


Sari Suomela1, Kati Kainu2, Päivi Onkamo3, Inkeri Tiala2, Johan Himberg4, Lotta Koskinen2,5, Erna Snellman6, Seija-Liisa Karvonen1, Jaakko Karvonen7, Tutta Uurasmaa8, Timo Reunala9, Kristiina Kivekäs7, Christer Jansen8, Päivi Holopainen2, Outi Elomaa2, Juha Kere2,10 and Ulpu Saarialho-Kere1,10,11
1Department of Dermatology, Helsinki University Central Hospital, 2Department of Medical Genetics, 3Division of Genetics, Department of Biological and Environmental Sciences, University of Helsinki, Helsinki, 4Laboratory of Computer and Information Science (CIS), Helsinki University of Technology, Espoo, 5Department of Tissue Typing and Research Laboratory, Finnish Red Cross Blood Service, Helsinki, Finland, Departments of Dermatology, 6Central Hospital of Päijät-Häme, Lahti, 7Oulu University Central Hospital, Oulu, 8Turku University Central Hospital, Turku, 9Tampere University Central Hospital, Tampere, Finland, 10Department of Biosciences and Nutrition, and Clinical Research Centre, Karolinska Institutet, Huddinge, and 11Department of Dermatology, Karolinska Institutet at Stockholm Söder Hospital, Stockholm, Sweden
The PSORS1 locus is the consistently replicated genetic risk factor for psoriasis. Clinical associations with the main marker allele of PSORS1, HLA-Cw6, have been addressed in a number of studies, but clinical associations have not been used as a way to distinguish the effects of the neighbouring candidate genes in PSORS1. Our results show that HLA-Cw6 and CCHCR1 risk allele associations with clinical features of psoriasis are predictably highly similar in a Finnish nationwide cohort of 379 psoriasis patients. The clinical profiling of a small group of patients (n = 34) who were HLA-Cw6– but CCHCR1*WWCC positive suggested that no great differences existed between them and HCR–Cw6– patients. HCR+ genotype (as well as Cw6+ genotype) correlated for the first time positively with female sex and, in contrast with previous studies, negatively with disease severity. Presence of psoriatic arthritis was more pronounced in HCR– psoriasis (as well as in Cw6– psoriasis). Clinical profiling may be a useful approach to distinguishing genetic effects of candidate genes even within a locus in sufficiently large cohorts. Key words: HLA-C antigens; psoriatic arthritis; guttate psoriasis; nail; anti-psoriatic drugs.
(Accepted August 29, 2006.)
Acta Derm Venereol 2007; 87: 127–134.
Ulpu Saarialho-Kere, Department of Dermatology, Helsinki University Central Hospital, Meilahdentie 2, FI-00250 Helsinki, Finland. E-mail: ulpu.saarialho-kere@helsinki.fi
A strong genetic component associates with psoriasis, which is a common chronic skin disorder affecting 2% of Caucasians, males and females equally (1, 2). The overall clinical course of psoriasis may be highly variable: the symptoms may worsen, wane, and occasionally go into spontaneous remission. The sudden, generalized appearance of small, red, scaly lesions is typical for guttate psoriasis, which is the most frequent disease form in children and young adults. Later in life, approximately 70% of these patients develop the chronic plaque form (psoriasis vulgaris), which is the psoriasis subtype affecting 90% of patients (1, 3). Chronic plaque patients may also present with guttate flares. In severe forms, the entire skin becomes inflamed, leading to erythrodermic psoriasis, or generalized sterile pustules arise, leading to pustular psoriasis. About 5–20% of psoriatic patients develop psoriatic arthritis (PsA), a seronegative spondylarthropathy, which often improves with cutaneous improvement. Arthritis is associated more commonly with nail changes, including pitting, discoloration, subungual hyperkeratosis and onycholysis (4).
Cutaneous trauma can cause the development of a psoriatic plaque in about 40% of psoriatic patients (Koebner’s phenomenon) (5). In addition, psychological stress and several drugs, alcohol and cigarette smoking, as well as bacterial, viral and yeast infections may exacerbate or trigger psoriasis (6–9). In particular, group A beta-haemolytic streptococcal infections are associated with acute guttate psoriasis and exacerbation of chronic plaque psoriasis (10, 11). T-cell-mediated immunity is considered to be the key element in the disease process, but the exact pathogenesis remains unknown (12, 13).
Several candidate genes exist on the basis of either their location in the genome (PSORS1-9) or their putative role in the pathophysiology of psoriatic lesions. We have focused on a positional candidate gene, CCHCR1 (earlier HCR, alpha-Helical Coiled-coil Rod homologue or C6ORF18), which is one of the eight genes in the most important psoriasis susceptibility locus, PSORS1 on chromosome 6p21.3. In previous studies, we and others have shown that HCR is highly polymorphic and has a psoriasis-associated allele (HCR*WWCC) in different populations (14–16). The predicted structure of the risk allele of HCR protein differs from the wild-type allele, affecting possibly also the antigenic properties of the protein (15). We have previously shown that HCR protein is differently expressed in lesional psoriatic skin compared with normal skin (15) and staining for the cell proliferation marker Ki67 shows negative correlation with HCR staining, suggesting that HCR has a role in keratinocyte proliferation (15). A regulatory role for CCHCR1 in transcription factor binding has been discovered recently (17). HCR transgenic mice having either the human non-risk HCR allele or the psoriasis risk allele showed altered cutaneous expression profiles for several proteins known to be upregulated in human psoriasis, such as keratins 6, 16, and 17, tenascin C, and certain SPRRs and matrix metalloproteinases (18). All these findings make HCR a plausible candidate gene for psoriasis susceptibility.
