


Henrik F. Lorentzen1, Kaare Weismann2, Kristian Rossen3 and Henrik Klem Thomsen3
1Department of Dermatology, Odense University Hospital, Odense, 2Dermatological Clinic, Hørsholm Hospital, and 3Department of Pathology, Bispebjerg University Hospital, Copenhagen, Denmark
Dermatoscopy increases the accuracy of diagnosis of melanoma. An atypical vascular pattern may be an indicator of cutaneous malignant melanoma (CMM). During dermatoscopy of certain CMMs numerous ruby droplets of blood appear when the dermatoscope is pressed firmly against the lesion. The aim of this paper was to examine the histopathological background for this observation. CMMs from 8 patients showing the poppyfield sign, i.e. squirts of ruby blood droplets, were paired with 8 CMMs of equal Breslow thickness not showing this sign. The 16 CMMs were placed in an unsystematic sequence and presented to two dermato-pathologists who assessed the lesions independently for confirmation of Breslow thickness, Clark level, ulceration and presence of dilated tumour vessels. There was no disagreement between the pathologists’ assessments. Age of the patients and Breslow thickness of the cutaneous malignant melanoma were similar in the two groups. All 8 poppyfield CMMs had dilated tumour vessels compared with 25% (2/8) of the non-poppyfield CMMs (p < 0.007). Histological ulceration was observed in all poppyfield CMMs and none of the non-poppyfield CMMs (p < 0.001). The poppyfield bleeding sign is a dermatoscopic clue to dilated tumour vessels. It may be a dermatoscopic reflection of increased vascular density described in primary CMMs compared with adjacent skin and may also reflect the presence of primitive vessels in CMMs displaying increased fragility. Key words: melanoma; dermoscopy; ulceration; prognosis.
(Accepted August 10, 2006.)
Acta Derm Venereol 2007; 87: 149–151.
Henrik F. Lorentzen, Department of Dermatology, Odense University Hospital, DK-5000 Odense, Denmark. E-mail: Lorentzen@dadlnet.dk
The incidence of cutaneous malignant melanoma (CMM) is increasing and, despite case-finding actions and public education initiatives, dermatologists are recurrently challenged with advanced primary CMM. For formally trained observers, dermatoscopy increases diagnostic performance (1). Various diagnostic algorithms have been suggested (2–4), but none enables 100% sensitivity or specificity (5–7). For this reason additional “clues” to the dermatoscopic diagnosis of CMM are desirable.
Over the past decade we have repeatedly observed characteristic bleeding from some CMMs during dermatoscopy. When the hand-held dermatoscope is pressed firmly over the CMM, we have observed small ruby squirts of blood with a diameter of approximately 0.2 mm, resembling a field of poppies, hence the designation “poppyfield sign”. The aim of this study was to investigate the histopathological background for this observation.
Dermatoscopic or epiluminescence microscopic images are projections of features perpendicular to the skin surface, as seen by histopathology, to a flat plane parallel to the skin surface. Close cooperation between dermatologists and dermatopathologists is imperative for understanding dermatoscopy.
Materials and methods
Dermaphot pictures were taken with a Heine Dermaphot mounted on a Minolta SLR camera using a 64 ASA Kodak film with a colour temperature of 21°C. Primary excision was performed with a 5-mm margin. Tissue sections were stained with haematoxylin-eosin and S-100 (8) and HMB-45 (9) immunostains.
Our database of pigmented skin lesions was searched for those showing the poppyfield sign. Eight CMMs showing this sign were identified. Eight lesions not showing the poppyfield sign, but having similar Breslow thickness, were selected from the database for further comparison. The 16 CMMs were reassessed independently by two dermatopathologists, who were blinded to the clinical dermatoscopic observations. The CMMs were presented to the pathologists in random order. The lesions were assessed for confirmation of the diagnosis of CMM, Breslow thickness, extravasation of erythrocytes, vascular density, and dilation of capillaries and venules. Assessments were performed on prefabricated entry-sheets, which were subsequently returned for data analysis not leaving possibilities for corrections once assessments were performed. We analysed the 2 × 2 contingency table of the proportions using Fisher's exact test and unpaired t-test was used for comparison of parametric data. A p-value of 0.05 was considered significant.
