


Jung-Wook Kim, Jeong-Hoon Park, Deborah Lee, Seon-Wook Hwang and Sung-Wook Park
Department of Dermatology, Busan Paik Hospital, College of Medicine, Inje University, 633-165, Kaegum-dong, Busanjin-gu, Busan 614-735, Korea. E-mail: der7611@hanmail.net
Accepted November 8, 2006
Sir,
Pyoderma gangrenosum (PG) is a sterile, pustular, ulcerative process of unknown cause (1). It is frequently associated with various systemic diseases, including inflammatory bowel disease, arthritis, monoclonal gammopathy, malignant disease (2) and, rarely, Behçet’s disease (3). Four clinical and histological variants have been recognized: ulcerative, pustular, bullous and vegetative. Vegetative PG is usually not associated with systemic disease (2). We report here a case with vegetative PG in Behçet’s disease.
Case report
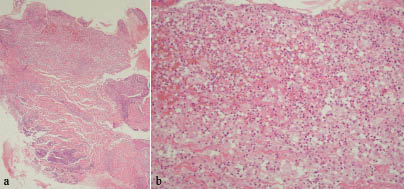
In November 2005, a 75-year-old Korean man presented with painful erythematous plaques on his face and anterior chest, of 4 months’ duration. His medical history included Behçet’s disease with recurrent oral and genital ulcers, arthritis and ocular lesions. He was treated with colchicine, dapsone, sulphasalazine, and prednisolone intermittently for about 2 years. The patient also had chronic pancreatitis that was treated with camostat mesilate. Physical examination revealed erythematous crusted plaques, 1.5 cm diameter, on his right chin and 7–8 cm diameter on his right forehead and anterior chest (Fig. 1). The lesions were initially erythematous plaques or nodules, but evolved to form superficial ulcers. They gradually increased in size and were surrounded by purple borders. The skin lesions concurred with an exacerbation of Behçet’s disease, manifested as vasculitis of the superior mesenteric artery. Laboratory examination revealed anaemia (red blood cells 2.4×106/μl, haematocrit 25.4%) and increased C-reactive protein (2.8 mg/dl). Repeated smears and cultures for bacteria and fungi were negative. An incisional biopsy from the anterior chest showed ulceration, diffuse neutrophilic infiltration with dermal inflammatory infiltrates consisting of epithelioid histiocytes, lymphocytes and multinucleated giant cells. Although vascular reaction was found in the histological sections, frank vasculitis was not observed (Fig. 2). Both periodic acid Schiff (PAS) stain and Gomori’s methenamine-silver (GMS) stain were negative. Based on the clinical and histological findings, our case was diagnosed as vegetative PG occurring during an exacerbation of Behçet’s disease. The lesions improved markedly after systemic corticosteroid therapy (prednisolone 30 mg/day for 2 weeks) and healed with scarring.

Fig. 1. Erythematous and vegetative plaques (a) on the patient’s face and (b) on the anterior chest.
Fig. 2. Incisional biopsy from the lesion showed a diffuse dermal neutrophilic infiltration surrounded by a granulomatous reaction. H&E stain ×40 (a) and ×200 (b).
Discussion
PG, which was first described by Brunsting et al. (4), is a rare, destructive inflammatory skin disease in which a nodule or pustule breaks down to form a progressively enlarging ulcer. Approximately 50% of patients have an associated systemic disease including inflammatory bowel diseases, arthritis, monoclonal gammopathy, or malignant disease (2). Since the first report by Munro & Cox in 1988 (5), 5 cases of PG associated with Behçet’s disease have been reported in the English literature (3, 6–9) (Table I).
Table I. Reported cases of pyoderma gangrenosum with Behçet’s disease
| Author | Age/Sex | Type of PG | Treatment |
| Munro & Cox (5) | 43/F | Pustular and Ulcerative | Thalidomide |
| Lilford et al. (6) | 40/F | Ulcerative | Steroid |
| Rustin et al. (7) | 40/M | Ulcerative | Thalidomide |
| Armas et al. (8) | 52/M | Ulcerative | Steroid |
| Singh et al. (9) | 8/F | Bullous | Not given |
| Nakamura et al. (3) | 16/F | Ulcerative | Total colectomy |
| Present case | 75/M | Vegetative | Steroid |
According to the clinical appearance, the rate of progression, the associated systemic disease and the histopathological changes, PG has been classified into 4 clinical variants: ulcerative, pustular, bullous and vegetative (2). Vegetative PG is a limited, non-aggressive, chronic, superficial and vegetative variant, which is also termed superficial granulomatous pyoderma (1). Unlike classic PG, many patients with vegetative PG do not have an associated systemic disease (10). However, Langan & Powell (11) reported that 18% of patients had other medical conditions, including diabetes mellitus, rheumatoid arthritis, chronic lymphocytic leukaemia, polycythaemia rubra vera, para-proteinemia and pulmonary sarcoidosis.
