Sigurd Broesby-Olsen1, Anette Bygum1, Anne-Marie Gerdes2 and Flemming Brandrup1
Departments of 1Dermatology, and 2Biochemistry, Pharmacology and Genetics, Odense University Hospital, Denmark



Sigurd Broesby-Olsen1, Anette Bygum1, Anne-Marie Gerdes2 and Flemming Brandrup1
Departments of 1Dermatology, and 2Biochemistry, Pharmacology and Genetics, Odense University Hospital, Denmark
Multiple self-healing squamous epithelioma of Ferguson-Smith (MSSE) is a rare autosomal dominantly inherited disease, almost exclusively reported in patients of Scottish origin, with recurrent, histologically malignant tumours that undergo spontaneous regression. We report clinical observations in a Danish family with 11 affected patients, which appears to be the first Scandinavian family published with the disease. Anamnestic data and data concerning age of onset, localization, number of tumours and treatment modalities were collected from the family and from medical records, and all living patients were examined. Detailed clinical findings in 6 patients are described, together with a summary of clinical data from all 11 affected family members. The mean age of onset in the family was 52.6 years (range 30–81 years). A total of 44 tumours, chiefly located in sun-exposed areas, were recorded and the average number of tumours per patient was 4 (range 1–23). 61.4% of the tumours were excised, 31.8% regressed spontaneously without treatment. MSSE may thus also affect patients of non-Scottish origin. The disease severity can vary greatly among patients and the onset can be at an advanced age. MSSE constitutes an important model for research into tumour biology. Key words: multiple self-healing squamous epithelioma; MSSE; Ferguson-Smith disease; multiple keratoacanthomas of Ferguson-Smith; skin cancer.
(Accepted June 13, 2007.)
Acta Derm Venereol 2008; 88: 52–56.
Sigurd Broesby-Olsen, Department of Dermatology, Odense University Hospital, DK-5000 Odense C, Denmark. E-mail: s.broesby-olsen@dadlnet.dk
In 1934 the Scottish dermatologist J. Ferguson-Smith described a single case of multiple skin tumours in a 23-year-old man, recurring intermittently since the age of 16 years (1). Spontaneous regression with scarring was observed, in spite of histopathological findings compatible with squamous cell carcinoma (SCC). The same condition was recorded later on in the patient’s daughter (2), and related cases from other families have been published (3, 4). In 1971, Malcolm A. Ferguson-Smith (geneticist, son of the dermatologist) and co-workers (5), presented reliable information on 62 cases of multiple self-healing squamous epithelioma (MSSE) from the west of Scotland, including pedigrees compatible with autosomal dominant inheritance. MSSE has since been mapped to a region on chromosome 9q22 (6), but the gene has not been identified yet. Molecular analyses indicate that the MSSE gene is a new tumour suppressor gene (7).
In this paper we present additional clinical and histopathological findings in a Danish MSSE-family covering 11 patients from three affected generations, which appears to be the first Scandinavian family published with this rare disease.
MATERIALS AND METHODS
A pedigree involving four generations (Fig. 1) was constructed. Anamnestic data were collected, based on information given by affected and non-affected relatives, supplemented with information from medical records including previous histopathological descriptions. Data concerning age of onset, localization, number of tumours and treatment modalities were recorded retrospectively from the medical record files. All living affected relatives were examined. Information about the youngest generation was collected by interviewing the parents because most of these family members were children at the time of the interview.
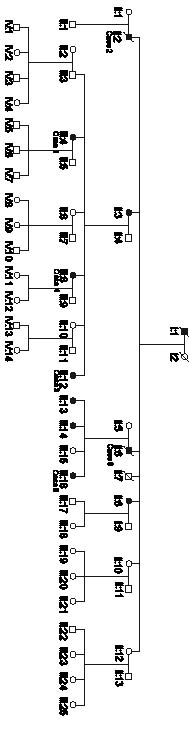
Fig. 1. Pedigree of the family covering four generations. The youngest generation is as yet unaffected, but they are all children or teenagers.
SELECTED CASE REPORTS
Case 1 (patient III:4)
A 51-year-old woman was referred with a 5×5 mm skin tumour on the upper lip, close to the nose (Fig. 2), which had been growing over the course of 2 months. A punch biopsy was interpreted as a highly differentiated SCC. Due to continuous growth up to 15×10 mm, considerable pain and the cosmetically delicate localization, X-ray treatment (54 Gy/18 fractions) was given with an excellent cosmetic result and no recurrence.