The purpose of this study was to investigate whether the clinical phenotype shows a different profile in subjects stratified according to the presence or absence of risk allele at nearby genes within PSORS1. Specifically, we addressed the clinical profiles of HLA-Cw6 and CCHCR1*WWCC. We analysed the psoriatic phenotype in type I psoriatic patients (19) identified in the course of our psoriasis gene study (15). Our results suggest that, at least in this population, female psoriatic patients in Finland tend to be HCR+ more often than men and HCR+ disease seems to correlate negatively with severity of the disease and positively with puberty as a trigger. Psoriatic arthritis was associated with the HCR– genotype, especially in men, and correlated more often with nail disease.
MATERIALS AND METHODS
Subjects
Between 1999 and 2001, 399 psoriatic patients (282 probands, 117 family members) were recruited from Helsinki, Turku, Tampere, and Oulu University Central Hospitals and Central Hospital of Päijät-Häme, Lahti, Finland, for a genetic study (15). Of these, 379 had psoriasis onset before or at 40 years of age (type I psoriasis) and were included in the present study. The subgroup of probands was analysed separately, but due to similar findings, only the results comprising the whole group of type I psoriatic patients are reported here. Familial psoriatic patients (n = 172, 45.4%) were affected offspring-parent pairs (n = 46), affected sibling pairs (n = 30) or belonged to large multiplex families (n = 84) and 12 patients had another psoriatic patient distantly related. A slight majority of the patients (n = 216, 57.8%) were men (Table I). The diagnosis of psoriasis was established by physical examination by a dermatologist, with the following inclusion criteria: (i) onset of psoriasis before the age of 40 years; (ii) at least two typical psoriasis plaques present when the patient was examined and interviewed. Patients who had pustulosis palmoplantaris, lesions only on scalp, or uncertain diagnosis were excluded. All participants donated a blood sample. The clinical assessment was carried out and recorded before patients were genotyped for HCR and HLA-C susceptibility alleles. Psoriatic arthritis was recorded positive if it had been diagnosed by a rheumatologist earlier; mere joint complaints were not recorded. Psoriasis Area and Severity Index (PASI) was calculated at the time of investigation according to the rules proposed by Fredriksson & Pettersson (20). The dermatologist also recorded if the patient had “mild” (= treated with ointments, only few contacts with healthcare system), “moderate” (= treated also with ultraviolet (UV) therapies, frequently as an outpatient), or “severe” (= systemic medications, inpatient periods) psoriasis. With a detailed questionnaire and careful physical examination, age, body mass index (BMI), age at onset, triggers at onset (infection, stress, trauma, medication), familiar prevalence, nail changes, face and scalp manifestations, pustular manifestations, hospital admissions (as an inpatient or an outpatient), various UV-therapies, systemic medications, and other illnesses were recorded. The study protocol was approved by the ethics committees of Helsinki, Turku, Tampere, and Oulu University Central Hospitals and Central Hospital of Päijät-Häme and followed the Declaration of Helsinki Guidelines.
Additional query
To further enrich the information obtained in the original genetic study, a questionnaire targeted specifically at tobacco smoking at the time of onset, blood sugar and lipid levels, puberty as a contributing factor, possible favourable effect of sunlight or UV therapy and usage of anti-psoriatic systemic medications, was designed and sent to patients from Helsinki and Päijät-Häme districts. In total, 170 psoriatic patients answered.
Genotyping
DNA was extracted from venous blood samples using a standard non-enzymatic method. HCR susceptibility allele was determined by genotyping two SNPs in the HCR gene, HCR–325 (rs130076) and HCR–1723 (rs130079) using polymerase chain reaction (PCR) amplification and altered restriction sites for AvaII and MsII, respectively, as described previously (15). HCR+ patients were defined as those having the alleles HCR-325*T and HCR-1723–*T, and HCR– all the other allele combinations (CG, CT, TG, respectively). Based on our previous results, HCR-325*T and HCR–1723*T are in strong linkage disequilibrium with each other and with the other two SNPs comprising the psoriasis susceptibility haplotype HCR*WWCC (18). HLA-Cw*6 allele was genotyped using SSP-PCR (21).
Statistical analysis
Binary and categorical traits were compared between the sexes and risk allele carriers vs. non-carriers by χ2 test and by Fisher’s exact test, when the asymptotical properties for the χ2test were not appropriate.
One-way ANOVA with post hoc tests accompanied by adjusted p-values for normal traits and Mann-Whitney U test for non-normal traits were used to make the between-group-comparisons of continuous variables.
Logistic regression was used for controlling for confounding effects of binary phenotypes, such as differing sex ratio in the risk allele carrier groups. For rare traits, odd’s ratios with 95% confidence intervals (CI) were estimated. Because of the exploratory nature of the study, correction for multiple testing was only applied in the post hoc tests. All statistical analyses were done with the SPSS statistical package.
To create an overall picture of the differences of averages of the continuous variables and occurrence frequencies of categorical variables in genotype classes HCR+Cw6+, HCR+Cw6–, and HCR–Cw6–, a profile of the differences was drawn. Here, the significance was tested by a parameter-free permutation test procedure (22). The number of random permutations was 1000 and the significance threshold was set at p = 0.05.
