plain betamethasone treatment.
Although our current understanding of the dysfunctional immune system in AD suggests that antimicrobial treatment should be effective, it has been discussed whether a topical combination of antibiotic and steroid is more efficacious than the steroid alone in treatment of infected dermatoses (18). For example, in the study by Wachs & Maibach (5) on the therapeutic effect of gentamicin and betamethasone, the clinical and bacteriological results appeared to favour the use of the combination over gentamicin alone, but the data was not statistically significant at all investigated parameters. For fusidic acid, the combination with a steroid has, however, been demonstrated to be beneficial in infected AD (6, 7).
The safety profiles of fusidic acid and betamethasone 17-valerate are well known (3). In the present study, lesional or perilesional drug reactions (typically pruritus and skin burning) were reported in about 2% of the patients in the active treatment groups. In contrast, a higher number of patients (14%) in the vehicle group reported similar reactions. This is considered due to the lack of a corticosteroid in the vehicle.
This study has confirmed that S. aureus is frequently present in clinically infected AD as it was isolated from 416 (66.1%) out of 629 patients. It is known that S. aureus isolates increase with the severity of the disease (3, 4, 19, 20). In our study, the incidence was lower than that reported by Abeck & Mempel (3), but similar to that observed in patients with mild to moderate lesions by Ramsay et al. (7) and Hjorth et al. (6).
In the S. aureus isolates grown in this study, almost 80% were resistant to penicillin, which is consistent with previous findings (21). Twenty percent were resistant to erythromycin, similar to that seen in methicillin susceptible strains from out-patients (22, 23). In our study, only 1% of the isolates were methicillin resistant S. aureus (MRSA), and these were only detected in Belgium. Reports on the percentage of MRSA vary from country to country and amongst the type of patients studied. A recent study in skin and soft tissue infection out-patients in the USA and in Europe reported of 29.1% MRSA in the USA, 27.9% in France, 27.4% in Italy, 14.8% in Spain and 4% in Germany (22). In some countries, resistance to fusidic acid in S. aureus has been reported to have increased in recent years (24–26). Our observations confirm that resistance exists in some regions of a country such as Denmark (22%), but is rare in other countries such as Finland (3%).
Our study was prospective and enables us to examine the emergence of fusidic acid resistance associated with the use of short-term fusidic acid and betamethasone therapy in clinically infected AD. Selection of S. aureus isolates resistant to fusidic acid was seen in only 2.3% of patients applying Fucicort®. This was not statistically significantly different from that seen in the vehicle treated group (Table III). However, selection of resistance was seen in only one patient given the vehicle, and such a comparison has to be viewed carefully. On the other hand, Menday & Noble (10), who reviewed the bacteriological outcome of fusidic acid and betamethasone treatment of dermatitis, reported a virtually identical outcome. In their study at the end of treatment, fusidic acid resistance was seen in 9 of 327 patients (2.8%) with a fusidic acid susceptible “infection”. In patients given a comparator treatment, primarily betamethasone with or without another antibiotic, resistance to fusidic acid “emerged” in 6 of 241 patients (2.5%) (10). Similarly, Ravenscroft et al. (27) found no evidence to support the hypothesis that short-term treatment of AD with topical fusidic acid and a corticosteroid increased fusidic acid resistant S. aureus during a 2-week treatment period. None of these data indicate a significant causal relationship between the short-term use of topical fusidic acid and increasing resistance. However, long-term use of topical antibiotics, including fusidic acid, may lead to emergence of resistant bacteria (28).
Poor patient compliance is a potential cause of treatment failure in AD. In addition to efficacy, the vehicle properties of the formulation therefore become an important factor. The choice of formulation will depend on the individual patient preference influenced by the dryness of the skin. Some patients may prefer a conventional cream formulation, while others may prefer a more lipid-rich formulation. In the present study, the cosmetic acceptance of the two cream formulations was found to be equally high, indicating that both the lipid cream and the conventional cream satisfied the patients’ needs and preferences. A high cosmetic acceptance is expected to increase patient compliance, thereby contributing to treatment success.
In conclusion, the new Fucicort® Lipid cream is as effective and well-tolerated as Fucicort® cream in the short-term treatment of clinically infected AD. The lipid cream formulation is thus a valuable treatment alternative to the established cream and gives both patients and doctors the choice of two similarly effective formulations depending upon the individual preferences and needs for emollient effect on the eczematous skin lesions.
Acknowledgements
The authors would like to thank the following main (≥10 patients recruited) investigators: J. Porters (Turnhout, BE), P. Roquet-Gravy (Marchienne-au-Pont, BE), E. Suys (Kortrijk, BE), J. Decroix (Mouscron, BE), M. Morren (Mechelen, BE), R. Kaufmann (Frankfurt am Main, DE), J. Ring (München, DE), M. Sebastian (Mahlow, DE), B. Gerlach (Dresden, DE), C. Meyer (Berlin, DE), N. Veien (Aalborg, DK), F.G. Larsen (Copenhagen, DK), A. Garcia (Madrid, ES), M. Casado (Madrid, ES), M. Ruer-Mulard (Martigues, FR), P. Lepeytre (Nice, FR) G. Rostain (Nice, FR), P. Autio (Helsinki, FI), S. Pitkänen (Helsinki, FI).
Conflict of interest: FSL has no affiliation or involvement to LEO Pharma. The other authors are employees at the Medical, Statistical, and CM Dermatological Departments at LEO Pharma, Ballerup, Denmark.
