Aleksandra Zamirska, Adam Reich, Joanna Berny-Moreno, Joanna Salomon and Jacek C. Szepietowski
Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland



Aleksandra Zamirska, Adam Reich, Joanna Berny-Moreno, Joanna Salomon and Jacek C. Szepietowski
Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland
Approximately 80% of psoriatic individuals experience pruritus, of varying intensity. This study evaluated the frequency of vulvar itching and burning and its influence on well-being in women with psoriasis. A total of 93 women were included in the study. Psoriasis severity was assessed according to the Psoriasis Area and Severity Index, the intensity of vulvar discomfort by visual analogue scale and depressive symptoms by Beck’s Depression Inventory. On admission 41 (44.1%) women experienced vulvar discomfort, 18 (19.4%) itching, 10 (10.8%) burning and 13 (14.0%) both itching and burning sensations. Psoriatic lesions on the vulva were found in 22 (23.7%) women. No significant correlation was found between burning or itching intensity and global psoriasis severity (r = 0.19, p = 0.26). Patients with vulvar discomfort had psoriatic lesions on the vulva more often than women without discomfort (43.6% vs. 8.2%, p < 0.001). In addition, patients with vulvar discomfort more frequently demonstrated depressive symptoms (p < 0.05). We conclude that vulvar discomfort is an important clinical problem in women with psoriasis and should be taken into consideration during treatment. Key words: vulvar discomfort; psoriasis; pruritus; pain; vulvovaginal disorders.
(Accepted August 20, 2007.)
Acta Derm Venereol 2008; 88: 132–135.
Adam Reich, Department of Dermatology, Venereology and Allergology, Wrocław Medical University, Ul. Chalubinskiego 1, 50-368 Wrocław, Poland. E-mail. adi_medicalis@go2.pl
Psoriasis is one of the most common skin disorders. Psoriatic lesions are sometimes found on the vulva. Apart from the typical psoriatic lesions, itching is a symptom frequently associated with psoriasis. Previous studies have shown that pruritus occurs in 70–90% of psoriatic individuals during the disease exacerbation (1–3). Itching in psoriasis can be generalized or localized (3). The most common site of itching in psoriasis is the lower limbs, followed by the trunk, upper limbs and scalp (3). Some studies have also shown a significant positive correlation between psoriasis severity and itching intensity (2, 3).
The present study aimed to evaluate vulvar discomfort, defined as pruritus and/or burning sensation of the external female genitalia (mons pubis, labia majora and minora, and clitoris) in women with psoriasis. In addition, it aimed to assess the correlation between vulvar discomfort and psychosocial well-being.
Patients and methods
Participants were recruited consecutively from women hospitalized due to psoriasis exacerbation in the Department of Dermatology, Venereology and Allergology in Wrocław, Poland between November 2001 and January 2003. The inclusion criteria were: subjects who were willing to participate in the study; gave written informed consent; had active psoriatic lesions on the skin; and were literate in Polish. All patients underwent careful dermatological examination including detailed evaluation of the vulva (mons pubis, labia majora and minora, and clitoris). Women showing clinical abnormalities on examination suggesting candidiasis, herpes simplex infection, other types of infections or skin irritation resulting from abnormal vaginal discharges, which might be responsible for pruritic or burning sensations within the vulvar region, were excluded from the study. In addition, direct microscopic examination of a vaginal smear was performed in every patient to exclude candidiasis. Of all the subjects initially surveyed, one refused to participate in the study and a further 2 were excluded due to suspicion of vaginal candidiasis.
A total of 93 women were included in the study: 78 with exacerbated plaque psoriasis (83.9%) and 15 with arthropathic psoriasis and skin lesions (16.1%). All patients gave their written informed consent for participation in the study. The age range of included women was 17–76 years (mean 48.0 ± 16.5 years). The mean age of first onset of disease was 28.6 ± 16.9 years, mean duration of psoriasis 17.5 ± 14.1 years, and mean duration of the current disease exacerbation 3.2 ± 4.9 months. Among the included subjects, 37 (39.8%) had a positive family history of atopic disease.
The clinical severity of psoriasis was assessed according to the Psoriasis Area and Severity Index (PASI) and varied between 2.3 and 49.5 points (mean 15.9 ± 11.5 points). No significant differences regarding disease severity were found between subjects with plaque psoriasis and arthropathic psoriasis (mean PASI 16.5 ± 12.1 points and 14.1 ± 9.4 points, respectively, p = 0.33). The intensity of vulvar discomfort, considered as itching or burning sensations of the vulvar area (mons pubis, labia majora and minora, and clitoris), was evaluated using a 10-point visual analogue scale (VAS): 0 points referred to no itching/burning, 10 points referred to the worst itching/burning. All patients were also asked to complete the Beck’s Depression Inventory (BDI) (4). If a patient scored more than 11 on the BDI she was considered to have depression. A χ2 test with Yates modification, Student’s t-test and Pearson’s correlation test were used for statistical analysis. p-values of less than 0.05 were considered significant.
