Sir,
Organ transplant recipients under immunosuppressive therapy have a highly increased risk of acquiring unusual opportunistic fungal infections. Therefore, diagnostics for uncharacteristic inflammatory skin lesions in transplant recipients must include an appropriate search for fungi. We recently diagnosed a renal transplant recipient with a cutaneous phaeohyphomycosis due to Alternaria infectoria, and a literature search revealed 3 similar previous reports in dermatological journals (1–3). This low number of observations is probably due to 2 factors: A. infectoria may be disregarded as a supposed contaminant by dermatologists; and strains may be identified with difficulty using conventional methods alone. Appropriate awareness and routinely applied genetic diagnostics may therefore lead to an increase in detection of A. infectoria infections.
CASE REPORT
A 68-year-old renal transplant recipient was referred to our hospital with an unspecific painless and erythematous nodule on the lateral distal dorsal side of his right foot, which had developed within the last 2–3 months and had reached a diameter of approximately 3 cm (Fig. 1). The patient did not recall any preceding injury or trauma at this site. His general health had remained unchanged within the last months. He was under continuous immunosuppressive therapy with tacrolimus (4 mg daily), mycophenolate mofetil (1000 mg daily) and prednisone (5 mg daily). In addition, he was under therapy for hypertension, cardiac insufficiency, hyperlipidaemia and osteoporosis. He used insulin for his diabetes and took phenprocoumon.
Fig. 1. Erythematous nodule on the right foot caused by cutaneous Alternaria infectoria infection. The blue thread marks the site of the biopsy.
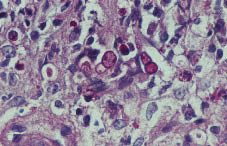
A skin biopsy was taken from the nodule on his foot because some kind of granulomatous reaction was clinically suspected. In this biopsy, multiple thick periodic acid-Schiff-positive unpigmented short hyphal and large thick-walled spherical fungal elements were detected in the dermis within a granulomatous infiltrate of histiocytes, macrophages, giant cells and other inflammatory cells (Fig. 2). Some fungal cells were surrounded by clear spaces. As a consequence of this finding, a chest X-ray and abdominal sonography were performed, but revealed no abnormalities. Furthermore, a second deep skin biopsy was taken from the lesion after meticulous skin surface disinfection for mycological cultures. Immediately after this second biopsy, an oral antimycotic treatment was initiated in consultation with the transplantation centre, starting with 400 mg itraconazole per day. Upon regression of the lesion this was tapered off to 200 mg/day after one week and to 100 mg/day after another 3 weeks in order to reduce interference with the immunosuppressive therapy. Additionally, topical application of ciclopiroxolamine was prescribed. After 2 months of therapy the lesion had healed.
Fig. 2. Dermal skin biopsy taken from the lesion shown in Fig. 1. In the centre there are conspicuous large and thick-walled spherical periodic acid-Schiff-positive fungal elements. Some are surrounded by clear spaces (centre, left side).
Mycology
Dermal tissue obtained from the second biopsy was inoculated on agars free of cycloheximide that were incubated at 26ºC and 37ºC. Fungal growth was observed at 26ºC only. The thalli showed a rapid radial spreading with, initially, some scarce aerial mycelium, but after 14 days the colony surfaces had become glabrous. Dark pigmentation was missing and only very sporadic and rudimentary conidia were obtained. Subsequent DNA analysis at the Centraalbureau voor Schimmelcultures (CBS), The Netherlands, revealed A. infectoria E.G.Simmons. The strain is now deposited in the public CBS collection (CBS no. 120931).
DISCUSSION
Of the saprobic Alternaria species that are potentially able to cause opportunistic cutaneous infections in immunosuppressed organ transplant recipients, A. alternata is seen most commonly (4, 5). However, we found 10 case reports of proven A. infectoria infections in the medical literature accessible via PubMed (1–10) and 4 additional unpublished cases are listed in the CBS database (http://www.cbs.knaw.nl/databases/index.htm). Four cases were published in 2006. A. infectoria was, in fact, observed as an aetiological agent of disease decades ago, but with incorrect species identification (11, 12). The first case published as A. infectoria infection dates back to 1994, involving the nose of a cat (13).
In contrast to strains of A. alternata, clinical isolates of A. infectoria often show only very poor sporulation or are sterile. Production of melanin, which is a helpful clue to recognize dematiaceous moulds, may also be largely absent from A. infectoria cultures (4, 14). Non-sporulating cultures of clinical strains of A. infectoria that lack dark pigmentation interfere with conventional morphological identification and require molecular methods for unambiguous identification (1, 2, 7, 10, 14). It may also be helpful that A. infectoria can release at least 7 unique, and as yet unidentified, metabolites of unknown pathogenetic relevance (15).
Cutaneous infections with A. infectoria usually cause slightly erythematous or bluish, mostly painless and uncharacteristic nodules. The nodules can be single (10) or multiple (1, 4, 5, 7) and can have a sporotrichoid distribution (5). The extremities are most frequently affected (1, 3–8, 10). A. infectoria infections usually remain confined to the skin; in only one case pulmonary involvement was suspected but not proven (4).