There is a clinical and histological overlap between PG and Behçet’s disease (3, 5). Pustular lesions can be the initial skin manifestation, and skin hyper-reactivity or pathergy is often found in both diseases. The skin lesions of PG and Behçet’s disease may show a similar range of histological appearances, including a neutrophilic vascular reaction. Therapeutic agents used to treat PG and Behçet’s disease are similar: glucocorticoids, sulpha-drugs and immunosuppressive agents, such as cyclosporine, azathioprine or cyclophosphamide. However, there is a histopathological distinction between PG and Behçet’s disease (12). In PG, vascular involvement ranges from none to fibroid necrosis, and in most cases a neutrophilic infiltrate is present with limited vascular damage. Conversely, in Behçet’s disease, mononuclear cell vasculitis with variable fibrin deposition or leukocytoclastic vasculitis is usually found.
Nakamura et al. (3) reported a patient with PG that improved rapidly after resection of the colon, which was affected by intestinal Behçet’s disease; these authors suggested that the association of PG with Behçet’s disease was highly relevant. In the present case, vegetative PG developed concurrently with an exacerbation of activity of Behçet’s disease. Therefore, this clinical course suggests a close relationship between vegetative PG and Behçet’s disease.
Conflict of interest: None to declare.
References
1. Wolff K, Stingl G. Pyoderma gangrenosum. In: Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, editors Fizpatrick’s dermatology in general medicine, 6th edn, vol. 1. New York: McGraw-Hill, 2003: p. 969–976.
2. Powell FC, Su WP, Perry HO. Pyoderma gangrenosum: classification and management. J Am Acad Dermatol 1996; 34: 395–409.
3. Nakamura T, Yagi H, Kurachi K, Suzuki S, Konno H. Intestinal Behçet’s disease with pyoderma gangrenosum: a case report. World J Gastroenterol 2006; 12: 979–981.
4. Brunsting LA, Goeckerman WH, O’Leary PA. Pyoderma (ecthyma) gangrenosum: clinical and experimental observations in five cases occurring in adults. Arch Dermatol Syph 1930; 22: 655–680.
5. Munro CS, Cox NH. Pyoderma gangrenosum associated with Behçet’s syndrome-response to thalidomide. Clin Exp Dermatol 1988; 13: 408–410.
6. Lilford RJ, Tindall VR, Batchelor AG. Post-surgical pyoderma gangrenosum of the vaginal vault associated with ulcerative colitis and Behçet’s disease: a case report. Eur J Obstet Gynecol Reprod Biol 1989; 31: 93–94.
7. Rustin MH, Gilkes JJ, Robinson TW. Pyoderma gangrenosum associated with Behçet’s disease: treatment with thalidomide. J Am Acad Dermatol 1990; 23: 941–944.
8. Armas JB, Davies J, Davis M, Lovell C, McHugh N. Atypical Behçet’s disease with peripheral erosive arthropathy and pyoderma gangrenosum. Clin Exp Rheumatol 1992; 10: 177–180.
9. Singh G, Sethi A, Okade R, Harish MR. Bullous pyoderma gangrenosum: a presentation of childhood Behçet’s disease. Int J Dermatol 2005; 44: 257–258.
10. Quimby SR, Gibson LE, Winklemann RK. Superficial granulomatous pyoderma: clinicopathologic spectrum. Mayo Clin Proc 1989; 64: 37–43.
11. Langan SM, Powell FC. Vegetative pyoderma gangrenosum: a report of two new cases and a review of the literature. Int J Dermatol 2005; 44: 623–629.
12. Elder D, Elenitsas R, Johnson B Jr., Murphy G. Cutaneous manifestations of nutritional deficiency states and gastrointestinal disease. In: Elder DE, Elenitsas R, Johnson BL, Murphy GF, editors. Lever’s histopathology of the skin. 9th edn. Philadelphia: Lippincott-Williams & Wilkins, 2005: p. 422–426.

