Camilla Hörfelt, Bo Stenquist, Olle Larkö, Jan Faergemann and Ann-Marie Wennberg
Department of Dermatology, Sahlgrenska University Hospital, Göteborg, Sweden



Camilla Hörfelt, Bo Stenquist, Olle Larkö, Jan Faergemann and Ann-Marie Wennberg
Department of Dermatology, Sahlgrenska University Hospital, Göteborg, Sweden
Acne vulgaris does not always respond to conventional therapy. Photodynamic therapy (PDT) has been proposed as a treatment option. The aim of this study was to determine the optimal light dose for effective PDT treatment of acne and to investigate whether PDT reduces sebum excretion and the amount of Propionibacterium acnes. Fifteen patients (9 men, 6 women, age range 16–44 years, mean age 25 years) with mild to severe acne were enrolled in an open, unblinded study. Aminolaevulinic acid cream (20% in Unguentum Merck) was applied on two circular areas 3 h before PDT. The areas of investigation were irradiated with red light (635 nm) from a Waldman PDT 1200 lamp. Ten patients with facial acne were treated with a light dose of 50 J/cm2 on the right cheek and 30 J/cm2 on the left cheek. Five patients with acne on their back were treated either with 50 J/cm2 or with 70 J/cm2. Clinical follow-up was performed for at least 10 weeks. In the patients with facial acne, sebum excretion was determined before PDT and at every follow-up visit. The amount of P. acnes was measured in a skin surface biopsy using a cyano-acrylate polymer to extract the content of the sebaceous follicles. In 9 patients with facial acne the improvement of lesions was the same for the two light doses. According to the patients’ own assessment, 8 improved after PDT (p=0.02). No difference was found between the two doses in patients with acne on the back. Hyperpigmentation was more common at higher doses of light, and pain was experienced more often by the patients when higher doses were used. No significant reduction in P. acnes or sebum excretion was found at any time after PDT. It is concluded that PDT could be an alternative treatment of acne lesions. The lowest possible light dose should be used for minimal side-effects. Other mechanisms of action for PDT than eradication of P. acnes and sebosuppression should be considered. Key words: acne; delta-aminolaevulinic acid; dose-response; photodynamic therapy; Propionibacterium acnes; sebum.
(Accepted December 21, 2006.)
Acta Derm Venereol 2007; 87: 325–329.
Camilla Hörfelt MD, Department of Dermatology, Sahlgrenska Univeristy Hospital, SE-41345 Göteborg, Sweden. E-mail: camilla.s.horfelt@vgregion.se
Acne vulgaris is a common dermatological disorder, affecting approximately 85% of all young people between 12 and 24 years of age (1). There is a significant number of patients who show no clinical response to antibiotic therapy. In addition, the indiscriminate use of antibiotics leads to increased bacterial resistance (2). Oral retinoids are extremely effective in treating severe acne, but there are significant side-effects with this therapy, such as teratogenicity. There is therefore a need for new alternatives in acne treatment.
Phototherapy with visible light has shown a beneficial effect on acne and has the potential to kill bacteria on the skin (3). The porphyrins produced by Propionibacterium acnes are mostly co-proporphyrins and when δ-aminolaevulinic acid (ALA) is applied an enhanced intracellular porphyrin synthesis with higher amount of co-proporphyrins is found (4). ALA is known to be preferentially taken up by the pilosebaceous unit (5) and is metabolized to light-sensitive protoporphyrin IX (PpIX). PpIX is a photosensitizer with excessive production in acne skin, probably due to the presence of the P. acnes. Photo-activation by light at a suitable dose and wavelength for PpIX forms cytotoxic singlet oxygen and free radicals, which causes destruction of cell nuclei, cell membranes and apoptosis.
The objectives of this small unblinded dose-response study using topical photodynamic therapy (ALA-PDT) were: (i) to determine the optimal light dose for effective treatment of acne with minimal side-effects; and (ii) to investigate whether PDT improves acne by injuring the pilosebaceous unit, thereby reducing both sebum excretion and the amount of P. acnes.
