Vincenzo de Giorgi1, Barbara Alfaioli1, Daniela Massi2, Alessia Gori1, Serena Sestini1, Federica Papi1, Marta Grazzini1 and Torello Lotti1
1Department of Dermatology, and 2Department of Human Pathology and Oncology, University of Florence, Via della Pergola 60, IT-50121 Firenze, Italy. E-mail: vincenzo.degiorgi@unifi.it
Accepted January 21, 2008.
Sir,
Pilomatricoma (known previously as “calcifying epithelioma of Malherbe”) is a slowly growing benign adnexal skin tumour. This neoplasm is usually asymptomatic and painless (although some patients report pain during episodes of inflammation or ulceration). It is considered an epithelioma that arises from hair follicles with cytodifferentiation of the hair matrix cells and the cells of the inner sheath. Pilomatricoma develops from an abnormal formation of cells that are similar to hair cells, which become hardened or calcified, in the lower dermis and subcutaneous fat. The calcified cells form a solitary firm nodule beneath the skin (1).
Pilomatricoma typically affects young individuals, most cases occurring in children. There is a slightly higher prevalence in females. It is more common on the face and neck, but it is sometimes found on the scalp, eyelids and arms. The lesion is usually solitary, but there are multiple forms, that are associated with myotonic dystrophy, Gardner’s syndrome and other genetic disorders (1, 2). Diagnosing this lesion is usually easy, but there is a rare variant termed bullous, that can create some diagnostic problems.
CASE REPORT
A 9-year-old boy presented with a red/rose, translucent, protruding soft nodular mass on the abdomen. The lesion had been present for 5–6 months and had grown progressively, reaching considerable dimensions (12 × 10 × 13 mm) in a few months. The overlying skin appeared slightly erythematous and presented telangiectasies and minor haemorrhages, determining the red coloration of the nodule (Fig. 1). The lesion was soft to the touch and extremely mobile, the skin around the lesion was normal in consistency and colour. Thorough palpation revealed the presence in depth, within the derma, of a nodular lesion with irregular limits. There was no history of any particular local trauma or chronic irritation at the sight of the lesion. There was no regional lymphoadenopathy. Systemic examination was normal. Laboratory examination of haematological, biochemical, and urinalysis tests was normal.
Fig. 1. Pinkish, erythematous lesion, with regular and clearly defined limits, soft to the touch, appearing in a short time on the abdominal region of a 9-year-old boy.
Formulating a certain clinical diagnosis was difficult and, considering the slow, but constant, growth of the lesion, we decided to remove it for diagnostic purposes. The lesion was removed surgically in its entirety, both its surface thickness and its underlying deep nodule, and subjected to histopathological examination.
Histopathological examination showed a relatively well-circumscribed dermal cystic lesion surrounded by connective tissue stroma. The lesion was characterized by large masses of eosinophilic cornified material (faulty hair matrix) containing shadow (ghost) cells, squamoid cells and foci of basaloid cells (matrical and supramatrical cells) surrounded by a dense inflammatory infiltrate with giant cells (Fig. 2). Basaloid cells exhibited deeply basophilic oval or round nuclei and a variable number of mitotic figures. In the superficial dermis overlying the lesion we observed numerous dilated lymphatic vessels rimmed by thinned endothelium (Fig. 3). A final histopathological diagnosis of pilomatricoma was made. Considering the clinical examination and the presence at the histopathological level of numerous dilated lymphatic vessels, we formulated a clinical-pathological diagnosis of bullous pilomatricoma.
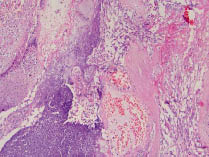
Fig. 2. The lesion displayed basaloid cells (matrical and supramatrical cells) and eosinophilic cornified material (faulty hair matrix) containing shadow (ghost) cells surrounded by a dense inflammatory infiltrate with extravasated erythrocytes (H&E × 20).