Results
At the time of examination 41 women (44.1%) experienced vulvar discomfort: 18 (19.4%) reported itching, 10 (10.8%) burning, and the remaining 13 (14.0%) both itching and burning. The intensity of vulvar discomfort assessed according to VAS was 3.8 ± 2.5 points (range 1–10 points). On admission, psoriatic lesions on the vulva were found in 22 (23.7%) women: 4 (4.3%) had only erythema, 7 (7.5%) presented with erythema and scaling, 6 (6.5%) had typical psoriatic plaques, 3 (3.2%) had erythema and oedema, 1 (1.1%) oedema and scaling and 1 (1.1%) erythema and psoriatic papules. In addition, approximately half of the women examined (44 participants, 47.3%) had previously reported vulvar localization of psoriasis during disease flares: 33 (35.5%) sporadically, 10 (10.8) frequently and 1 (1.1%) always. Patients with vulvar itching and/or burning suffered from slightly more severe psoriasis than did those with no symptoms within the external genitalia: mean PASI scoring for both groups 17.9 ± 11.0 points and 14.7 ± 12.4, respectively (p = 0.22) (Table I). There was no significant correlation between itching and/or burning intensity and psoriasis severity assessed by PASI (r = 0.19, p = 0.26). However, there was significant correlation between the presence of vulvar discomfort and vulvar localization of psoriasis: only 4 of 52 women (7.7%) without vulvar discomfort had psoriatic lesions within the vulva compared with 18 of 41 (43.9%) women reporting itching and/or burning within the external genitalia (p < 0.001) (Table I, Fig. 1). The presence of vulvar discomfort was independent of the patients’ age (p = 0.5), duration of psoriasis (p = 0.69), age at first psoriasis onset (p = 0.75), duration of the last exacerbation (p = 0.98), positive family history of atopic disease (p = 0.73) and frequency of admission to dermatological departments (p = 0.08) (Table I).
Table I. Comparison of psoriatic women with and without vulvar discomfort
| Patients with vulvar itching and/or burning n = 41 | Patients without vulvar discomfort n = 52 | p | |
| PASI (points), mean ± SD | 17.9 ± 11.0 | 14.7 ± 12.4 | 0.22 |
| Presence of psoriatic lesions within vulva (%) Yes No | 18 (43.9) 23 (56.1) | 4 (7.7) 48 (92.3) | < 0.001 |
| Age (years), mean ± SD | 46.8 ± 15.3 | 44.4 ± 17.3 | 0.5 |
| Age at disease onset (years), mean ± SD | 28.9 ± 19.3 | 27.7 ± 15.4 | 0.75 |
| Disease duration (years), mean ± SD | 17.9 ± 14.7 | 16.7 ± 13.4 | 0.69 |
| Duration of the last exacerbation (months), mean ± SD | 3.3 ± 6.1 | 3.3 ± 4.0 | 0.98 |
| Family history of atopic diseases (%) Positive Negative | 15 (36.6) 26 (63.4) | 22 (42.3) 30 (57.7) | 0.73 |
| Number of hospitalizations due to psoriasis, mean ± SD | 2.4 ± 2.6 | 1.6 ± 1.1 | 0.08 |
| Negative influence of psoriasis on patients’ well-being (%) None Slight Severe | 6 (14.6) 10 (24.4) 25 (61.0) | 7 (13.5) 21 (40.4) 24 (46.1) | 0.25 |
| Negative influence of psoriasis on patients’ sexual life (%) None Slight Severe Not sexually active | 8 (19.5) 10 (24.4) 15 (36.6) 8 (19.5) | 34 (65.4) 7 (13.5) 5 (9.6) 6 (11.5) | < 0.001 |
| BDI (scores), mean ± SD | 9.6 ± 6.9 | 6.9 ± 5.7 | < 0.05 |
| BDI (%) < 11 scores ≥ 11 scores | 25 (61.0) 16 (39.0) | 42 (80.8) 10 (19.2) | < 0.05 |
BDI: Beck’s Depression Inventory; PASI: Psoriasis Area Severity Index.
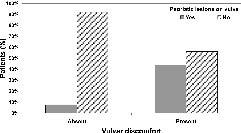
Fig. 1. Relationship between the presence of psoriatic lesions on the vulva and vulvar discomfort (itching and/or burning) χ2 test with Yates modification: p < 0.001.