The melanomas were also compared with ulcerated basal cell carcinomas from the database published previously (1) and with the in situ CMMs and CMMs with Breslow thickness less than 1 mm.
Results
Patient characteristics and histopathology data are summarized in Table I.
Table I. Histology and dermatoscopy for 8 thick melanomas with poppyfield sign and 8 thick melanomas without poppyfield sign
| Case | Age (years) | Gender | Site | Breslow (mm) | Clark level | Dilated vessels |
| With poppyfield sign | ||||||
| 1 | 87 | F | Arm | 3.7 | IV | + |
| 2* | 91 | F | Cheek | > 4.5 | IV | + |
| 3 | 78 | F | Thorax | 1.5 | III | + |
| 4 | 99 | F | Calf | 2.5 | IV | + |
| 5 | 80 | M | Thorax | 2.6 | IV | + |
| 6 | 66 | M | Back | 4.3 | IV | + |
| 7 | 77 | F | Shin | 2.4 | IV | + |
| 8 | 65 | F | Thorax | 3.9 | IV | + |
| Without poppyfield sign | ||||||
| 1 | 71 | M | Back | 4.0 | IV | + |
| 2 | 72 | M | Abdomen | 2.2 | III | – |
| 3 | 74 | F | Shoulder | 1.3 | II | – |
| 4 | 77 | F | Calf | 3.5 | V | + |
| 5 | 90 | F | Back | 2.7 | III | – |
| 6 | 71 | M | Thigh | 3.1 | IV | – |
| 7 | 79 | M | Arm | 1.7 | IV | – |
| 8 | 90 | F | Thigh | 3.0 | IV | – |
*Primarily incompletely removed lesions.
There were no disagreements between the two pathologists. The average Breslow thickness in the poppyfield group was 3.2 mm (95% confidence level (CI) 2.3–4.1 mm) and that of the non-poppyfield group 2.7 mm (95% CI 1.9–3.4 mm). The difference was not significant (p = 0.3). The average age of the patients was 80 years in the poppyfield group, compared with 78 years in the non-poppyfield group (p = 0.64).
The proportion of dilated vessels in the poppyfield group was 8/8 (100%), whereas the proportion was 2/8 (25%) in the non-poppyfield group (p = 0.007). Histopathological ulceration occurred in all 8 poppyfield CMMs (100%) and none of the non-poppyfield CMMs (p < 0.001).
Fig. 1 shows an example of the poppyfield sign in a malignant melanoma (Fig. 2). In contrast to basal cell carcinomas, where bleeding and ulceration appeared as larger flat areas of blood, poppyfield bleeding occurs as small ruby squirts of blood dispersed in the visual field. They are not visible when ethanol or water is used as contact fluid, but seem to be dependent on the polar blood to non-polar paraffin or mineral oil interface.
Poppyfield bleeding was not observed in other lesions: none of 17 basal cell carcinomas previously published (1) showed this sign, nor did any of the CMMs with Breslow thickness less than 1 mm.

Fig. 1. Amelanotic malignant melanoma. Dermatoscopy with immersion oil showing ruby droplets of blood designated the “poppyfield sign”. A central gray-blue area and atypical vascular pattern were observed, but no other dermatoscopic signs were present, and without the poppyfield sign the lesion might have been missed. (Dermaphot, Heine Optotechnik) (×10).
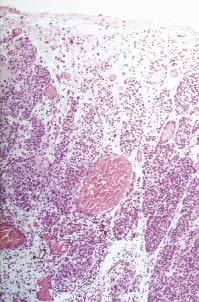
Fig. 2. Malignant melanoma from Fig. 1. Histopathology showing thin-walled dilated capillaries and superficial ulceration. Haematoxylin-eosin; microscopic magnification (×25).