RESULTS
HCR risk allele positive vs. HCR risk allele negative patients
The majority (62.3%) of patients were HCR risk allele positive (HCR+) (Table I). When psoriatic arthritis patients were excluded, the numbers of HCR+ and Cw6+ patients were even more pronounced: of the 309 patients, 66.3% were HCR+ and 57.4% (159/277) Cw6+. For comparison, only 9% of the normal population is Cw6+ and 19% HCR+, as documented previously (14). A positive family history was more common in the HCR+ group (54.5%), while in the HCR– group, 69.2% were sporadic cases (p < 0.001) (Fig. 1). The median age at onset was lower (18 years, range 0–40 years) in the HCR+ group compared with 25 years (range 1–40 years) in the HCR– group (p < 0.001) (Table II). Consequently, the HCR+ disease had lasted longer (24 vs. 20 years, p < 0.003) when the median age did not differ between these two groups (Table II). Patients in the HCR+ group were reported to have had an infection as a trigger at onset more often than HCR–, and usually the infection was acute β-haemolytic streptococcal throat infection (p < 0.025 and p < 0.046, respectively). Psychological stress was more pronounced as a trigger at onset in HCR– patients (p < 0.025). Trauma was reported to be a trigger in 11% of cases in both groups. HCR– patients presented with nail changes more often than HCR+ patients (p < 0.001) (Fig. 1).
Table I. Epidemiological factors and other characteristics for type I psoriatic patients
| Total | Males | Females | Psoriatic arthritis | Only skin lesions | |
| n | 379 | 219 | 160 | 66 | 309 |
| HCR+ (%) | 62.3 | 54.8 | 72.5 | 43.9 | 66.3 |
| Cw6+ (%) | 53.8 (n = 338) | 43.6 (n = 195) | 67.8 (n = 143) | 35.6 (n = 59) | 57.4 (n = 277) |
| Male/Female (%) | 57.8 /42.2 | – | – | 66.7 /33.3 | 56/44 |
| Median age (range), years | 46 (5–81) | 47 (5–77) | 45 (9–81) | 49 (5–74) | 45 (9–80) |
| Median age at onset (range), years | 20 (0–40) | 24 (1–40) | 16 (0–40) | 24 (1–40) | 20 (0–40) |
| Median duration (range), years | 22 (1–68) | 22 (1–56) | 23 (1–68) | 26 (3–58) | 22 (1–68) |
| Median PASI (range) | 4.0 (0–32.0) | 4.3 (0.4–32.0) | 3.3 (0–24.3) | 5.8 (0.4–29.1) | 3.6 (0–32.0) |
| Median BMI (range) | 25.98 (15–47) | 26.26 (15–41) | 25.25 (18–47) | 25.94 (18–47) | 26.07 (15–41) |
| Positive family history (%) | 45.5 | 39.0 | 54.4 | 33.3 | 48.1 |
| Infection/tonsillitis/stress/trauma as a trigger (%) | 22.2/18.2/31.9/11.1 | 16.4/11.7/35.2/11.9 | 30.0/27.4/27.5/10.0 | 19.7/16.7/28.8/12.1 | 23.0/18.7/32.7/11.0 |
| Psoriatic arthritis (%) | 17.6 | 20.3 | 13.9 | 100 | – |
| Nail changes (%) | 64.9 | 72.6 | 54.5 | 89.4 | 59.6 |
| ”severe”/”mild” disease (%) | 18.2/33.0 | 20.5/28.8 | 15.0/38.8 | 40.9/15.2 | 13.3/37.2 |
| Sought for medical advice (%) | 66.9 | 70.2 | 62.5 | 88.5 | 62.3 |
| Inpatient (%) | 21.1 | 24.3 | 16.7 | 46.8 | 15.5 |
| Anti-psoriatic drugs (%) | 40.4 | 46.6 | 32.0 | 75.4 | 32.2 |
| Erythrodermic/pustular form (%) | 2.5/6.3 | 3.3/6.4 | 1.3/6.3 | 4.9/9.1 | 2.0/5.8 |
| Plaque/solely plaque lesions (%) | 86.3/60.7 | 88.7/64.2 | 82.9/55.9 | 91.8/34.4 | 84.9/59.9 |
| Guttate/solely guttate lesions (%) | 27.2/8.8 | 22.2/7.1 | 34.2/11.2 | 18/1.6 | 28.8/10.4 |
| Scalp/facial lesions (%) | 92.2/58.7 | 93.0/56.9 | 91.1/61.3 | 93.8/61.5 | 92.1/58.6 |
| Asthma and allergy symptoms (%) | 8.7 | 8.3 | 9.4 | 10.6 | 8.2 |
| High blood pressure (%) | 15.6 | 17.4 | 13.1 | 16.7 | 15.2 |
PASI: psoriasis area and severity index; BMI: body mass index
HCR positivity associated with lower PASI values (p < 0.002) (Table II). In addition, all PASI scores over 20 (n = 9) were reported in the HCR– group. Anti-psoriatic systemic drugs had been used as a treatment in 33.6% of cases in HCR+ patients compared with 51.9% of HCR– patients (p < 0.001) (Fig. 1). During the last 5 years, the proportion of those who had no contacts with the healthcare system due to psoriasis was 38.6% in the HCR+ group and 23.7% in the HCR– group (p < 0.002) (Fig. 1). When classified into mean disease severity subgroups “severe”/”moderate”/”mild”, 14.4% of HCR+ psoriatic patients were ranked as having severe psoriasis compared with 24.5% of HCR– psoriatic patients, and 36.4% of the HCR+ were reported to have mild psoriasis compared with 27.3% of the HCR– group (p < 0.05). Moreover, the proportion of those who had been hospitalized, was 17.8% in the HCR+ group and 26.7% in the HCR– group (p < 0.045). UV treatments had been administered just as often in HCR+ as in HCR– groups, but according to query results, UV therapy proved to be more beneficial in HCR+ patients (94% vs. 82%, p < 0.025). Only 6/223 of the HCR+ patients had ever had the pustular form of psoriasis, compared with 18/127 of HCR– patients (p < 0.001) (Fig. 1), and 2/225 of HCR+ cases had erythrodermic psoriasis at the time of investigation compared with 7/137 of HCR– cases (p < 0.03), further stressing the more severe nature of HCR– psoriasis. The results persist after taking confounding factors (different sex ratio) into account (data not shown).