Fig. 2. A dome-shaped, yellowish-red, firm tumour on the upper lip, close to the nose.

Since the age of 43 years, multiple tumours, located preferably on the face and arms, had been excised by plastic surgeons. Typically, the process started with a pin-point papule developing within 2–3 weeks into a dome-shaped, yellowish-red nodule with a central hyperkeratotic plug that histopathologically was interpreted as keratoacanthoma (KA) or highly differentiated SCC.
A diagnosis of MSSE was established, based on the multiplicity of KA-like skin tumours and the family history, including experiences from case 2.
Since then, 17 tumours have been observed during 5 years follow-up; 10 of which were excised without recurrence. Seven tumours located on the legs, arms, hands, upper lip, nose and forehead have been observed without treatment. After an initial growth phase, spontaneous regression was achieved in about 4–8 weeks, leaving a small pitted scar. The patient refused prophylactic treatment with etretinate.
The family history revealed several cases of recurring KA or SCC, including case 2, who had been treated in our department 5 years previously.
Case 2 (patient II:2)
A 75-year-old man was referred with a skin tumour on the forehead, which had been gradually expanding in the course of 2 months. A large, 50×55 mm elevated tumour with central hyperkeratinization, crusting and deep infiltration was found in the midline (Fig. 3). Multiple skin biopsies were interpreted as KA, invasive SCC or plaque-type KA. Because of continuing expansion in the direction of the right eye, X-ray treatment was given (54 Gy/18 fractions), which resulted in regression and flattening without recurrence. There were no signs of metastases.
Fig. 3. A large, elevated tumour with central hyperkeratinization, crusting and deep infiltration on the forehead.

Case 3 (patient III:12)
A 43-year-old woman, younger sister of case 1, was diagnosed with her first tumour at the age of 30. The tumour affected her upper lip and had been growing rapidly during a few weeks. A punch biopsy showed SCC and the tumour was excised. The cosmetic result was poor and still very unsatisfactory in spite of later plastic surgical correction and transplantation.
At the age of 37 years she had developed a 6 mm tumour on her right cheek over the course of 2 weeks, which was excised and histology showed invasive SCC. One year later a similar tumour on the nose was excised, and the histological findings were compatible with KA.
In her early forties she developed small tumours affecting the right side of her upper lip, the root of the nose and her chin. The tumours were 3–5 mm in size, dome-shaped, yellowish-red, scaly, with centrally crusted lesions, and initially grew rapidly over weeks, followed by spontaneous regression over 3–4 months leaving small scars (Fig. 4 A, B). The most recent tumour on her right leg, clinically resembling KA, was treated with topical imiquimod 5% (Aldara®, 3M), which had to be stopped after 14 days because of marked inflammation. One week after stopping treatment the tumour had significantly regressed, but 2 weeks later an accelerated growth to 20×18 mm (Fig. 5) was observed, and the tumour was excised.
Fig. 4. (A) A dome-shaped, firm tumour on the left side of the chin. (B) 4 months later. The tumour has healed spontaneously leaving a small scar. Note the unsatisfactory cosmetic result after previous tumour excision on the upper lip despite plastic surgical correction.

Fig. 5. A large keratoacanthoma-like tumour on the leg, after unsuccessful treatment with topical imiquimod 5%. The tumour was later excised.

Case 4 (patient III:8)
A 50-year-old woman, sister of case 1 and 3, developed a 7×7 mm dome-shaped tumour on her chin in the course of a few weeks. A biopsy was interpreted as SCC and excision was planned. However, due to the family history of MSSE combined with signs of obvious regression, excision was cancelled. The tumour regressed completely in 2 months, leaving a small scar.
Case 5 (patient III:16)
A 34-year-old woman, cousin of case 1, 3 and 4, was referred with a flat, keratotic, 5×5 mm tumour on her left cheek with a well-defined border and rolled edges. The tumour was excised and histology was compatible with KA.
Case 6 (patient II: 6)
A 41-year-old man, father of case 5, had gone through previous extensive surgery including skin transplantation due to presumed skin cancer affecting the nose. This was performed many years before a diagnosis of MSSE was established in the family. At the age of 64 years, he presented with a new tumour affecting his forehead developing within 2–3 weeks. It was treated by curettage, and histology showed KA.