Discussion
Poppyfield bleeding appears in some thick CMMs. Various vascular patterns have been described in dermatoscopy of CMM, and atypical vascular patterns have been associated with thick CMMs (10). The prognostic significance of an atypical vascular pattern has not been independently assessed. However, increasing pathological evidence has accumulated over the past decade that vascular density in primary CMM is higher than in surrounding tissue and in benign melanocytic naevi. Kashani Sabet et al. (11) demonstrated an independent inverse prognostic factor for tumour vascularity on survival and relapse-free interval. The structure of the smooth muscles in the vessel walls in CMM have been found to be more primitive than in benign melanocytic naevi, causing fragility of the vessels, thereby facilitating translocation of malignant cells to the bloodstream and increasing the risk of distant metastases. The poppyfield sign is thought to be a dermatoscopic reflection of this, as data support a causal complex between histopathological ulceration and dilated vessels and dermatoscopic poppyfield bleeding. According to Laplace’s law the transmural pressure of a cylinder is proportional to the wall tension and inversely proportional to the radius of the cylinder. When the dermatoscope is pressed against the skin, the transmural pressure is assumed to increase, eventually leading to abrupt rupture of the outset dilated and fragile vessels, causing the poppyfield sign seen by dermatoscopy.
References
1. Lorentzen H, Weismann K, Sand Petersen C, Grønhøj Larsen F, Skødt V. Clinical and dermatoscopic diagnosis of malignant melanoma – assessed by an expert and non-expert group. Acta Derm Venereol 1999; 79: 301–304.
2. Stolz W, Rieman A, Cognetta AB, Pillet L, Abmayr W, Hölzel D, et al. ABCD rule of dermatoscopy: a new practical method for early recognition of malignant melanoma. Eur J Dermatol 1994; 4: 521–527.
3. Menzies SW, Crotty KA, Ingvar C, McCarthy WH. An atlas of surface microscopy of pigmented skin lesions. 1. John Rowe. Sydney: McGraw-Hill; 1996.
4. Argenziano G, Fabbrocini G, Carli P, De GV, Sammarco E, Delfino M. Epiluminescence microscopy for the diagnosis of doubtful melanocytic skin lesions. Comparison of the ABCD rule of dermatoscopy and a new 7-point checklist based on pattern analysis. Arch Dermatol 1998; 134: 1563–1570.
5. Lorentzen HF, Weismann K. [Dermatoscopic diagnosis of cutaneous malignant melanoma. Secondary prophylaxis]. Ugeskr Laeger 2000; 162: 3312–3316. In Danish.
6. Bafounta ML, Beauchet A, Aegerter P, Saiag P. Is dermoscopy (epiluminescence microscopy) useful for the diagnosis of melanoma? Results of a meta-analysis using techniques adapted to the evaluation of diagnostic tests. Arch Dermatol 2001; 137: 1343–1350.
7. Kittler H, Pehamberger H, Wolff K, Binder M. Diagnostic accuracy of dermoscopy. Lancet Oncol 2002; 3: 159–165.
8. Kahn HJ, Baumal R, Marks A. The value of immunohistochemical studies using antibody to S100 protein in dermatopathology. Int J Dermatol 1984; 23: 38–44.
9. Wick MR, Swanson PE, Rocamora A. Recognition of malignant melanoma by monoclonal antibody HMB-45. An immunohistochemical study of 200 paraffin-embedded cutaneous tumours. J Cutan Pathol 1988; 15: 201–207.
10. Argenziano G, Fabbrocini G, Carli P, De Giorgi V, Delfino M. Clinical and dermatoscopic criteria for the preoperative evaluation of cutaneous melanoma thickness. J Am Acad Dermatol 1999; 40: 61–68.
11. Kashani Sabet M, Sagebiel RW, Ferreira CM, Nosrati M, Miller JR. Tumor vascularity in the prognostic assessment of primary cutaneous melanoma. J Clin Oncol 2002; 20: 1826–1831.