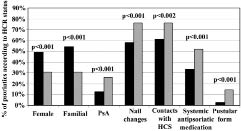
Fig. 1. Clinical characteristics according to HCR genotype. Female gender and positive family history were more frequently encountered in HCR+ patients (). Male gender, psoriatic arthritis (PsA), nail changes, contacts with healthcare system (HCS), usage of systemic anti-psoriatic drugs, and pustular disease form were more common in the HCR– group ().
At the time of investigation, no significant differences were observed in the presence of plaque-type lesions in HCR– vs. HCR+ groups (84.7% vs. 87.2%), but HCR+ patients had more of the guttate-type lesions (31.7% vs. 19.7%) (p < 0.025, data not shown). When HCR+ and HCR– patients were compared, no statistically significant differences were observed in the number of scalp or facial lesions or presence of pure guttate form.
Puberty was reported to have modified psoriasis symptoms more often in the HCR+ group according to the query (33% vs. 11%, p < 0.01). The BMI was, on average, lower in both HCR+ men and women, as well as PsA and skin psoriasis patients. With pure skin psoriasis, the BMI was over 30 in 13.9% of cases in HCR+ group vs. 20.6% in HCR– group, though the p-value remained non-significant. The age of onset was higher in the obese group (BMI >25.5): 18 vs. 24 years (p < 0.006) and the obese were also older at the time of investigation, 50 vs. 42 years (p < 0.001). Considering the other diseases, reported by the patients, asthma and allergy were more common in the HCR– group: 16% compared with 8% in the HCR+ group (p < 0.05) (data not shown).
Possible genotype-wise differences in susceptibility to rare traits were evaluated by odds ratios (OR). They give relative risk of developing the condition given exposure class, e.g. the risk ratio for developing pustular psoriasis in HCR– compared with the risk for developing pustular psoriasis in HCR+. Erythrodermic psoriasis seemed to be more common in HCR– vs. HCR+; the OR was 5.75 (with CI 1.21–27.27). The same applied to pustular psoriasis: 4.88 (CI 1.99–12.00), and asthma and allergy symptoms (HCR– vs. HCR+): 2.02 (CI 1.05–3.86).
Women vs. men
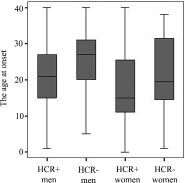
Women were more often HCR+ than men: 72.5% of female psoriatic patients had HCR risk allele compared with 54.8% of men (p < 0.001) (Table I, Fig. 1). Women had earlier disease onset than men (16 vs. 24 years, p < 0.001) and HCR+ women had been younger than HCR– women at the time of onset (15 vs. 20 years; p < 0.03) and HCR+ men even more so (21 vs. 27 years, p < 0.001) (Fig. 2). Of the HCR+ patients, however, 50.2% were men and 49.8% were women (Table II). Many other characteristics that differed significantly in HCR+ vs. HCR– comparison differed also according to sex (Table I). However, most characteristics remained significant in HCR+ vs. HCR– comparisons independently in both sexes.
Both HCR+ men and women had positive family history more frequently than HCR– men and women (men: 46% vs. 33%, p < 0.016; women: 63% vs. 32%, p < 0.001). Nail changes and pustular form were more common in female (69% vs. 49%, p < 0.027; 16% vs. 3%, p < 0.004, respectively) and male (79% vs. 67%, p < 0.049; 11% vs. 3%, p < 0.026, respectively) HCR– groups.
HCR– men had higher PASI values (5.7 vs. 3.6, p < 0.002), more frequent visits to the dermatologist (126 contacts vs. 48 contacts during the last 5 years, p < 0.004), more frequently had psoriatic arthritis (29% vs. 13%, p < 0.005), more frequently used anti-psoriatic drugs (57% vs. 38%, p < 0.007), had asthma or allergy symptoms more often (13% vs. 4%, p < 0.026), and puberty influenced their symptoms less (3% vs. 25%, p < 0.004) than HCR+ men. No significant difference was seen among women in these characteristics, probably because of the low number of HCR– women (n = 44). HCR+ women more often had guttate lesions, and stress less frequently influenced the onset of their psoriasis (44% vs. 21%, p < 0.05; and 45% vs. 24%, p < 0.025, respectively).
Psoriatic arthritis
PsA was diagnosed in 66 patients (17%), who were significantly older than other patients (median age 49 vs. 45 years, p < 0.002). This form of disease was more common in the HCR– group: 26.2% of HCR– patients had been diagnosed with PsA, compared with only 12.4% of HCR+ patients (p < 0.001) (Table I, Fig. 1). Only 33.3% of the psoriatic arthritis patients were women (Table I). Psoriatic arthritis patients also resembled HCR– patients in other characteristics: only 33.3% had another psoriatic patient in the family and they rarely had pure guttate form (1 out of 66 vs. 31 out of 299 skin psoriatic patients, p < 0.04) (Table I). The median PASI score was highest in this subgroup, 5.8 compared with 3.6 in psoriasis confined to skin (p < 0.039), and the patients had had contact with the healthcare system, been inpatients, received systemic anti-psoriatic drugs and PUVA therapy more frequently (p < 0.001 with all these characteristics) compared with skin psoriasis patients (Table I). Dermatologists categorized these patients as having “severe” psoriasis in 40.9% of cases vs. 13.3% with pure skin psoriasis (p < 0.001). Nail changes were reported in 89.4% of cases, equally in HCR+ and HCR– patients (85.7% vs. 91.4%), but clearly more often than in skin psoriasis (59.6%, p < 0.001). Subdividing PsA patients into HCR+ and HCR– groups revealed the HCR– patients to have more often scalp and facial lesions (scalp: 92% vs. 69%, p < 0.047; facial: 76% vs. 43%, p < 0.007) and additionally to have higher PASI values (p < 0.001).