METHODS
Patients
This clinical study was performed at the Department of Dermatology, Sahlgrenska University Hospital, Göteborg, Sweden, and was approved by its local ethics committee and conducted in compliance with the protocol and according to good clinical practice. All patients gave their informed consent before enrolment. Fifteen patients (9 men, 6 women, age range 16–44 years, mean age 25 years), with mild to severe acne grade 1–4 according to Pillsbury et al. (6), were enrolled during a 10-month period. The acne lesions were localized to the cheeks (10 patients) or the back (5 patients). Most patients had been treated previously with tetracyclines, but all had finished acne treatment at least 2 months prior to PDT. At baseline, the number of acne lesions was counted within the area to treat with a circular template (10 cm in diameter). Sebum excretion and the amount of P. acnes were also measured and photographs were taken (see below).
Photodynamic treatment
In all 15 patients ALA-cream (20% in Unguentum Merck) was applied on two circular areas using a template so that each area could be located accurately at subsequent visits. The ALA-cream was applied 3 h before PDT and the treatment site was occluded by a Tegaderm® dressing to enhance penetration. A Waldman PDT 1200 lamp (Waldman Medical, Schwenningen, Germany) with a wavelength interval of 600–730 nm, was used for PDT. Both areas of investigation on the back or the cheeks were irradiated with red light at the absorption maximum of 635 nm for PpIX.
Dose-response PDT
Ten patients with acne on their cheeks were treated with a light dose of 50 J/cm2 (intensity 50 mW/cm2) on the right cheek and with 30 J/cm2 on the left cheek. Five patients with acne on their back were treated with a light dose of 50 J/cm2 on one area and on the other with a higher dose of 70 J/cm2. After investigation the treated sites were covered with a light protective dressing for 24 h to minimize the risk of undesired phototoxic reactions.
Clinical evaluation after PDT
The acne scoring (Tables I and II) was re-evaluated after the photodynamic treatment at every follow-up visits. The ten patients with acne on their cheeks were followed up after 1, 2, 3 and 10 weeks. The five patients with acne on their back were in addition followed up after 20 weeks, which was not possible in those with acne on their cheeks because the subsequent summer season made a further check-up irrelevant.
Table I. Characteristics of 10 patients with acne on the cheeks before and after photodynamic therapy (PDT). Clinical acne score (1–4) was graded according to Pillsbury et al. (17)
| Patient no. | Sex/age (years) | Skin typea | Acne score before PDT | Acne score 10 weeks after PDT | |||
| Left | Right | Left (30 J/cm2) | Right (50 J/cm2) | ||||
| 1 | M/17 | III | 3 | 3 | 2 | 2 | |
| 2 | F/21 | III | 1 | 1 | 2 | 1 | |
| 3 | F/30 | II | 2 | 2 | 1 | 1 | |
| 4 | F/22 | IV | 1 | 1 | 1 | 1 | |
| 5 | M/16 | II | 3 | 3 | 1 | 2 | |
| 6 | M/22 | III | 2 | 2 | 1 | 1 | |
| 7b | M/19 | IV | 3 | 3 | NA | NA | |
| 8 | M/44 | II | 2 | 2 | 1 | 1 | |
| 9 | M/16 | III | 3 | 3 | 1 | 2 | |
| 10 | F/27 | II | 3 | 3 | 1 | 2 | |
aFitzpatrick
bPatient number 7 was followed for only 3 weeks after PDT.
NA, not applicable.
Table II. Characteristics of 5 patients with acne on the back. Back 1 and Back 2 represent the skin areas treated with PDT with different light doses.
| Patient no. | Sex/age (years) | Skin typea | Acne score before PDT | Acne score 20 weeks after PDT | |||
| Back 1 | Back 2 | Back 1 (50 J/cm2) | Back 2 (70 J/cm2) | ||||
| 11 | F/30 | II | 2 | 1 | Resolved | Resolved | |
| 12 | F/29 | II | 1 | 1 | Resolved | Resolved | |
| 13b | M/24 | II | 2 | 2 | NA | NA | |
| 14 | M/43 | II | 4 | 4 | 4 | 4 | |
| 15b | M/17 | III | 3 | 3 | NA | NA | |
aFitzpatrick
bPatients number 13 and 15 were not evaluated at 20 weeks after PDT.
NA, not applicable.
