


Nicoletta Cassano and Gino A. Vena*
2nd Dermatology Clinic, Department of Internal Medicine, Immunology and Infectious Diseases, University of Bari, 70124, Bari, Italy. *E-mail: g.vena@dermatologia.uniba.it
Accepted September 11, 2006.
1This study was presented as a poster at the 1st World Psoriasis & Psoriatic Arthritis Conference 2006, Stockholm 31 May–4 June 2006.
Sir,
We read with interest the article of Dr Downs reporting the fast and good response of scalp psoriasis to a two-compound ointment containing 0.5 mg/g betamethasone dipropionate and 50 µ/g calcipotriol (Dovobet ointment) (1). We report here the results of a 12-week open-labelled study that aimed to evaluate the efficacy and tolerability of treatment with Dovobet ointment followed by a maintenance treatment with calcipotriol solution in scalp psoriasis.
MATERIALS AND METHODS
Twenty-five patients (17 men, 8 women; age range 20–74 years; mean age 45.5 years) entered the study, after giving written informed consent. They presented with scalp psoriasis alone or associated with stable localized lesions of plaque psoriasis that were adequately controlled by topical therapies. Patients were asked to avoid treatments that interfered with study evaluations (including medicated shampoos). Topical treatments for scalp psoriasis and standard systemic therapies were to be stopped for at least 2 and 4 weeks, respectively, prior to study entry.
Study treatment consisted of three sequential phases: (i) application of Dovobet ointment to the affected scalp areas once daily (qid) for 2 weeks; (ii) treatment with Dovobet ointment qid and calcipotriol 0.005% solution twice daily on alternate days for 4 weeks; (iii) treatment with calcipotriol solution twice daily for 6 weeks. Patients were instructed to apply the two-compound ointment at bedtime and to wear a bathing cap overnight, shampooing their hair in the morning of the following day.
Clinical evaluation was performed at baseline and after 2, 6 and 12 weeks. Signs of scalp psoriasis (erythema, scaliness, thickness) were scored using a 5-point scale (0 = absent; 1 = mild; 2 = moderate; 3 = severe; 4 = very severe). The same scale was used by patients for the assessment of severity of pruritus. Clinical total score corresponded to the sum of the single scores. Wilcoxon signed-rank sum test was used to compare clinical scores at week 2, week 6 and week 12 with baseline scores (statistical significance for p < 0.05).
At week 12, patients assessed both the efficacy and cosmetic acceptability of the treatment regimen using a 4-point scale from poor to excellent.
RESULTS
All patients completed the study as scheduled. At baseline, mean total score was 8.3. A significant improvement of signs and symptoms was observed at week 2 (total score: 3.5), at week 6 (total score: 2.6) and week 12 (total score: 3.2) (p < 0.05 for each evaluation) (Fig. 1).
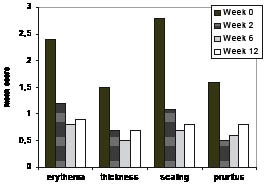
Fig. 1. Change of severity of signs and symptoms during the study period (n = 25).
Treatment was well tolerated. Only 2 patients complained of transient and mild burning sensation (one with the combined treatment with two-compound product and calcipotriol solution, the other during monotherapy with calcipotriol solution).
The efficacy of the treatment regimen was judged as good or excellent by 75% of patients (Table I). Acceptability was considered good or excellent by only 40% of patients. Reasons for poor or moderate acceptability were primarily linked to the ointment formulation of the two-compound product (greasiness, difficult application, necessity of washing).
Table I. Patients’ assessment of efficacy and cosmetic acceptability of treatment (n = 25)
| Efficacy n (%) | Acceptability n (%) | |
| Poor | 2 (8) | 9 (36) |
| Moderate | 4 (16) | 6 (24) |
| Good | 12 (48) | 7 (28) |
| Excellent | 7 (28) | 3 (12) |
DISCUSSION
The results of this pilot study show the good response of scalp psoriasis to the calcipotriol/betamethasone dipropionate two-compound product in agreement with the report previously published by Downs (1). The two-compound product provided prompt relief of both signs and symptoms, and the therapeutic effect was maintained for up to 12 weeks by a combined / sequential treatment with calcipotriol 0.005% solution.
The choice of our therapeutic scheme was influenced by the original regimen proposed by Koo (2) for scalp psoriasis, consisting of an initial 2-week treatment with clobetasol, which was tapered off and combined with calcipotriol in a 2-week transitional phase, followed by maintenance on calcipotriol alone.
A remarkable finding was the rapid improvement in pruritus induced by Dovobet. Pruritus is a symptom frequently associated with psoriasis (3, 4), although it is usually underestimated. The marked and prompt control of pruritus may be particularly useful for increasing patient's compliance with treatment and preventing the exacerbation of lesions due to scratching (5). A questionnaire-based survey of 1023 patients showed that scalp psoriasis is psychologically and socially distressing, with itch and scaling as the most relevant sources of distress (6).
The results obtained in our study also confirm the need for a cosmetically more acceptable formulation of Dovobet for scalp psoriasis (1).
Conflict of interest: None reported.
REFERENCES
1. Downs AMR. Dovobet® ointment under occlusion overnight for troublesome scalp psoriasis. Acta Derm Venereol 2006; 86: 57–58.
2. Koo J. Vitamin D and scalp psoriasis. Cutis 2002; 70 Suppl 5: 21–24.
3. Yosipovitch G, Goon A, Wee J, Chan YH, Goh CL. The prevalence and clinical characteristics of pruritus among patients with extensive psoriasis. Br J Dermatol 2000; 143: 969–973.
4. Sampogna F, Gisondi P, Melchi CF, Amerio P, Girolomoni G, Abeni D; IDI multipurpose psoriasis research on vital experiences investigators. Prevalence of symptoms experienced by patients with different clinical types of psoriasis. Br J Dermatol 2004; 151: 594–599.
5. Cassano N, Miracapillo A, Coviello C, Loconsole F, Bellino M, Vena GA. Treatment of psoriasis vulgaris with the two-compound product calcipotriol/betamethasone dipropionate followed by different formulations of calcipotriol. Clin Drug Invest 2006; 26: 227–233.
6. van de Kerkhof PC, de Hoop D, de Korte J, Kuipers MV. Scalp psoriasis, clinical presentations and therapeutic management. Dermatology 1998; 197: 326–334.