Fig. 2. Age at onset in years according to sex and HCR status. Each box shows the median, quartiles, and extreme values within the sex in relation to HCR status class. The differences between groups were very clear between HCR+ men and HCR– men, the former having an earlier onset (p < 0.002 after correction for post hoc comparisons with Tamhane’s correction). HCR– men also clearly differed from HCR+ women (adjusted p < 0.000 after post hoc comparisons). The other group mean differences did not reach statistical significance after taking correction for post hoc comparisons into account, but gave concordant trends (age at onset is lower in women vs. men, and lower in HCR+ than HCR–).
Comparison between HCR+Cw6+, HCR+Cw6–, and HCR–Cw6– psoriasis
Cw6 status was determined in 338 cases; 53.8% were Cw6+ (57.4% when psoriatic arthritis patients were excluded) (Tables I and II). All Cw6+ cases were also HCR+ (n = 182), but 10% of all patients (n = 34) were HCR+Cw6– (Table II). This offered a valuable point of comparison for the combinations of genotypes. The differences are depicted as averages and occurrence frequencies of the different variables in the groups HCR+Cw6+, HCR+Cw6–, and HCR–Cw6– (Fig. 3). Number of random permutations was 1000 and the significance threshold was set at p = 0.05; thus it is not corrected for overall number of tests made in the study, and should be interpreted with that in mind, as suggestive evidence.
All three groups were similar with respect to age at the time of investigation. HCR–Cw6– patients differed from HCR+Cw6+ patients in the same way as HCR– patients differed from HCR+ patients (Figs 1 and 3; Table II). HCR+Cw6+ patients had significantly less high blood pressure than HCR–Cw6– patients, though, and contacts with the healthcare system did not reach significance in HCR+Cw6+ vs. HCR–Cw6– comparisons. Guttate form and infection and puberty as triggers were significantly related to HCR+Cw6+ genotype and pustular form and stress as a trigger to HCR–Cw6– genotype. Also HCR+Cw6– patients differed from HCR+Cw6+ patients, largely in the same clinical characteristics as HCR–Cw6– patients (Fig. 3). In contrast, presence of PsA (11.7% vs. 14.7%, p = ns), stress and puberty as triggers, presence of erythrodermic or pustular forms, and PASI values did not differ significantly between HCR+Cw6+ and HCR+Cw6- (possibly in part due to low numbers of cases). In addition, HCR+Cw6– patients had most often pure plaque lesions (77%, HCR+Cw6+: 56%, HCR–Cw6–: 67%) and high blood glucose (38%, HCR+Cw6+: 11%, HCR–Cw6–: 22%). In HCR+Cw6– vs. HCR–Cw6– comparison, a significant difference was found only in hospital admissions: inpatients were more frequent in Cw6–HCR– group (p < 0.023).
Table II. Epidemiological factors for different HCR genotypes
| Patients | p-value | Patients | p-value | |||||||
| HCR+ | HCR– | HCR+ vs. HCR– | Cw6+ vs. Cw6– | HCR+Cw6+ | HCR+Cw6– | HCR-Cw6– | HCR+Cw6+ vs. HCR–Cw6- | HCR+Cw6+ vs. HCR+Cw6– | HCR+Cw6- vs. HCR-Cw6– | |
| n | 236 | 143 | p < 0.001 | p < 0.001 | 182 | 34 | 122 | p < 0.001 | p < 0.025 | ns |
| Men/women (%) | 50.8/49.2 | 69.2/30.8 | 46.7/53.3 | 67.6/32.4 | 71.3/28.7 | |||||
| Age, years (range) | 46 (5–81) | 46 (18–76) | ns | ns | 45 (5–81) | 49 (20–73) | 47 (18–76) | ns | ns | ns |
| Age at onset, years (range) | 18 (0–40) | 25 (1–40) | p < 0.001 | p < 0.001 | 16.5 (0–40) | 25 (10–40) | 25 (2–40) | p < 0.001 | p < 0.001 | ns |
| Duration, years (range) | 24 (1–68) | 20 (1–48) | p < 0.003 | p < 0.001 | 27.0 (1–68) | 19.5 (3–43) | 21.0 (1–48) | p < 0.001 | p < 0.049 | ns |
| PASI (range) | 3.5 (0–19.4) | 5.2 (0.2–32) | p < 0.002 | p < 0.007 | 3.5 (0–9.4) | 5.2 (0.8–13.6) | 4.95 (0.6–32) | p < 0.008 | ns | ns |
| BMI (range) | 25.7 (18–39) | 26.7 (15–47) | ns | ns | 25.6 (19–39) | 25.0 (20–38) | 26.7 (15–41) | ns | ns | ns |
| ns : not significant; PASI : psoriasis area and severity index; BMI: body mass index. | ||||||||||
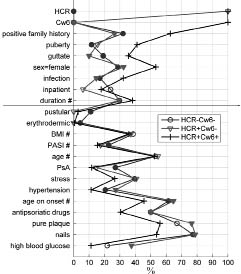
Fig. 3. Average of the attributes in HCR+Cw6+ vs. HCR–Cw6– and HCR+Cw6– The solid marker indicates the significance p < 0.05 between the averages: HCR–Cw6– vs. HCR+Cw6+ (solid circle) and HCR+Cw6– vs. HCR+Cw6+ (solid triangle). Attributes above the line are linked to PSORS1 positivity and under the line to PSORS1 negativity (with the exception of “inpatient”, “BMI”, “age”). For most of the attributes the scale shows directly the relative frequency (%) of the positive cases for the attribute. For continuous variables (#) the values are in relative scale (0% corresponds to the minimum and 100% to the maximum value of the attribute). Significance of the difference between means in groups HCR+Cw6– vs. HCR–Cw6– is not indicated since for these groups only the difference for “inpatient” has p < 0.05.