Of all the women examined, 13 (14.0%) declared that psoriasis had no impact on their psychosocial well-being, 31 (33.3%) stated that psoriasis reduced their well-being slightly, and the remaining 49 (52.7%) regarded psoriasis as having a large negative influence on their psychosocial well-being. Moreover, 17 (18.3%) women stated that psoriasis slightly and 20 (21.5%) severely impaired their sexual life. In 42 patients psoriasis had no influence on their sexual life. The remaining 14 (15.1%) individuals were not sexually active (Table I). Patients reporting vulvar discomfort significantly more frequently stated that psoriasis had a negative influence on their sexual life (p < 0.001) (Table I). In addition, 34 (64.2%) of these participants stated that itching and/or burning within the vulva had a negative impact on their psychosocial well-being: slight in 17 (32.1%) and severe in 17 (32.1%); in the remaining 19 (35.8%) females vulvar discomfort had no negative impact on well-being. Regarding depressive symptoms, it was observed that patients reporting vulvar discomfort on admission had significantly higher BDI scores than women without itching and/or burning within the vulvar region (9.6 ± 6.9 vs. 6.9 ± 5.7, respectively, p < 0.05) (Fig. 2). Moreover, among women with vulvar discomfort, depression was noted more frequently (BDI > 11) compared with patients with no symptoms within the vulva (39.0% vs. 19.2%, respectively, p < 0.05).

Fig. 2. Comparison of depressive symptoms between women with and without vulvar discomfort Student’s T test: p < 0.05. SE, standard error; SD, standard deviation.
Fifty-three (57.0%) women had reported vulvar discomfort during previous psoriasis exacerbations: 39 (41.9%) sporadically, 12 (12.9%) frequently, and 2 (2.2%) always. Among this group, 38 (71.7%) women believed that the vulvar discomfort was connected with psoriasis flares, 9 (17.0%) with the involvement of vulva by psoriasis, 4 (7.5%) with the concomitant pruritus of the skin and only 2 (3.8%) subjects stated that vulvar discomfort was unrelated to psoriasis. Among 53 women experiencing vulvar discomfort at any time in the past, 29 (54.7%) had never, 13 (24.5%) sporadically, and only 11 (20.8%) always reported these symptoms during visits to the dermatological outpatient clinic. Fourteen (26.4%) patients requested help from the gynaecologist in relieving vulvar discomfort. Directed treatment was applied by 28 (52.8%) women. The following treatment modalities were applied: topical corticosteroids: 12 patients (22.6%); anti-psoriatic preparations: 2 patients (3.8%); disinfectants: 2 patients (3.8%); anti-mycotics: 1 patient (1.9%); anti-histamic drugs: 1 patient (1.9%); topical anti-inflammatory drugs: 1 patient (1.9%); moist compresses with boric acid: 1 patient (1.9%). The symptoms of itching and/or burning were relieved, when psoriatic lesions disappeared in 29 women (54.7%), when pruritus of the skin was reduced in 11 women (20.8%), after directed treatment in 10 women (18.9%), and independently of psoriasis symptoms in 3 subjects (5.7%).
Discussion
Chronic or recurrent vulvar discomfort is an embarrassing clinical problem (5). Most patients with chronic symptoms within the vulva suffer frequently from dermatological conditions and they are commonly referred to dermatologists. The most frequent dermatoses affecting the vulva are irritant or contact dermatitis, vulvovaginal candidiasis, lichen sclerosus and lichen planus (6–8). Psoriasis is considered as a cause of vulvar discomfort in approximately 5% of all women with itching or burning of the vulva (7). However, the exact data concerning the prevalence and intensity of vulvar discomfort among women with psoriasis has been poorly investigated.
The current study revealed a high prevalence of vulvar itching and/or burning in women with psoriasis. Approximately half of participating subjects experienced vulvar discomfort at the time of examination. Moreover, a strong relationship was found between vulvar symptoms and the presence of psoriatic lesions within the vulvar region. Although we cannot definitely exclude the possibility that some patients might have other gynaecological conditions that are responsible for pruritus or burning of the vulva region, several factors strongly suggested that the reported ailments within the vulva were related to psoriasis in at least the majority of examined women: the majority of patients (88.7%) combined the presence of vulvar discomfort with psoriasis exacerbation or with vulvar location of psoriatic lesions. In over 50% of women vulvar discomfort resolved after the disappearance of psoriatic lesions within the skin. Moreover, the presence of psoriatic lesions within the vulva region strongly correlated with the presence of itching and/or burning of the vulva, and there was no relationship between vulvar discomfort and previous gynaecological diseases or a positive family history of atopic disorders.