RESULTS
The clinical and histopathological findings in the proband and affected relatives are summarized in Table I. Of 11 patients, 3 were male and 8 were female. The mean age of onset was 52.6 years; 61.0 years in males (range 41–75 years) and 49.5 years in females (range 30–81 years). A total of 44 tumours were recorded and the average number of tumours per patient was 4 (range 1–23). Tumours were located chiefly in sun-exposed areas, primarily in the face, subsequently on the exposed areas of the upper- and lower extremities, whereas no tumours were seen on, for example, the abdomen or mucous membranes. Approximately half of the tumours were classified histopathologically as KA, one-quarter as SCC, while biopsies were avoided in the remaining typical tumours.
Table I. Characteristics of the patients
| Patient | Age of onset | No. of lesions | Localization | Histology | Treatment |
| I:1 | 67 | 4 | Face:4 | SCC:4 | Radiotherapy: 1 Excision: 3 |
| II:2 | 75 | 1 | Face | SCC | Radiotherapy |
| II:3 | 81 | 1 | Lower leg | SCC | Spontaneous regression |
| II:6 | 41 | 2 | Face:2 | SCC:1 KA:1 | Excision:2 |
| II:8 | 60 | 2 | Lower leg:2 | KA:2 | Excision:2 |
| III:4 | 43 | 23 | Face:10 Hand/arm:10 Lower leg:3 | KA:15 SCC:1 Unknown:7 | Excision:15 Radiotherapy:1 Spontaneous regression:7 |
| III:8 | 50 | 1 | Face | SCC | Spontaneous regression |
| III:12 | 30 | 7 | Face:5 Hand/arm:1 Lower leg:1 | KA:2 SCC:2 Unknown:3 | Excision:4 Spontaneous regression:3 |
| III:13 | 50 | 1 | Lower leg | Unknown | Spontaneous regression |
| III:14 | 48 | 1 | Hand/arm | Unknown | Spontaneous regression |
| III:16 | 34 | 1 | Face | KA | Excision |
| Cumulated data | 52.6 (mean) (30–81) | 44 | Face: 24 (54.5%) Hand/arm: 12 (27.3%) Lower leg: 8 (18.2%) | KA: 21 (47.7%) SCC: 11 (25%) Unknown: 12 (27.3%) | Excision: 27 (61.4%) Radiotherapy: 3 (6.8%) Spontaneous regression: 14 (31.8%) |
SCC: squamous cell carcinoma; KA: keratoacanthoma
Most of the tumours were excised and radiotherapy was chosen in selected cases. In the follow-up phase of our study, after the diagnosis of MSSE was established in the family, 22 tumours in 3 patients were recorded. Eleven were observed without treatment and regressed spontaneously. The remaining tumours were excised, twice after unsuccessful treatment with imiquimod. Cryotherapy was performed once, without obvious influence on the natural course of that tumour, which regressed in about 6–8 weeks. No metastases were observed in any of the patients.
There was no record of basal cell carcinoma, melanoma, immunosuppression, excess ultraviolet (UV) exposure or arsenic ingestion in the patients, who were all Caucasians.
DISCUSSION
Two large families from the west of Scotland have formed the base of knowledge and research into MSSE, and genetic analyses so far have indicated that the Scottish cases have arisen from a founder mutation before 1790 (5). Apart from a sporadic case reported by Rajka in 1971 (8), this is the first Scandinavian family published with the disease.
The clinical findings of KA-like tumours in the actual family are in agreement with previous case series (1–4). The initial lesions of MSSE are similar to KA and typically localized in light-exposed skin areas. They begin with an acne-like lesion or a reddish macule, developing into a papule and later a nodule with a central crateriform ulcer with rolled edges and often a central horny plug. The tumour is locally destructive and deep local infiltration can be seen. One fatal case from local invasive growth has been described (9), but metastases have, to our knowledge, not been reported. The growth phase is, after a few weeks, followed by spontaneous regression over a period of months leaving pitted scars. Our report includes details of six illustrative cases of MSSE, where the clinical appearance and course of the tumours fits this description. However, the large, widely expanding tumour in case 2 is remarkable.
Age of onset for MSSE is highly variable, ranging from 8 to 62 years, but often with manifestations in young adult life. Ferguson-Smith et al. (5) reported the mean age of onset to be 25.5 years in women and 26.9 in men, and maximum ages of onset 56 and 55 years, respectively. In the actual family the age of onset is higher than reported previously, and it is noteworthy that one of the patients had her first tumour at the age of 81 years.
The disease severity varied greatly among the affected family members, not only by the number of tumours, but also by the course and treatment modalities chosen, which reflects not only the phenotypical variability of MSSE, but also the unpredictable course of every single tumour.