BMI: body mass index; PASI: psoriasis area and severity index; PsA: psoriatic arthritis.
Cw6+/– psoriasis compared with HCR risk allele+/– in psoriasis patients
PASI levels were reported to be lower in the HCR+ group than the HCR– group. The same was true when comparing Cw6+ and Cw– patients (p < 0.007) (Table II). Cw6+/- results showed significant differences in high blood glucose levels and high blood pressure levels (more in Cw6– psoriasis: 11% vs. 21%, p < 0.025 and 6% vs. 10%, p < 0.01, respectively), and pure plaque lesions associated with Cw6– psoriasis, but no difference was found between HCR+ and HCR– psoriasis in these characteristics.
HCR+/– as well as Cw6+/– differences were significant in pustular psoriasis involvement (less pustular form in positive groups), and involvement of joints (less in positive groups) but in HCR+/– comparison the differences were more profound. On the other hand, in Cw6+/– comparison, the significance was more in parameters of guttate lesions (more in positive group), effect of puberty (more reported in positive group), and infection, especially tonsillitis, as a trigger at onset (more in positive group).
DISCUSSION
Previous studies have proved HLA-Cw6 to be the most highly associated allele in psoriasis: it is found in approximately 40–60% of psoriatic patients. Also, in the current study comprising both familial and sporadic psoriasis cases, 62.3% of attended psoriatic patients were HCR+ and 53.8% Cw6+. Like in other studies, positive family history (8, 19), earlier age at onset (19, 23, 24), longer duration of disease, infection as a trigger (especially throat infection) (8, 23, 24), guttate type lesions (8, 23–25) and HLA-Cw6 were linked together. In this study, these characteristics also associated with HCR positivity. As a new finding, puberty had influenced the symptoms more often in the HCR+ group (as well as in Cw6+ group) than in the HCR– group, especially in men, reflecting either the earlier onset or possible hormonal effects. However, trigger factors represent retrospective and putatively uncertain data and thus those results should be interpreted with caution.
Females have been reported to have an earlier onset than men (19, 23, 26). To our knowledge, this is, however, the first study to show clear over-representation of HCR+ (as well as Cw6+) female psoriatic patients. In fact, only a little more than 25% of female psoriatic patients proved to be HCR–, and the reason for this is unclear. Of the attended patients, men represented the majority. A smaller proportion of men than women (39% vs. 54.4%) had another psoriatic patient in the family. One explanation for this could be that women were more interested in attending if they had psoriasis in the family and as a result, women were more often related than men. In the subgroup of probands (n = 282, 71% of the attended psoriatic patients), women were also more often HCR+ than men (p < 0.001).
The severity of the disease was measured with several parameters: the PASI score, dermatologist’s evaluation, number of admissions to hospital, frequency of systemic medications, and presence of severe forms of psoriasis (pustular/erythrodermic). Due to the genetic nature of the original study protocol, the PASI value was determined at the time of investigation. Many patients (especially the probands, n = 282) had already received therapies by this time, which probably lowered the recorded PASI values. Assuming the impact of therapies would have been the same in both HCR+ and HCR– groups, the possible bias would also have been the same in both groups. The results of HCR– patients having received anti-psoriatic drugs, been hospitalized, having more severe forms of psoriasis and more severe disease from the dermatologist’s point of view, and having contacted the healthcare system more often than HCR+ patients indicated HCR– psoriasis to be more severe in nature than HCR+ psoriasis. The PASI data may be less accurate to compare between patients. It has been shown that HLA-Cw6+ patients have a higher mean disease severity score, at least in a material with high familial penetrance (23). Henseler & Christophers (19) also reported more extensive and frequently recurrent symptoms in a HLA-Cw6+ group. In a study comparing familial and sporadic cases, Stuart et al. (27) found that in familial psoriasis total body surface area (%TBSA) involvement was greater with early onset psoriasis, but in sporadic psoriasis %TBSA was lower when onset was early. This is in agreement with our results for more sporadic male cases. Perhaps the men participated if they had a more severe disease and not because they had psoriasis in the family. A previous study with Finnish patients, however, also suggested less severe disease in HLA-Cw6+ patients (28).
In a recent study by Gudjonsson et al. (29), the lower the age at onset of Cw6+ patients (and, conversely, the higher the age at onset of Cw6– patients), the higher the disease severity score. In our material, we could not confirm this. HCR+ patients had lower PASI values than HCR– patients not depending on the age at onset. By contrast, the highest PASI values were seen in HCR– patients with the lowest age at onset (data not shown).
HCR– patients had more PsA and nail changes than HCR+ patients – also in the subgroup of probands – as seen previously also in HLA-Cw6– patients (23, 24). On the other hand, familial clustering is typical of PsA, and linkage results as well as association studies show HLA region to be a candidate region for PsA (30, 31). The only available genome-wide scan localizes a PsA candidate region to 16q (32).
Many of the HCR– patients reported stress as the trigger of onset. Previously non-guttate psoriasis has been linked to recent life crisis (8, 24). In accordance with this, guttate lesions associated more with HCR+ psoriasis than with HCR– psoriasis. Various mechanisms underlying the possible connection between psoriasis and stress include altered barrier homeostasis and stratum corneum integrity, which can be counter-attacked by topical physiological lipids (cholesterol, ceramides, free fatty acids) (33).
