Yoshio Kawakami1, Koichiro Nakamura2, Akiko Nishibu1, Hirokatsu Yanagihori1, Hideo Kimura3 and Toshiyuki Yamamoto1
Department of Dermatology, 1Fukushima Medical University Graduate School of Medicine, Hikarigaoka-1, Fukushima 960-1295, 2Saitama Medical University Faculty of Medicine, Saitama, and 3Division of Hematology, Kita-Fukushima Medical Center, Fukushima, Japan. E-mail: kawayoshio@yahoo.co.jp
Accepted August 27, 2007.
Sir,
Cutaneous squamous cell carcinoma (SCC) is a common malignant neoplasm derived from suprabasal epidermal keratinocytes. Treatment modalities for SCC include conventional surgical excision, Mohs micrographic surgery, radiation, and non-excisional ablative techniques. For aggressive lesions refractory to conventional treatments, chemotherapy has been performed (1), although it is often discontinued due to adverse side-effects. We report here a case of chronic myeloid leukaemia (CML) complicated by SCC of the face. Unexpectedly, there was a significant regression of SCC during the treatment of CML with the tyrosine kinase inhibitor imatinib mesylate (Gleevec®, Novartis, Tokyo, Japan).
CASE REPORT
An 84-year-old Japanese man presented in September 2006 with a skin lesion on his left cheek. The lesion had appeared 3 years earlier and had gradually increased in size. He had been diagnosed with Philadelphia (Ph) chromosome-positive CML in January 1995. Initial treatment comprised interferon-alpha and hydroxyurea, followed by hydroxyurea alone. Due to intolerance, hydroxyurea treatment was discontinued 11 years later. In August 2006, he was started on imatinib mesylate treatment, 400 mg daily.
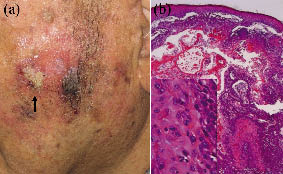
Clinical examination demonstrated an ill-defined ulcerated plaque, measuring 20×25 mm (Fig. 1a). Skin biopsy showed irregular masses of squamoid cells proliferating downward into the dermis. The invading cells were composed of variable degrees of atypical cells with mitosis and showed keratinization (Fig. 1b). Immunohistochemically, the tumour was positive for cytokeratin (CK), but negative for c-kit (CD117). Ziehl-Neelsen staining for Mycobacterium, and periodic acid-Schiff and Grocott-Gomori methenamine-silver nitrate stains for fungi were all negative. Computed tomography (CT) did not reveal any signs of lymphadenopathy or metastasis.
Fig. 1. (a) Ulcerated plaque with ill-defined border on the left cheek (arrow). (b) Irregular proliferation of tumour mass in the dermis in continuity with epidermis (H&E ×25). Inset: tumour cells showing variable degrees of atypical squamous cells with mitosis (H&E ×400).
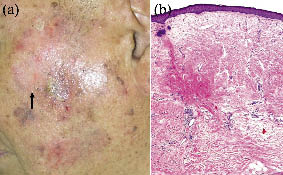
Because a laboratory blood test demonstrated thrombocytopaenia associated with CML, surgical excision of SCC was postponed while waiting for recovery from thrombocytopaenia. Meanwhile, there was a gradual regression of SCC, and after 4 months of imatinib therapy, the skin lesion had flattened significantly (Fig. 2a) and the biopsy specimen taken from the centre of the pre-existing lesion showed normal epidermis with no tumour cells (Fig. 2b). Since December 2006, the patient has been receiving 200 mg of imatinib daily. There has been no recurrence of the skin lesion for 4 months after the last skin biopsy.
Fig. 2. After four months treatment with imatinib mesylate for CML. (a) The skin lesion shown in Fig. 1 had flattened significantly (arrow). (b) Skin biopsy obtained from the centre of the pre-existing lesion showed no evidence of SCC (H&E ×25).
DISCUSSION
In our case, the skin lesion appeared 11 years after treatment with hydroxyurea. As occurrence of SCCs has been reported on sun-exposed sites in patients with CML who are on long-term treatment with hydroxyurea (2), it is thought that hydroxyurea treatment may be involved in the development of this tumour. To our knowledge, this is the first report describing the regression of SCC in a patient with CML during treatment with imatinib. It is possible that the discontinuation of hydroxyurea and the restoration of immune function following treatment of CML with imatinib might play a role in the regression of SCC. However, the possibility of the participation of imatinib in the regression of SCC cannot be excluded.