References
1. Schultz Larsen F, Hanifin JM. Epidemiology of atopic dermatitis. Immunol All Clin North America 2002; 22: 1–24.
2. Leung DYM, Bieber T. Atopic dermatitis. Lancet 2003; 361: 151–160.
3. Abeck D, Mempel M. Staphylococcus aureus colonisation in atopic dermatitis and its therapeutic implications. Br J Dermatol 1998; 139: 13–16.
4. Leyden JJ, Marples RR, Kligman AM. Staphylococcus aureus in the lesions of atopic dermatitis. Br J Dermatol 1974; 90: 525–530.
5. Wachs GN, Maibach HI. Co-operative double-blind trial of an antibiotic/corticoid combination in impetiginized atopic dermatitis. Br J Dermatol 1976; 95: 323–328.
6. Hjorth N, Schmidt H, Thomsen K. Fusidic acid plus betamethasone in infected or potentially infected eczema. Pharmatherapeutica 1985; 4: 126–131.
7. Ramsay CA, Savoie JM, Gilbert M, Gidon M, Kidson P. The treatment of atopic dermatitis with topical fusidic acid and hydrocortisone acetate. J Eur Acad Dermatol Venereol 1996; 7 (suppl 1): 15–22.
8. Javier PR, Ortiz M, Torralba M, Montinola FL, Lim KE, Canete R. Fusidic acid/betamethasone in infected dermatoses – a double-blind comparison with neomycin/betamethasone. Br J Clin Prac 1986; 40: 235–238.
9. Strategos J. Fusidic acid-betamethasone combination in infected eczema: an open, randomized comparison with gentamicin-betamethasone combination. Pharmatherapeutica 1986; 4: 601–606.
10. Menday AP, Noble WC. Topical betamethasone/fusidic acid in eczema: efficacy against and emergence of resistance in Staphylococcus aureus. J Dermatol Treat 2000; 11: 143–149.
11. Wilkinson JD, Leigh DA, Menday AP. Comparative efficacy of betamethasone and either fusidic acid or neomycin in infected or potentially infected eczema. Curr Ther Res 1985; 38: 177–182.
12. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol 1980; suppl 92: 44–47.
13. National Committee for Clinical Laboratory Standards. Performance standards for antimicrobial disk susceptibility tests; approved standard. Seventh edition. NCCLS document M02-A7. Wayne, PA, US, 2000.
14. National Committee for Clinical Laboratory Standards. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically. Approved standard. Fifth edition. NCCLS document M07–A5. Wayne, PA, US, 2000.
15. Note for guidance on statistical principles for clinical trials. The European Agency for the Evaluation of Medicinal Products. CPMP/ICH/363/96. London, UK, 1998.
16. SAS Institute Inc., SAS OnlineDoc®, version 8, Cary, NC, USA. SAS Institute Inc., 1999.
17. Lacour M, Hauser C. The role of microorganisms in atopic dermatitis. Clin Rev Allergy 1993; 11: 491–522.
18. Leyden JJ, Kligman AM. The case for steroid-antibiotic combinations. Br J Dermatol 1977; 96: 179–187.
19. Lever R, Hadley K, Downey D, Mackie R. Staphylococcal colonization in atopic dermatitis and the effect of topical mupirocin therapy. Br J Dermatol 1988; 119: 189–198.
20. Stalder JF, Fleury M, Sourisse M, Rostin M, Pheline F, Litoux P. Local steroid therapy and bacterial skin flora in atopic dermatitis. Br J Dermatol 1994; 131: 536–540.
21. Filius PM, Gyssens IC. Impact of increasing antimicrobial resistance on wound management. Am J Clin Dermatol 2002; 3: 1–7.
22. Jones ME, Karlowsky JA, Draghi DC, Thornsberry C, Sahm DF, Nathwani D. Epidemiology and antibiotic susceptibility of bacteria causing skin and soft tissue infections in the USA and Europe: A guide to appropriate antimicrobial therapy. Int J Antimicrob Agents 2003; 22: 406–419.
23. Korting HC, Neubert U, Abeck D. Current antimicrobial susceptibility of cutaneous bacteria to first line antibiotics. Int J Antimicrob Agents 1998; 10: 165–168.
24. Osterlund A, Eden T, Olsson-Liljequist B, Haeggman S, Kahlmeter G. Clonal spread among Swedish children of Staphylococcus aureus resistant to fusidic acid. Scand J Inf Dis 2002; 34: 729–734.
25. Livermore D, James D, Duckworth G, Stephens P. Fusidic acid use and resistance. Lancet 2002; 360: 806.
26. Mason BW, Howard AJ, Magee JT. Fusidic acid resistance in community isolates of methicillin-susceptible Staphylococcus aureus and fusidic acid prescribing. J Antimicrob Chemother 2003; 51: 1033–1036.
27. Ravenscroft JC, Layton AM, Eady EA, Murtagh MS, Coates P, Walker M, Cove JH. Short-term effects of topical fusidic acid or mupirocin on the prevalence of fusidic acid (FusR) Staphylococcus aureus in atopic eczema. Br J Dermatol 2003; 148: 1010–1017.
28. Perera G, Hay R. A guide to antibiotic resistance in bacterial skin infections. J Eur Acad Dermatol Venereol. 2005; 19: 531–545.

