M. Carmen González-Vela1, J. Fernando Val-Bernal1*, Marcos A. González-López2, Mariona Novell1 and Hector Fernández-Llaca2
1Department of Anatomical Pathology and 2Service of Dermatology Marqués de Valdecilla University Hospital, Medical Faculty, University of Cantabria, Avda. Valdecilla s/n, ES-39008 Santander, Spain. *E-mail: apavbj@humv.es
Accepted May 29, 2007.
Sir,
The coexistence of more than one neoplasm in a single cutaneous specimen is relatively uncommon and has been defined as a collision or compound tumour (1, 2). Although some of these collision tumours may arise from the involvement of related cell types, most occur by chance (1). Melanocytic naevus has been reported as occurring associated with several different tumour types (1, 3). The association of a melanocytic naevus arising contiguously with or adjacent to seborrhoeic keratosis is, however, uncommon (1, 4–7). We report here a patient who presented with a pigmented macule that she had had for a long time, and which had recently increased in size and darkened. Histopathological examination showed a pigmented seborrhoeic keratosis that developed contiguously with a melanocytic naevus.
CASE REPORT
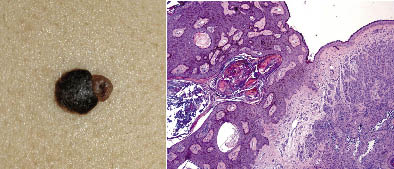
A 39-year-old woman had had a brown, asymptomatic cutaneous lesion on her back since childhood. She reported that the lesion had increased in size and became darker in the last year. Clinical examination disclosed an asymmetric, pigmented tumour measuring 13 mm in diameter on the right scapular region. The lesion exhibited 2 well-differentiated areas of pigmentation: one part was light brown in colour, 4 mm in diameter and the other was black, 9 mm in diameter, with follicular prominence (Fig. 1a). Dermoscopic evaluation of the whole lesion revealed a sharp demarcation, with pseudo-horn cysts, comedo-like openings and fissures in the bigger area. The other part of the tumour showed the presence of a pigmented network with small hypopigmented areas. Clinical and dermoscopic findings suggested a collision tumour: seborrhoeic keratosis and melanocytic naevus. The lesion was surgically excised. Histopathological examination showed a symmetrical intradermal melanocytic proliferation composed of nests of melanocytes without atypia, consistent with a melanocytic intradermal naevus. Adjacent to the melanocytic naevus we observed a proliferation of pigmented small basaloid cells with uniform appearance with hyperkeratosis, acanthosis and pseudohorn cysts (Fig. 1b). The latter features were consistent with pigmented seborrhoeic keratosis.
Fig. 1. (a) Asymmetric pigmented skin tumour composed of one dark-brown plaque 9 mm in diameter and one papular light-brown lesion 4 mm in diameter. (b) Confluence of a seborrhoeic keratosis (left) and an intradermal melanocytic naevus (right).
DISCUSSION
The combination of a melanocytic naevus with other tumours of epidermal or adnexal origin has often been described (1, 3). Common epidermoid cyst and melanocytic nevus is the association reported most frequently (8). Melanocytic naevus has also been associated with a trichilemmal cyst (9), steatocystoma, hidrocystoma and dermoid cyst (8), syringoma (10), trichoepithelioma (3), trichoadenoma (11) and basal cell carcinoma (1).
Despite the fact that melanocytic lesions and seborrhoeic keratosis are among the skin lesions from which biopsies are more commonly taken, the association of a melanocytic naevus with a seborrhoeic keratosis is uncommon. Boyd & Rapini (1), in a retrospective study of 40,000 cutaneous biopsies, found 14 cases of melanocytic naevus juxtaposed with a seborrhoeic keratosis. Only another 4 cases of melanocytic naevus associated with a seborrhoeic keratosis have been reported in the English literature (4–7). The association may either represent the chance of development of 2 common neoplasia together, or may support the theory that there is a pathogenic relationship between seborrhoeic keratosis and melanocytic lesions. We believe that a cutaneous collision tumour usually represents the presence of 2 or more common lesions juxtaposed by coincidence.