All adverse events were recorded and graded as none, mild, moderate or severe. Photographs were also taken at every follow-up. All patients wrote a personal diary in which they assessed the effect of the acne treatment according to the four alternatives: worse, no change, better or resolved.
Sebum measurement of the acne area on the cheeks
Sebum excretion was registered in the ten patients with acne on their cheeks before PDT and at every follow-up visit. The sample was taken from the same spot 3 cm lateral to the alar rim on both cheeks every time. Patients were informed not to wash or use any emollient for 12 h before every visit. A Sebumeter Combi SM810/CM825/PH900 (Courage Khazaka Electronic, Köln, West Germany) was used. The sebum measurement was performed by briefly pressing a plastic film against the skin for 30 s and the sample was then immediately measured photometrically and expressed in µm-1.
Counts of P. acnes in acne area on the right cheek
The amount of P. acnes was measured before PDT and at every follow-up visit, using the method described by Mills & Kligman (7). A skin surface biopsy was taken using a quick-setting cyano-acrylate polymer to extract the content of the sebaceous follicles. A droplet (20 μl) was spread over a glass slide, which was pressed against the skin for 90 s and then peeled off with a rocking movement. The glass slide samples follicular material that contains microcomedones with the anaerobe P. acnes. The samples were taken 5 cm lateral to the alar rim. The right cheek was chosen for sampling because it received the largest dose of irradiation during PDT. Microcomedones within an area of 8 mm in diameter were cut out of the glass slide with a sterile scalpel. The microcomedones were isolated by homogenizing the sample in Triton X-100 and serially diluting in buffered Triton X. The different dilutions, 0.1 ml each, were cultured anaerobically for 7 days on horse blood agar plates and colonies of P. acnes were counted.
Statistical analysis
Statistical analysis was carried out using ANOVA to compare the changes from baseline of acne lesion counts, sebum excretion and P. acnes. The sign test was used to evaluate the effect of PDT from baseline of patients’ assessment of their acne.
Results
Dose-response PDT: clinical evaluation
In those patients with acne on their cheeks, one was lost for follow-up after 3 weeks. In the other 9 patients there was no difference in clinical results between 30 J/cm2 and 50 J/cm2 at the final evaluation (Table I). Eight out of 9 patients were improved in their acne after PDT. All patients noted improvement of “tightening” of the pores. According to the patients’ own evaluation at the last follow-up 8 of 9 subjects thought that their acne had improved after PDT (p=0.02). The clinical result for patient 1 is shown in Fig. 1.

Fig. 1. Right cheek (patient number 1), (a) before photodynamic therapy (PDT) and (b) 10 weeks after PDT at 50 J/cm2.
In the patients with acne on the back, there was no difference in the results between the two doses, 50 J/cm2 and 70 J/cm2, at the final evaluation (Table II). The acne lesions were resolved in two patients at clinical evaluation. In one patient no improvement was found. Two patients were not available for the 20 weeks follow-up; one was lost to follow-up and the other was treated with isotretinoin because of severe acne in other locations. No statistical analysis was carried out in this small group of patients.
Adverse events
All patients with acne on the cheeks had more pain at the higher dose (50 J/cm2). Three out of 10 patients experienced a hyperpigmentation on the cheek with the higher dose (50 J/cm2) and none with the lower dose (30 J/cm2). The hyperpigmentation resolved in all 3 patients after 10 weeks. All other adverse events resolved after 3–10 days in all patients. No bacterial or viral infections were observed. In the patients with acne on the back there was more pain with the higher dose (70 J/cm2). Three out of 5 patients got a hyperpigmentation only when treated with the higher dose.