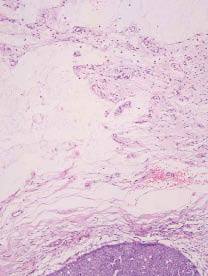
Fig. 3. Numerous dilated lymphatics were seen in the superficial dermis overlying the lesion. Epidermis is shown at the top (H&E × 20).
The patient was clinically free of disease at his recent follow-up 2 years after treatment.
DISCUSSION
The bullous form of pilomatricoma is clinically characterized by a soft, heavily folded, striae-like skin appearance and focal loss of elastic fibres in the dermis above the pilomatricoma, mimicking secondary anetoderma (3–5).
The incidence of pilomatricoma with a bullous appearance is estimated to range between 3% and 6%, according to cases reported in the literature (2, 3, 5, 6).
Theories have been proposed to explain the bullous appearance seen on pilomatricomas. The main role in bullous appearance is attributed to lymphatic obstruction, and it has been postulated that the pressure on the area around the hard core of the pilomatricoma induces the obstruction of lymphatic vessels and congestion of lymphatic fluid. This results in the dilation of lymphatic vessels, the leakage of lymphatic fluid, and oedema in the dermis surrounding the tumour, producing a bullous appearance (2, 6). Lymph contains fibrinogen and other coagulation factors and has the ability to form a coagulation thrombus during lymph stasis (7). In an unusual case of bullous pilomatricoma, Lao et al. (7) described papillary endothelial hyperplasia within dilated lymphatic vessels overlying a typical pilomatricoma, resulted from peculiar organization of a thrombus, which is similar to the process occurring in blood vessels.
Our case also presented a difficult pre-surgery diagnosis. Possible diagnoses were: a bullous morphea that presented similar characteristics, a lymphangioma, but also a feared cutaneous lymphoma (3, 8, 9).
Our case was peculiar given its location on the abdomen; a location that has not been reported previously in the literature, and for the rapidity of the lesion’s growth (5–6 months), which is generally slower.
Like classical pilomatricoma, since this form does not regress spontaneously, surgical excision is the treatment of choice because recurrence is rare. Although malignant transformation has been described, it is exceedingly rare (10).
References
1. Kumaran N, Azmy A, Carachi R, Raine PA, Macfarlane JH, Howatson AG. Pilomatrixoma-accuracy of clinical diagnosis. J Pediatric Surg 2006; 41: 1755–1758.
2. Fetil E, Soyal MC, Menderes A, Lebe B, Gunes AT, Ozkan S. Bullous appearance of pilomatricoma. Dermatol Surg 2003; 29: 1066–1067.
3. Weichert GE, Bush KL, Crawford RI. Bullous pilomatricoma: a report of clinical and pathological findings and review of dermal bullous disorders. J Cutan Med Surg 2001; 5: 394–396.
4. Darwish AH, Al-Jalahema EK, Dhiman AK, Al-Khalifa KA. Clinicopathological study of pilomatricoma. Saudi Med J 2001; 22: 268–271.
5. Yiqun J, Jianfang S. Pilomatricoma with a bullous appearance. J Cutan Path 2004; 31: 558–560.
6. Inui S, Kanda R, Hata S. Pilomatricoma with a bullous appearance. J Dermatol 1997; 24: 57.
7. Lao L, Kumakiri M, Kiyohara T, Sakata K, Takeuchi A. Papillary endothelial hyperplasia and dilated lymphatic vessels in bullous pilomatricoma. Acta Derm Venereol 2005; 85: 160–163.
8. Daoud MS, Su WP, Lieferman KM, Perniciaro P. Bullous morphea: clinical pathologic, and immunopathologic evaluation of thirteen cases. J Am Acad Dermatol 1994; 30: 937–943.
9. Synkowski DR, Lobitz WC, Provost TT. Bullous scleroderma. Arch Dermatol 1981; 117: 135–137.
10. Mathen LC, Olver JM, Cree IA. A large rapidly growing pilomatrixoma on a lower eyelid. Br J Ophthalmol 2000; 84: 1203–1204.