Psoriasis associates with hyperlipidaemia (34), obesity and diabetes mellitus (35). Increased cardiovascular morbidity is typical for severe psoriasis (35, 36). In our study, the average BMI was higher in the HCR– group and in different HCR– subgroups than in HCR+ groups, but the difference was not significant. The mean BMI was, however, over 25 (the upper boundary for normal values) in all groups and the age at onset was higher if the patient was obese at the time of investigation. In addition, hypertension and high blood-glucose levels were reported more frequently in HLA-Cw6– patients.
Psoriasis is a disease with a complex genetic background requiring environmental triggers and complicated by heterogeneity. The PSORS1 region on chromosome 6p21.3 has demonstrated the strongest association with psoriasis in various studies and is therefore believed to contain a major predisposing factor for psoriasis. The HLA-Cw6 allele has shown the strongest association, but whether this allele is “the psoriasis gene” or simply a marker in strong linkage disequilibrium with the true disease gene is not known (37, 38). This epidemiological study shows that HLA-Cw6 and CCHCR1 risk alleles have largely the same clinical associations. As reported for HLA-Cw6+ patients (23, 29), HCR risk allele carriers had lower age of onset, throat infection as a trigger, positive family history, more beneficial response to UV therapy, and more guttate lesions. However, erythrodermic and pustular forms were more common in HCR– patients, agreeing with previous data showing that these subtypes are perhaps not related to PSORS1 (25, 39, 40). HCR and Cw6 generally associate with the same clinical features. However, there still exist type I psoriatic patients who have neither alleles.
ACKNOWLEDGEMENTS
We thank the patients and their families for their participation. We also thank Mrs Riitta Lehtinen for skilful technical assistance. This study was supported by grants from the Academy of Finland (1205704), Sigrid Juselius Foundation, Helsinki University Central Hospital Research Funds (TYH4226), Finska Läkaresällskapet, and The Finnish Dermatological Society.
REFERENCES
1. Lomholt G. Psoriasis: prevalence, spontaneous course, and genetics: a census study on the prevalence of skin diseases on Faroe Islands. Copenhagen: GEC Gad, 1963.
2. Christophers E. Psoriasis – epidemiology and clinical spectrum. Clin Exp Dermatol 2001; 26: 314–320.
3. Williams RC, McKenzie AW, Roger JH, Joysey VC. HL-A antigens in patients with guttate psoriasis. Br J Dermatol 1976; 95: 163–167.
4. Lavaroni G, Kokelj F, Pauluzzi P, Trevisan G. The nails in psoriatic arthritis. Acta Derm Venereol 1994; suppl 186: 113.
5. Raychaudhuri SP, Gross J. A comparative study of pediatric onset psoriasis with adult onset psoriasis. Pediatr Dermatol 2000; 17: 174–178.
6. Poikolainen K, Reunala T, Karvonen J. Smoking, alcohol and life events related to psoriasis among women. Br J Dermatol 1994; 130: 473–477.
7. Tsankov N, Kazandjieva J, Drenovska K. Drugs in exacerbation and provocation of psoriasis. Clin Dermatol 1998; 16: 333–351.
8. Naldi L, Peli L, Parazzini F, Carrel CF; Psoriasis Study Group of the Italian Group for Epidemiological Research in Dermatology. Family history of psoriasis, stressful life events, and recent infectious disease are risk factors for a first episode of acute guttate psoriasis: results of a case-control study. J Am Acad Dermatol 2001; 44: 433–438.
9. Naldi L, Chatenoud L, Linder D, Belloni Fortina A, Peserico A, Virgili AR, et al. Cigarette smoking, body mass index, and stressful life events as risk factors for psoriasis: results from an Italian case-control study. J Invest Dermatol 2005; 125: 61–67.
10. Telfer NR, Chalmers RJ, Whale K, Colman G. The role of streptococcal infection in the initiation of guttate psoriasis. Arch Dermatol 1992; 132: 717–718.
11. Gudjonsson JE, Thorarinsson AM, Sigurgeirsson B, Kristinsson KG, Valdimarsson H. Streptococcal throat infections and exacerbation of chronic plaque psoriasis: a prospective study. Br J Dermatol 2003; 149: 530–534.
12. Krueger JG. The immunologic basis for the treatment of psoriasis with new biologic agents. J Am Acad Dermatol 2002; 46: 1–23.
13. Krueger JG, Bowcock A. Psoriasis pathophysiology: current concepts of pathogenesis. Ann Rheum Dis 2005; 64 suppl 2: ii30–36.
14. Asumalahti K, Laitinen T, Itkonen-Vatjus R, Lokki ML, Suomela S, Snellman E, et al. A candidate gene for psoriasis near HLA-C, HCR (Pg8), is highly polymorphic with a disease-associated susceptibility allele. Hum Mol Genet 2000; 9: 1533–1542.
15. Asumalahti K, Veal C, Laitinen T, Suomela S, Allen M, Elomaa, et al. Coding haplotype analysis supports HCR as the putative susceptibility gene for psoriasis at the MHC PSORS1 locus. Hum Mol Genet 2002; 11: 589–597.
16. Chang YT, Shiao YM, Chin PJ, Liu YL, Chou FC, Wu S, et al. Genetic polymorphisms of the HCR gene and a genomic segment in close proximity to HLA-C are associated with patients with psoriasis in Taiwan. Br J Dermatol 2004; 150: 1104–1111.
17. Corbi N, Bruno T, De Angelis R, Di Padova M, Libri V, Di Certo MG, et al. RNA Polymerase II subunit 3 is retained in the cytoplasm by its interaction with HCR, the psoriasis vulgaris candidate gene product. J Cell Sci 2005; 118: 4253–4260.