Sebum excretion and measurement of P. acnes
These investigations were carried out only in the 10 patients with acne on the cheeks. P. acnes measurements were done only on the right cheek (50 J/cm2) and there was no significant reduction in P. acnes after PDT at follow-up 1, 2, 3 or 10 weeks after treatment. Sebum excretion was measured on both cheeks and no significant reduction was seen after PDT on either cheek. (Fig. 2)
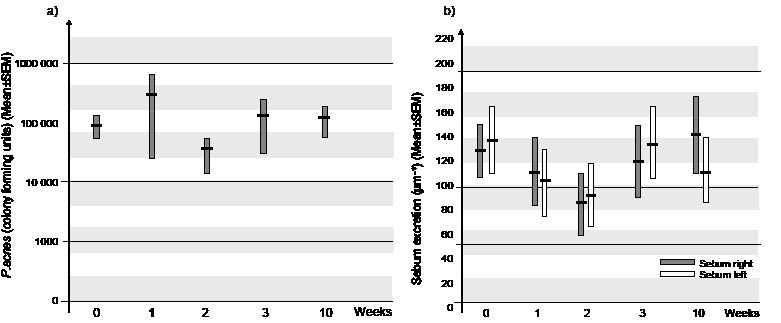
Fig. 2. (a) Changes in numbers of P. acnes during treatment with photodynamic therapy and (b) sebum measurements (µm sebum/cm).
Discussion
ALA-PDT has a specific effect on the pilosebaceous glands, and topical ALA cream is taken up preferentially by the pilosebaceous unit (8); together with the endogenous porphyrins produced by the P. acnes, this will have the potential to improve the acne (9).
This study is a small, un-blinded pilot study. To our knowledge this is the first dose-response study of PDT in acne patients. A dose-response study is important since the dose-response characteristics for ALA-PDT treatment of acne is unknown and probably different from other indications for PDT. We have found that the lower PDT dose had as good an effect as the higher dose on both the cheeks and the back. The optimum dose might in fact be below 30 J/cm2 (30 mW), which was the lowest dose in our study. The side-effects, e.g. pain, erythema and hyperpigmentation, were more frequent with a higher dose and patients with a darker skin type are more easily hyperpigmented with higher doses.
There is a theory that one session of PDT causes reversible damage to the sebaceous glands and multiple sessions are needed to ensure a more permanent effect on the acne lesions. This is supported in the study by Hongcharu et al. (10), using a dose of 150 J/cm2 broad-band light, who have found a reduction in inflammatory acne on the back for 10 weeks after a single treatment of PDT and a reduction in acne lesions for 20 weeks after multiple treatments. In another study of 13 patients with acne on the face, Itoh et al. (11) demonstrated an improvement and reduction in new acne lesions after a single treatment with PDT of 13 J/cm2, which persisted for 3–6 months. The most effective regimen for ALA-PDT on acne lesions would be repeated sessions for a long-term benefit. The question is, are there permanent effects on acne lesions with this therapy or are regular treatments better?
In this study we found a clinical improvement in acne but no reduction in the number of P. acnes or level of sebum excretion after PDT with both doses. Similar findings were obtained by Pollock et al. (12) in their study of 10 patients with acne on their back who were treated weekly for 3 weeks with PDT at a dose of 15 J/cm2. They found a reduction in inflammatory acne lesions after 6 weeks, but no statistically significant reduction in the number of P. acnes or sebum excretion. Other mechanisms of action should be considered, such as effect on infiltrating inflammatory cells around the acne lesion and on the increased expression of toll-like receptor 2 (TLR-2) (13). Another possibility, suggested by Hongcharu et al. (9), is that ALA-PDT reduces follicular obstruction by affecting keratinocyte shedding and hyperkeratosis.
There are various reports of blue light in the treatment of mild to moderate inflammatory acne vulgaris (14–16). The porphyrins produced by the P. acnes have a peak absorption at 415 nm, which is in the blue range of the photodynamic absorption spectrum. However, blue light does not penetrate as deeply into the tissue as red light, due to the shorter wavelength. When blue light is used for PDT, the topical ALA only needs to be applied for 15 min to obtain the full effect (16). It is also known that wavelengths shorter than 600 nm are mainly absorbed by the haemoglobin (17) and this is of importance in the treatment of inflammatory acne.
The side-effects of ALA-PDT, such as erythema, exfoliation and hyperpigmentation, would probably become less problematic if the application time of 3 h for topical ALA cream is reduced. On the other hand, an earlier study (9) indicated the necessity of 3 h application of topical ALA to penetrate deep enough in the tissue to ensure that all sebaceous glands are affected.
The new ALA ester in a cream formulation, methyl-ALA, is more lipid-soluble (18) and will probably increase the uptake in the pilosebaceous gland and the treatment will be more efficacious.