The majority of treatments were recorded retrospectively before a diagnosis of MSSE was established in the family and thus reflects prevailing treatments for SCC or KA. The optimal treatment of MSSE still has to be defined. Tumours tend to involute on their own, but as the growth phase is unpredictable and scarring after spontaneous resolution often unacceptable, early excision is usually performed. However, it is important to avoid mutilating surgery. Other treatment modalities reported include cryotherapy and prophylactic etretinate (10). Radiotherapy has been regarded to have a possible aggravating effect on the disease (3, 5, 10), something we could not confirm in our study.
The pedigree in the actual family is compatible with autosomal dominant inheritance. We observed no skipping of generations and that could indicate a complete penetrance, although the severity of the disease and age of onset are very variable. Due to the relatively late age at onset, clinical discrimination of gene mutation carriers may be impossible. The MSSE gene has not yet been identified, but it has been mapped to chromosomal region 9q22-q31, close to but different from the PTCH gene (6, 7). Linkage analysis in this family (data not shown) demonstrated linkage to the same region on chromosome 9q in both Scottish families and the Danish family, indicating that the same gene is involved in all the MSSE families. The haplotype of the Danish family was different from the Scottish haplotype, indicating that the Danish family is not related to the Scottish families (Frances Richards, personal communication). Molecular analyses of MSSE tumours indicate that the MSSE gene is a tumour suppressor gene (7). UV radiation might play a central role in the tumourigenesis in MSSE, since tumours are localized typically in light-exposed skin areas, but the precise mechanism is not clear. Evidence for an abnormal DNA repair, as in xeroderma pigmentosum, has not been found (10).
From the pedigree of the actual family, anticipation could be suspected; that is: younger age of onset and more severity of the disease in younger generations, but future research is needed to clarify this. In the reported family ascertainment bias concerning age of onset cannot be excluded. It will be interesting to determine whether family members in the youngest generation will develop tumours with an earlier debut.
In view of the varied clinical spectrum of the disease, the histological findings compatible with SCC or KA, and the potentially high age of onset, MSSE may be overlooked and taken for sporadic SCCs or KAs. Thus, a potential familial clustering has to be elucidated in cases of recurring SCC or KA. MSSE constitutes an important model for research into tumour biology, especially when considering the spontaneous regression of the histologically malignant tumours.
ACKNOWLEDGEMENTS
The authors thank Frances Richards for performing the haplotype analysis of the family. The family is thanked for excellent co-operation. Many colleagues from Denmark are thanked for sending patient material.
REFERENCES
1. Smith, J Ferguson. A case of multiple primary squamous-celled carcinomata of the skin in a young man, with spontaneous healing. Br J Dermatol 1934; 46: 267–272
2. Currie AR, Smith J. Ferguson. Multiple primary spontaneous-healing squamous-cell carcinomata of the skin. J Pathol Bacteriol 1952; 64: 827–839
3. Sommerville J, Milne JA. Familial primary self-healing squamous epithelioma of the skin (Ferguson Smith type). Br J Dermatol 1950; 62: 485–490
4. Charteris AA. Self-healing epithelioma of the skin. Am J Roentgenol 1951; 65: 459.
5. Ferguson-Smith MA, Wallace DC, Zoë HJ, Renwick JH. Multiple self-healing squamous epithelioma. Birth Defects 1971; 7: 157–163
6. Goudie DR, Yuille MAR, Leversha MA, Furlong RA, Carter NP, Lush MJ, et al. Multiple self-healing squamous epitheliomata (ESS1) mapped to chromosome 9q22-q31 in families with common ancestry. Nature Genet 1993; 3: 165–169
7. Bose S, Morgan LJ, Booth DR, Goudie DR, Ferguson-Smith MA, Richards FM. The elusive multiple self-healing squamous epithelioma (MSSE) gene: further mapping, analysis of candidates, and loss of heterozygosity. Oncogene 2006; 25: 806–812.
8. Rajka G. Multiple keratoacanthoma (self-healing squamous epithelioma according to Ferguson-Smith). Acta Derm Venereol 1971; 51: 232–233.
9. Chakrabarty KH, Perks AG. Ferguson-Smith syndrome: the importance of long term follow-up. Br J Plast Surg 1996; 49: 497–498.
10. Wright AL, Gawkrodger DJ, Branford WA, McLaren K, Hunter JAA. Self-healing epitheliomata of Ferguson-Smith: cytogenetic and histological studies, and the therapeutic effect of etretinate. Dermatologica 1988; 176: 22–28.

