


Noriyuki Misago1, Yasuko Ohtsuka1, Kenji Ishii2 and Yutaka Narisawa1
Division of 1Dermatology, Department of Internal Medicine, and 2Department of General Medicine, Faculty of Medicine, Saga University, Nabeshima 5-1-1, Saga 849-8501, Japan. E-mail: misago@post.saga-med.ac.jp
Accepted September 25, 2006.
Sir,
Annular elastolytic giant cell granuloma (AEGCG) (1) is a rare granulomatous skin disease, characterized by elastolysis, elastophagocytosis, and an abundance of multinucleated giant cells. Actinic granuloma (2) is generally involved in the entity of AEGCG (1), but is localized in chronically sun-exposed and damaged regions, while normally demonstrating solitary or multiple, typical annular lesions with erythematous raised borders, whereas AEGCG includes lesions showing a generalized distribution and involving both covered as well as sun-exposed areas (3). In addition, despite the word “annular”, AEGCG sometimes manifests itself in the form of numerous papules (3–5) and the associated erythematous patches do not always show typical annular lesions (6, 7); however, they rarely show diffuse erythematous patches with no special characteristics or reticular erythema (8–10). We herein report a case of AEGCG who demonstrated a generalized distribution of the lesions, and showed the presence of numerous papules as well as reticular erythema, while also demonstrating a rapid spontaneous regression.
CASE REPORT
A 62-year-old Japanese man presented with a 3-month history of erythematous lesions on his upper extremities and numerous papules on his trunk. He had a history of a gastrectomy due to a gastric ulcer 23 years previously. Examinations revealed diffuse and reticular erythematous plaques symmetrically on both the extensor and flexor aspects of both forearms partially involving the upper arms (Fig. 1A and B). In addition, numerous flesh-coloured to slightly brown, small lichenoid papules, measuring 1−2 mm in diameter, were found symmetrically on both sides of the abdomen extending to the waist and the lateral chest (Fig. 1A and D). These papular lesions were also found on the chest and upper back. Routine laboratory analyses were normal, except for the presence of mild, iron deficiency anaemia. Serum angiotensin converting enzyme was normal and antinuclear antibody was negative. An ophthalmological examination, chest X-ray, and a computed tomography scan of his chest, revealed normal findings, thus ruling out a diagnosis of sarcoidosis. Without any treatment, a complete spontaneous regression of both forms of the lesions was seen within one month (Fig. 1C and E).
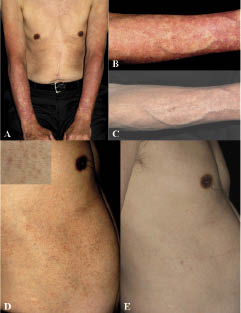
Fig. 1. (A) Diffuse and reticular erythematous plaques symmetrically presenting on the patient’s bilateral forearms partially involving the upper arms; and numerous flesh-coloured to slightly brown, small papules, distributed symmetrically on the abdominal side and the chest wall. (B) The reticular erythematous plaque on the extensor aspect of the right forearm. (C) Complete, spontaneous regression of the reticular erythematous plaque on the right forearm after one month. (D) Numerous flesh-coloured to slightly brown, small, lichenoid papules, distributed on the right abdominal side extending to the waist and the lateral chest. The insert shows a close-up view of the papules. (E) Complete, spontaneous regression of the numerous papules, distributed on the right abdominal side after one month.
Skin biopsies were obtained from the reticular erythema on the forearm and one of numerous papules on the abdominal side. A specimen of reticular erythema revealed a diffuse, band-like or patchy granulomatous infiltration composed of numerous multinucleated giant cells, histiocytes, and lymphocytes in the upper and middle dermis (Fig. 2A). The specimen from a papular lesion showed interstitial infiltration composed of many multinucleated giant cells, histiocytes, and lymphocytes in the upper and middle dermis. Elastophagocytosis by multinucleated giant cells and histiocytes was often seen in both specimens. Moderate solar elastosis was observed in the reticular erythema lesion, whereas no obvious solar elastosis was seen in the papular lesion. There were no features of necrobiosis, palisading granuloma, or mucin deposition in either specimens. Elastica van Gieson’s stain highlighted the elastophagocytosis and the absence or decrease of elastic fibres in the areas neighbouring granulomatous infiltrates in both specimens (Fig. 2B). Multinucleated giant cells and histiocytes were immunohistochemically positive for CD68.
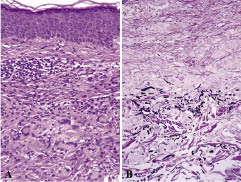
Fig. 2. (A) Histopathology of the reticular erythema, showing a diffuse granulomatous infiltration composed of numerous multinucleated giant cells, histiocytes and lymphocytes in the dermis. (B) Elastica van Gieson’s staining of the reticular erythema specimen highlighting the elastophagocytosis by multinucleated giant cells and histiocytes and a paucity of elastic fibres in the areas neighbouring the granulomatous infiltrates.