Proof of A. infectoria infection relies on the demonstration of the fungus in tissue. In histological preparations, mixed granulomatous dermal infiltrates are seen containing rather large fungal elements. Gnarled elongated and septate hyphal elements and thick-walled chlamydospore-like spherical elements that may be contained in capsules appear to be common features of A. infectoria infections (1, 3–8). The hyaline spherical elements can lead to misdiagnoses of cryptococcosis or blastomycosis (2). For species identification, culture plates free of cycloheximide should be inoculated with unfixed tissue and incubated at approximately 26ºC (not at 37ºC). It is advisable to perform DNA analysis as soon as sufficient material is available.
For treatment, small lesions can be excised completely (6, 10). A reduction in immunosuppressive therapy should be considered (5, 9). In most cases, systemic antimycotic therapy is required. Our positive experience with oral itraconazole is in accordance with some previous reports (1, 2, 5, 7). Amphotericin B was also found to be effective (4, 7) whereas terbinafine proved insufficient in one case (3). Systemic therapies must be coordinated with the responsible transplantation centre, because drug interactions with the immunosuppressive medication require particular attention and long-term clinical follow-up is advisable because of possible relapses (3, 6).
A. infectoria infections are thought to be acquired via direct traumatic inoculation of fungal propagules into the skin (7). A. infectoria is ubiquitous on decaying organic material, particularly on hard and dry substrates such as wheat straw and kernels, and is thus easily introduced into human skin. In our case, A. infectoria elements in contaminated soil or organic material may have been rubbed into the skin under a tightly fitting shoe.
REFERENCES
1. Gerdsen R, Uerlich M, De Hoog GS, Bieber T, Horré R. Sporotrichoid phaeohyphymycosis due to Alternaria infectoria. Br J Dermatol 2001; 145: 484–486.
2. Mayser P, Thoma W, Seibold M, Tintelnot K, Wiedemeyer K, de Hoog GS. Kutane Alternariose. Diagnostik, Klinik und Therapie. Hautarzt 2004; 55: 1137–1142.
3. Ara M, Aspiroz C, Zaballos P, Alcade V, Alvarez R, Rezusta A, et al. Relapse of cutaneous Alternaria infectoria in a renal transplant recipient after 2 years. Acta Derm Venereol 2006; 86: 154–155.
4. Halaby T, Boots H, Vermeulen A, van der Ven A, Beguin H, van Hooff H, et al. Phaeohyphomycosis caused by Alternaria infectoria in a renal transplant recipient. J Clin Microbiol 2001; 39: 1952–1955.
5. Gallelli B, Viviani M, Nebuloni M, Marzano AV, Pozzi C, Messa P, et al. Skin infection due to Alternaria species in kidney allograft recipients: report of a new case and review of the literature. J Nephrol 2006; 19: 668–672.
6. Laumaillé C, Le Gall F, Degeilh B, Guého E, Huerre M. Cutaneous Alternaria infectoria infection after liver transplantation. Ann Pathol 1998; 18: 192–194.
7. Lo Cascio G, Ligozzi M, Maccacaro L, Fontana R. Utility of molecular identification in opportunistic mycotic infections: a case of cutaneous Alternaria infectoria infection in a cardiac transplant recipient. J Clin Microbiol 2004; 42: 5334–5336.
8. Dubois D, Pihet M, Clec´h CL, Croue A, Beguin H, Bouchara JP, et al. Cutaneous phaeohyphomycosis due to Alternaria infectoria. Mycopathologia 2005; 160: 117–123.
9. Vieira R, Veloso J, Afonso A, Rodrigues A. Cutaneous alternariosis in a liver transplant recipient. Rev Iberoam Micol 2006; 23: 107–109.
10. Nulens E, De Laere E, Vandevelde H, Hilbrands LB, Rijs AJMM, Melchers WGJ, et al. Alternaria infectoria phaeohyphomycosis in a renal transplant patient. Med Mycol 2006; 44: 379–382.
11. Wätzig V, Schmidt U. Primäre kutane granulomatöse Alternariose. Hautarzt 1989; 40: 718–720.
12. Svobobová Y, Chmel L, Bojanovská A. Neuer Erreger der Chromomykose festgestellt in der CSSR. Derm Int 1966; 31: 114–115.
13. Roosje PJ, de Hoog GS, Koeman JP, Willemse T. Phaeohyphomycosis in a cat caused by Alternaria infectoria Simmons. Mycoses 1994; 36: 451–454.
14. De Hoog GS, Horré R. Molecular taxonomy of the Alternaria and Ulocladium species from humans and their identification in the routine laboratory. Mycoses 2002; 45: 259–276.
15. Andersen B, Thrane U. Differentiation of Alternaria infectoria and Alternaria alternata based on morphology, metabolite profiles, and cultural characteristics. Can J Microbiol 1996; 42: 685–689.