18. Elomaa O, Majuri I, Suomela S, Asumalahti K, Jiao H, Mirzaei Z, et al. Transgenic mouse models support HCR as an effector gene in the PSORS1 locus. Hum Mol Genet 2004; 13: 1551–1561.
19. Henseler T, Christophers E. Psoriasis of early and late onset: characterization of two types of psoriasis vulgaris. J Am Acad Dermatol 1985; 13: 450–456.
20. Fredriksson T, Pettersson U. Severe psoriasis – oral therapy with a new retinoid. Dermatologica 1978; 157: 238–244.
21. Tonks S, Marsh SGE, Bunce M, Bodmer JG. Molecular typing for HLA class I using ARMS-PCR: Further development following the 12th International Histocompatibility Workshop. Tissue Antigens 1999; 53: 175–183.
22. Hand D, Mannila H, Smyth P, editors. Principles of data mining. Chapter: Data analysis and Uncertainty, Hypothesis Testing. Cambridge, MA: MIT Press, 2001: pp. 93–139.
23. Gudjonsson JE, Karason A, Antonsdottir AA, Runarsdottir EH, Gulcher JR, Stefansson K, Valdimarsson H. HLA-Cw6-positive and HLA-Cw6-negative patients with psoriasis vulgaris have distinct clinical features. J Invest Dermatol 2002; 118: 362–365.
24. Mallbris L, Larsson P, Bergqvist S, Vingard E, Granath F, Stahle M. Psoriasis phenotype at disease onset: clinical characterization of 400 adult cases. J Invest Dermatol 2005; 124: 499–504.
25. Asumalahti K, Ameen M, Suomela S, Hagforsen E, Michaelsson G, Evans J, et al. Genetic analysis of PSORS1 distinguishes guttate psoriasis and palmoplantar pustulosis. J Invest Dermatol 2003; 120: 627–632.
26. Swanbeck G, Inerot A, Martinsson T, Wahlstrom J, Enerback C, Enlund F, Yhr M. Age at onset and different types of psoriasis. Br J Dermatol 1995; 133: 768–773.
27. Stuart P, Malick F, Nair RP, Henseler T, Lim HW, Jenisch S, et al. Analysis of phenotypic variation in psoriasis as a function of age at onset and family history. Arch Dermatol Res 2002; 294: 207–213.
28. Ikäheimo I, Tiilikainen A, Karvonen J, Silvennoinen-Kassinen S. HLA risk haplotype Cw6,DR7,DQA1*0201 and HLA-Cw6 with reference to the clinical picture of psoriasis vulgaris. Arch Dermatol Res 1996; 288: 363–365.
29. Gudjonsson JE, Karason A, Runarsdottir EH, Antonsdottir AA, Hauksson VB, Jonsson HH, et al. Distinct clinical differences between HLA-Cw*0602 positive and negative psoriasis patients – an analysis of 1019 HLA-C- and HLA-B-typed patients. J Invest Dermatol 2006; 126: 740–745.
30. Al-Heresh AM, Proctor J, Jones SM, Dixey J, Cox B, Welsh K, McHugh N. Tumour necrosis factor-alpha polymorphism and the HLA-Cw*0602 allele in psoriatic arthritis. Rheumatology (Oxford) 2002; 41: 525–530.
31. Gladman DD, Farewell VT, Pellett F, Schentag C, Rahman P. HLA is a candidate region for psoriatic arthritis. Evidence for excessive HLA sharing in sibling pairs. Hum Immunol 2003; 64: 887–889.
32. Karason A, Gudjonsson JE, Upmanyu R, Antonsdottir AA, Hauksson VB, Runasdottir EH, et al. A susceptibility gene for psoriatic arthritis maps to chromosome 16q: evidence for imprinting. Am J Hum Genet 2002; 72: 125–131.
33. Choi EH, Brown BE, Crumrine D, Chang S, Man MQ, Elias PM, Feingold KR. Mechanisms by which psychologic stress alters cutaneous permeability barrier homeostasis and stratum corneum integrity. J Invest Dermatol 2005; 124: 587–595.
34. Rocha-Pereira P, Santos-Silva A, Rebelo I, Figueiredo A, Quintanilha A, Teixeira F. Dislipidemia and oxidative stress in mild and in severe psoriasis as a risk for cardiovascular disease. Clin Chim Acta 2001; 303: 33–39.
35. Henseler T, Christophers E. Disease concomitance in psoriasis. J Am Acad Dermatol 1995; 32: 982–986.
36. Mallbris L, Akre O, Granath F, Yin L, Lindelöf B, Ekbom A, Ståhle-Bäckdahl M. Increased risk for cardiovascular mortality in psoriasis inpatients but not in outpatients. Eur J Epidemiol 2004; 19: 225–230.
37. Veal CD, Capon F, Allen MH, Heath EK, Evans JC, Jones A, et al. Family-based analysis using a dense single-nucleotide polymorphism-based map defines genetic variation at PSORS1, the major psoriasis-susceptibility locus. Am J Hum Genet 2002; 71: 554–564.
38. Holm SJ, Sanchez F, Carlen LM, Mallbris L, Ståhle M, O’Brien KP. HLA-Cw*0602 associates more strongly to psoriasis in the Swedish population than variants of the novel 6p21.3 gene PSORS1C3. Acta Derm Venereol 2005; 85: 2–8.
39. Karvonen J, Tiilikainen A, Lassus A. HL-A antigens in patients with persistent palmoplantar pustulosis and pustular psoriasis. Ann Clin Res 1975; 7: 112–115.
40. Muto M, Ohmura A, Hamamoto Y, Konishi Y, Shiozawa S, Youn JI, et al. Generalized pustular psoriasis: strategy for identification of psoriasis susceptibility gene. Arch Dermatol Res 2003; 295: S60–S62.