DISCUSSION
The relationship between AEGCG and granuloma annulare remains controversial, and an exact distinction of AEGCG from granuloma annulare may be difficult (11). However, recent histopathological studies (10, 12), suggest AEGCG to be a distinct condition, with the following characteristics: (i) absence of mucin and necrobiosis; (ii) predominance of multinucleated giant cells, elastolysis, and elastophagocytosis; and (iii) absence of palisading granuloma, (although sarcoidal granuloma is sometimes present in AEGCG). The histopathological features of the present case therefore favoured a diagnosis of AEGCG rather than granuloma annulare.
The clinical features of AEGCG tend to be quite variable, probably depending on the degree of immune response in individuals or the type of involved elastic tissues (13). When the complete elastophagocytosis by histiocytes to the actinically degenerated elastic tissue advances centrifugally, the lesions localized in sun-exposed areas may show typical annular configuration (2); the incomplete elastophagocytosis by histiocytes without centrifugal expansion may thus result in either erythematous patches with no special characteristics or reticular erythema. When the systemic host response occurs to the mildly actinic-degenerated or intact elastic tissue (3), generalized papular lesions may be seen; obvious solar elastosis was seen in the reticular erythema, but not in the papular lesion in the present case.
Although the lesions of AEGCG tend to resolve gradually over a period of several years (14), the course of the disease is usually chronic with inconstant responses to various treatments (3). A spontaneous remission within one year, as observed in the present case, has been reported in 3 previous cases (1, 9, 15). A complete regression within one month, may suggest that the immune reaction to actinically degenerated or intact elastic tissue in AEGCG could be a transient phenomenon. Nevertheless, this case demonstrated that AEGCG can show various degrees of clinical remission as well as varying clinical manifestations.
REFERENCES
1. O’Brien JP. Actinic granuloma. An annular connective tissue disorder affecting sun- and heat-damaged (elastotic) skin. Arch Dermatol 1975; 111: 460−466.
2. Hanke CW, Bailin PL, Roenigk HH Jr. Annular elastolytic giant cell granuloma. A clinicopathologic study of five cases and a review of similar entities. J Am Acad Dermatol 1979; 1: 413−421.
3. Ozkaya-Bayazit E, Buyukbabani N, Baykal C, Ozturk A, Okcu M, Soyer HP. Annular elastolytic giant cell granuloma: sparing of a burn scar and successful treatment with chloroquine. Br J Dermatol 1999; 140: 525−530.
4. Kato H, Uyeki Y, Yaoita H. Papular lesions associated with annular elastolytic giant cell granuloma. J Am Acad Dermatol 1989; 21: 398−400.
5. Morita K, Okamoto H, Miyachi Y. Papular elastolytic giant cell granuloma: a clinical variant of annular elastolytic giant cell granuloma or generalized granuloma annulare? Eur J Dermatol 1999; 9: 647−649.
6. Sina B, Wood C, Rudo K. Generalized elastophagocytic granuloma. Cutis 1992; 49: 355−357.
7. Pock L, Blazkova J, Caloudova H, Varjassyova I, Konkolova R, Hercogova J. Annular elastolytic giant cell granuloma causes an irreversible disappearance of the elastic fibres. J Eur Acad Dermatol Venereol 2004; 18: 365−368.
8. Mielke V, Weber L, Schunter M, Sterry W. Reticular elastolytic giant cell granuloma. A variant of the annular elastolytic giant cell granuloma. Hautarzt 1995; 46: 259−262.
9. Hermes B, Haas N, Czarnetzki BM. Annular elastolytic giant cell granuloma with a spontaneous healing tendency. Hautarzt 1995; 46: 490−493.
10. Limas C. The spectrum of primary cutaneous elastolytic granulomas and their distinction from granuloma annulare: a clinicopathological analysis. Histopathology 2004; 44: 2772−2782.
11. Ragaz A, Ackerman AB. Is actinic granuloma a specific condition? Am J Dermatopathol 1979; 1: 43−50.
12. Al-Hoqail IA, Al-Ghamdi AM, Martinka M, Crawford RI. Actinic granuloma is a unique and distinct entity: a comparative study with granuloma annulare. Am J Dermatopathol 2002; 24: 209−212.
13. O’Brien JP. Actinic granuloma: the expanding significance. An analysis of its origin in elastotic (“aging”) skin and a definition of necrobiotic (vascular), histiocytic, and sarcoid variants. Int J Dermatol 1985; 24: 473−490.
14. McGrae JD Jr. Actinic granuloma. A clinical, histopathologic, and immunocytochemical study. Arch Dermatol 1986; 122: 43−47.
15. Hohenleutner S, Wlotzke U, Landthaler M, Stolz W. Elastolysis of the mid-dermis and annular elastolytic giant cell granuloma: different stages in the clinical spectrum of dermal elastolysis? Case report and review of the literature. Hautarzt 1997; 48: 45−50.