A larger randomized investigator-blinded trial is planned to evaluate the best treatment procedure. The results from our pilot study, however, indicate that the least aggressive ALA-PDT regimen for improving acne is the best. The lowest possible dose should be used, to ensure minimal side-effects, and repeated treatments are necessary for an effective acne treatment. Thus PDT could be an alternative treatment for acne for those with complications after conventional treatments.
ACKNOWLEDGEMENTS
Financial support for this study was obtained from the Sahlgrenska University Hospital. The authors thank biomedical technician Ellinor Mattsson for valuable help with the culture of P. acnes.
Conflicts of interest: Non declared.
References
1. Leyden JJ. A review of the use of combination therapies for the treatment of acne vulgaris. J Am Acad Dermatol 2003; 49: 200–210.
2. Cunliffe WJ. Propionibacterium acnes resistance and its clinical relevance. J Dermatol Treat 1995; 6: 3–4.
3. Zeina B, Greenman J, Purcell WM, Das B. Killing of cutaneous microbial species by photodynamic therapy. Br J Dermatol 2001; 144: 274–278.
4. Ashkenazi H, Malik Z, Harth Y, NitzanY. Eradication of propionibacterium acnes by its endogenic porphyrins after illumination with high intensity blue light. FEMS Immunol Med Microbiol 2003; 35: 17–24.
5. Ibbotson SH. Topical 5-aminolaevulinic acid photodynamic therapy for the treatment of skin conditions other than non-melanoma skin cancer. Br J Dermatol 2002; 146: 178–188.
6. Pillsbury DM, Shelly WB, Kligman A, editors. A manual of cutaneous medicine. Philadelphia: WB Saunders, 1961.
7. Mills OH, Kligman AM. The follicular biopsy. Dermatologica 1983; 167: 57–63.
8. Divaris DXG, Kennedy JC, Poittier RH. Phototoxic damage to sebaceous glands and hair follicles of mice after systemic administration of 5-aminolevulinic acid correlates with localised protoporphyrin IX fluorescence. Am J Pathol 1990; 136: 891–897.
9. Itoh Y, Ninomiya Y, Tajima S, Ishibashi A. Photodynamic therapy for acne vulgaris with topical 5-aminolevulinic acid. Arch Dermatol 2000; 136: 1093–1095.
10. Hongcharu W, Taylor CR, Chang Y, Aghassi D, Suthamjariya K, Andersson RR. Topical ALA-photodynamic therapy for the treatment of acne vulgaris. J Invest Dermatol 2000; 115: 183–192.
11. Itoh Y, Ninomiya Y, Tajima S, Ishibashi A. Photodynamic therapy of acne vulgaris with topical δ-aminolaevulinic acid and incoherent light in Japanese patients. Br J Dermatol 2001; 144: 575–579.
12. Pollock B, Turner D, Stringer MR, Bojar RA, Goulden V, Stables GI, et al. Topical aminolaevulinic acid photodynamic therapy for the treatment of acne vulgaris: a study of clinical efficacy and mechanism. Br J Dermatol 2004; 51: 616–622.
13. Harper JC. An update on the pathogenesis and management of acne vulgaris. J Am Acad Dermatol 2004; 51: 36–38.
14. Cunliffe WJ, Goulden V. Phototherapy and acne vulgaris. Br J Dermatol 2000; 142: 853–856.
15. Goldman MP, Boyce SM. A single-center study of aminolevulinic acid and 417 nm photodynamic therapy in the treatment of moderate to severe acne vulgaris. J Drugs Dermatol 2003; 4: 393–396.
16. Gold MH, Rao J, Goldman MP, Bridges TM, Bradshaw VL, Boring MM, et al. A multicenter clinical evaluation of the treatment of mild to moderate inflammatory acne vulgaris of the face with visible blue light in comparison to topical 1% clindamycin antibiotic solution. J Drugs Dermatol 2005; 4: 64–70.
17. Kalka K, Merck H, Mukhtar H. Photodynamic therapy in dermatology. J Am Acad Dermatol 2000; 42: 389–413.
18. Peng Q, Moan J, Warloe T, Iani V, Steen HB, Bjorseth A, et al. Build-up of esterified aminolevulinic-acid-derivate-induced porphyrin fluorescence in normal mouse skin. J Photochem Photobiol B 1996; 3: 95–96.