Imatinib is a tyrosine kinase inhibitor with selectivity for bcr-abl, c-abl, platelet-derived growth factor receptor (PDGFR) and c-kit (3, 4). It is a novel drug for the treatment of CML, which is associated with the reciprocal translocation between chromosomes 9 and 22, resulting in the formation of the Ph chromosome that generates bcr-abl fusion gene (5). Imatinib is also useful in the treatment of gastrointestinal stromal tumours, which overexpress c-kit (6). Furthermore, imatinib shows efficacy in a large proportion of patients with hyper-eosinophilic syndrome, which is associated with rearrangements of PDGFR genes (7).
The potential efficacy of imatinib is also being evaluated in SCC. Previous studies have shown that imatinib exerts a significant inhibitory effect on cell growth in head and neck SCC cell lines (8). In addition, imatinib can enhance the tumour growth reduction induced by radiotherapy in human epidermoid carcinoma cells (9) or by cisplatin in head and neck SCC cell lines (10). Although immunohistochemical studies confirmed the expression of c-abl, PDGFR and c-kit in head and neck SCC cell lines, their expression did not change after imatinib treatment (8), suggesting the existence of an unidentified target inducing tumour growth reduction. On the other hand, recent in vitro studies have demonstrated that imatinib stimulates the activity of epidermal growth factor receptor tyrosine kinase in head and neck squamous tumour despite causing a dose-dependent decrease in the cell number (11). In addition, clinical observation demonstrated the appearance of new, and the progression of existing, squamous epithelial cancers in 2 patients treated with imatinib for CML (12); thus care is required when administering this drug to some cancer patients. Because of such discrepancies, further investigations are required in order to elucidate the difference between cases showing regression or aggravation of SCC. Nevertheless, imatinib is generally well tolerated, with mild side-effects, including oedema, skin rash, arthralgias and myalgias (13), and our case highlights the possibility that imatinib may be beneficial in some cancer patients.
REFERENCES
1. Grossman D, Leffell DJ. Squamous cell carcinoma. In: Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, editors. Fitzpatrick’s dermatology in general medicine, sixth edition. New York, McGraw Hill, 2004: p. 737–747.
2. Vassallo C, Passamonti F, Merante S, Ardigò M, Nolli G, Mangiacavalli S, et al. Muco-cutaneous changes during long-term therapy with hydroxyurea in chronic myeloid leukemia. Clin Exp Dermatol 2001; 26: 141–148.
3. Cohen MH, Williams G, Johnson JR, Duan J, Gobburu J, Rahman A, et al. Approval summary for imatinib mesylate capsules in the treatment of chronic myelogenous leukemia. Clin Cancer Res 2002; 8: 935–942.
4. Roskoski R. STI-571: an anticancer protein-tyrosine kinase inhibitor. Biochem Biophys Res Commun 2003; 309: 709–717.
5. Faderl S, Talpaz M, Estrov Z, Kantarjian HM. Chronic myelogenous leukemia: biology and therapy. Ann Intern Med 1999; 131: 207–219.
6. Baker DE. Imatinib mesylate. Rev Gastroenterol Disord 2002; 2: 75–86.
7. Müller AM, Martens UM, Hofmann SC, Bruckner- Tuderman L, Mertelsmann R, Lübbert M. Imatinib mesylate as a novel treatment option for hypereosinophilic syndrome: two case reports and a comprehensive review of the literature. Ann Hematol 2006; 85: 1–16.
8. Chu HR, Ongkeko WM, Diaz A, Altuna X, Aguilera J, Weisman RA, et al. Growth inhibition of head and neck squamous cell carcinoma by imatinib mesylate (Gleevec). Cancer Ther 2005; 3: 515–524.
9. Oertel S, Krempien R, Lindel K, Zabel A, Milker-Zabel S, Bischof M, et al. Human glioblastoma and carcinoma xenograft tumors treated by combined radiation and imatinib. Strahlenther Onkol 2006; 182: 400–407.
10. Wang-Rodriguez J, Lopez JP, Altuna X, Chu TS, Weisman RA, Ongkeko WM. STI-571 (Gleevec) potentiates the effect of cisplatin in inhibiting the proliferation of head and neck squamous cell carcinoma in vitro. Laryngoscope 2006; 116: 1409–1416.
11. Johnson FM, Saigal B, Donato NJ. Induction of heparin-binding EGF-like growth factor and activation of EGF receptor in imatinib mesylate-treated squamous cell carcinoma cells. J Cell Physiol 2005; 205: 218–227.
12. Baskaynak G, Kreuzer KA, Schwarz M, Zuber J, Audring H, Riess H, et al. Squamous cutaneous epithelial cell carcinoma in two CML patients with progressive disease under imatinib treatment. Eur J Haematol 2003; 70: 231–234.
13. Druker BJ, Talpaz M, Resta DJ, Peng B, Buchdunger E, Ford JM, et al. Efficacy and safety of a specific inhibitor of the BCR-ABL tyrosine. N Engl J Med 2001; 344: 1031–1037.