In the case described here, due to the clinical history of quick growth of the pigmented lesion adjacent to the melanocytic naevus, we decided to perform a histopathological study of the tumour. Although the lesion seemed to be benign dermatoscopically, it is known that malignant melanoma can mimic a seborrhoeic keratosis (12).
Preoperative diagnosis of cutaneous collision tumours remains extremely difficult in some cases, especially when one of the lesions is melanocytic. Dermatoscopy is a non-invasive technique that may increase diagnostic accuracy in assessing pigmented lesions (13), including cutaneous pigmented collision tumours (14). However, there are dermatoscopic features that can be found in both benign and malignant lesions and in both melanocytic and non-melanocytic lesions (15). In fact, in some cases of cutaneous collision tumours, dermatoscopy does not result in improved diagnostic accuracy, compared with clinical examination (5).
REFERENCES
1. Boyd AS, Rapini RP. Cutaneous collision tumors. An analysis of 69 cases and review of the literature. Am J Dermatopathol 1994; 16: 253–257.
2. Diaz-Cascajo C, Reichel M, Sánchez J. Malignant neoplasms associated with seborrheic keratosis: an analysis of 54 cases. Am J Dermatopathol 1996; 18: 278–282.
3. Brownstein MH, Starink TM. Desmoplastic trichoepithelioma and intradermal nevus: a combined malformation. J Am Acad Dermatol 1987; 17: 489–492.
4. Requena L, Sanchez M, Requena C. Simultaneous occurrence of junctional nevus and seborrheic keratosis. Cutis 1989; 44: 465–466.
5. Wagner RF, Galveston MD Jr. Benign pigmented tumor with combined features of seborrheic keratosis and compound nevus. Cutis 1991; 48: 463–464.
6. de Giorgi V, Massi D, Sestini S, Alfaioli B, Carelli G, Carli P. Cutaneous collision tumour (melanocytic naevus, basal cell carcinoma, seborrhoeic keratosis): a clinical, dermoscopic and pathological case report. Br J Dermatol 2005; 152: 787–790.
7. Betti R, Silvano M, Cerri A, Vergani R, Carlo C. Seborrheic keratosis with compound nevus, junctional nevus and basal cell carcinoma in the same lesion. Dermatology 2001; 203: 265–267.
8. Cohen PR, Rapini RP. Nevus with cyst. Am J Dermatopathol 1993; 15: 229–234.
9. Requena L, Ambrojo P, Sánchez Yus E. Trichilemmal cyst under a compound melanocytic nevus. J Cutan Pathol 1990; 17: 185–188.
10. Malhotra R, Bhawan J, Stadecker M. Association of syringoma and intradermal nevus. Int J Dermatol 1986; 25: 397.
11. González-Vela MC, Val-Bernal JF, Garcia-Alberdi E, González-López MA, Fernández-Llaca H. Trichoadenoma associated with an intradermal melanocytic nevus: a combined malformation. Am J Dermatopathol 2007; 29: 92–95.
12. Izikson L, Sober AJ, Mihm MC, Jr, Zembowicz A. Prevalence of melanoma clinically resembling seborrheic keratoses: analysis of 9204 cases. Arch Dermatology 2002; 138: 1562–1566.
13. Stolz W, Riemann A, Cognetta AB, Pillet L, Abmayr W, Hölzel D, et al. ABCD rule of dermatoscopy: a new practical method for early recognition of malignant melanoma. Eur J Dermatol 1994; 4: 521–527.
14. Cosme Alvarez-Cuesta C, Vazquez-Lopez F, Perez-Oliva N. Dermatoscopy in the diagnosis of cutaneous collision tumour. Clin Exp Dermatol 2004; 29: 199–200.
15. Argenziano G, Soyer HP, De Giorgi V, Piccolo D, Carli P, Delfino M, et al, editors. Interactive atlas of dermoscopy. Milan: Edra Medical Publishing & New Media, 2000.