Psoriasis is a skin disease with great impact on patients’ psychosocial well-being (9). According to previous studies, the quality of life of psoriatic patients is markedly impaired (10, 11). The symptoms of depression are also observed more frequently in patients with psoriasis than in the general population (12). Based on our study, it could be supposed that vulvar discomfort is an important clinical symptom contributing to the development of depression in women with psoriasis. Although the mean intensity of itching or burning within the vulva was quite low (VAS = 3.8), these symptoms should not be underestimated as these patients had a significantly higher scoring on the BDI and more frequently scored over 11 on the BDI, which strongly indicates depression. Remarkably, over 50% of investigated women with vulvar discomfort had never reported these symptoms to dermatologists. In addition, because intimate body regions are often omitted from typical examination of patients, the problem of vulvar discomfort may be overlooked in psoriatic subjects. However, as demonstrated in our study, vulvar discomfort significantly impairs sexual life and may lead to depression in women with psoriasis. We therefore recommend always asking women with psoriasis about vulvar symptoms and examining the whole patient including the genital region. It was demonstrated recently that psoriatic patients also have increased risk of other systemic diseases, including myocardial infarction, heart arrhythmia, diabetes mellitus and metabolic syndrome (13–17). Taken together, strong evidence exists that psoriasis is not only a dermatological disorder with skin involvement, but represents a disease with significant internal organ and psychiatric co-morbidity.
In conclusion, psoriasis may frequently be responsible for vulvar discomfort among women with this disease. Moreover, itching and/or burning of the vulva accompanying psoriasis significantly influences psychosocial well-being. Therefore, all dermatologists should be aware of the high frequency and clinical importance of genital symptoms in psoriasis.
References
1. Yosipovitch G, Goon A, Wee J, Chan YW, Goh CL. The prevalence and clinical characteristics of pruritus among patients with extensive psoriasis. Br J Dermatol 2000; 143: 969–973
2. Reich A, Wisnicka B, Szepietowski JC. Itching in psoriasis. Kosmetische Medizin 2004; 2: 77–82.
3. Szepietowski JC, Reich A, Wisnicka B. Itching in patients suffering from psoriasis. Acta Dermatovenereol Croat 2002; 10: 221–226.
4. Beck AT, Steer RA. Manual for the Beck Depression Inventory. San Antonio, TX: The Psychological Corporation, 1993.
5. Manolache L, Benea V, Vulcan P, Diaconu JD, Maier N. Clinical and therapeutical aspects in vulvodynia. Dermatol Klin 2003; 5: 169–173.
6. Fischer G, Spurret B, Fischer A. The chronically symptomatic vulva: aetiology and management. Br J Obstet Gynaecol 1995; 102: 773–779.
7. Fischer GO. The commonest causes of symptomatic vulvar disease: a dermatologist’s perspective. Australas J Dermatol 1996; 37: 12–18.
8. McKay M. Vulvitis and vulvovaginitis: cutaneous considerations. Am J Obstet Gynecol 1991; 165: 1176–1182.
9. de Korte J, Sprangers MAG, Mombers FMC, Bos JD. Quality of life in patients with psoriasis: a systematic literature review. J Invest Dermatol Proc 2004; 9: 140–147.
10. Szepietowski J, Salomon J, Finlay AY, Klepacki A, Chodynicka B, Marionneau N, et al. Dermatology Life Quality Index (DLQI): Polish version. Dermatol Klin 2004; 6: 63–70.
11. Hrehorow E, Reich A, Szepietowski J. Quality of life of patients with psoriasis: relationship with pruritus, stress and symptoms of depression. Dermatol Klin 2007, 9: 35–38.
12. Pacan P, Szepietowski JC, Kiejna A. Stressful life events and depression in patients suffering from psoriasis vulgaris. Dermatol Psychosom 2003; 4: 142–145.
13. Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. J Am Med Assoc 2006; 296: 1735–1741.
14. Markuszeski L, Bissinger A, Janusz I, Narbutt J, Jedrzejowska AS, Zalewska A. Heart rate and arrhythmia in patients with psoriasis vulgaris. Arch Med Res 2007; 38: 64–69.
15. Sommer DM, Jenisch S, Suchan M, Christophers E, Weichenthal M. Increased prevalence of the metabolic syndrome in patients with moderate to severe psoriasis. Arch Dermatol Res 2006; 298: 321–328.
16. Szepietowski JC, Bielicka E, Wasik F, Kopec W, Szepietowski T. Microalbuminuria as a subclinical marker of renal impairment in subjects with psoriasis vulgaris. J Eur Acad Dermatol Venereol 2000; 14: 513–514.
17. Szepietowski J, Szepietowski T. Is renal function altered in patients with psoriasis vulgaris? – a short review. J Dermatol 2000; 25: 569–572.

