Cornelia S. Seitz1, Axel Trautemann1, Eva-Bettina Bröcker1, Marianne Abele-Horn2 and Matthias Goebeler3
1Department of Dermatology, Venerology and Allergology, 2Institute of Hygiene and Microbiology, University of Würzburg, Josef-Schneider-Str. 2, DE-97080 Würzburg, and 3Department of Dermatology, University Hospital Mannheim, University of Heidelberg, Mannheim, Germany. E-mail: seitz_c@klinik.uni-wuerzburg.de
Accepted January 21, 2008.
Sir,
Mycobacterium haemophilum was first isolated in 1978 from a patient with Hodgkin’s disease suffering from septic arthritis and nodular skin lesions (1). Since then, infections with M. haemophilum have primarily been reported in two different groups of patients: (i) immunocompromised adults with organ or bone marrow transplants, haematological malignancies or advanced HIV infection (2); and (ii) immunocompetent children with cervico-facial lymphadenitis (3).The clinical presentation of M. haemophilum infections is variable and may include cellulitis, arthritis, osteomyelitis and pneumonia. Here, we report on a patient suffering from long-standing rheumatoid arthritis who presented with skin lesions that could be attributed to infection with M. haemophilum. This case report illustrates the difficulties of identification, isolation and eradication of this rarely reported pathogen.
CASE REPORT
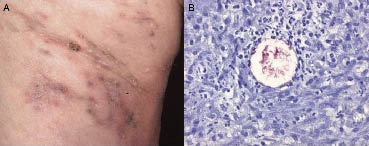
A 67-year-old woman with a 30-year history of rheumatoid arthritis who was treated with prednisolone (5 mg/day) and azathioprine (50 mg/day) presented to our outpatient clinic with nodular and pustular lesions that had initially developed on her right upper buttock and subsequently spread on her right upper lateral thigh (Fig. 1A). Biopsy of a nodule revealed a granulomatous reaction pattern with scattered neutrophils. On careful microscopic examination a few acid-fast bacilli were identified (Fig. 1B). Upon culture under standard laboratory conditions (cultures for non-tuberculous mycobacteria in both solid and liquid media at 30°C and 37°C with haemin-containing supplements), initially non-tuberculous mycobacteria of the M. chelonae/abscessus complex were isolated. Therapy with clarithromycin (500 mg twice daily) and ciprofloxacin (500 mg twice daily) was initiated, leading to a complete resolution of skin lesions within 4 months. However, several months later, under maintenance antibiotic treatment, several skin nodules developed distally from the original sites of infection. At this time-point, 10 new punch biopsies were obtained. While acid-fast bacilli could be observed microscopically in 7 of 10 biopsies, isolation was not successful in any of them and identification of M. haemophilum was only achieved by 16S rRNA sequencing. Treatment was switched to a combination of rifabutin, myambutol and clarithromycin, leading to a complete resolution of symptoms. Unfortunately, 8 weeks after initiation of the triple therapy, the patient developed complete loss of vision due to drug-induced uveitis and endophthalmitis. After withdrawal of rifabutin and myambutol and subsequent continuation of clarithromycin as monotherapy, the patient’s eye symptoms completely resolved and skin lesions slowly cleared.
Fig. 1. (A) Brownish-reddish papules, nodules and pustules on erythematous skin located on the right upper thigh. (B) Skin biopsy revealing a granulomatous and neutrophilic reaction pattern. Identification of acid-fast micro-organisms in skin tissue (Ziehl-Neelsen staining).
DISCUSSION
M. haemophilum is a slowly growing mycobacterium that differs from other non-tuberculous mycobacteria by its culture requirements. Besides ferric iron supplementation, optimal growing conditions include a temperature of 28–30°C (2, 4). Therefore, with conventional isolation procedures using routine media, M. haemophilum may not be isolated. More recently, new diagnostic procedures using molecular biology techniques, such as real-time PCR, have facilitated quick and reliable detection of mycobacterial strains that have been previously undetectable with conventional methods (5–8). In our case non-tuberculous mycobacteria of the chelonae/abscessus group had initially been isolated. Several months later, after treatment and recurrence of skin lesions, M. haemophilum was identified by 16S rRNA sequencing only, despite optimal culture conditions for isolation of slowly growing non-tuberculous mycobacteria. Whether the initial identification of the fast-growing mycobacteria of the chelonae/abscessus group was due to contamination or to a co-infection of 2 non-tuberculous mycobacteria with overgrowth of the fast-growing mycobacteria of the chelonae/abscessus group remains speculative.
Non-tuberculous mycobacteria are ubiquitously present micro-organisms in soil and water. While in earlier studies the occurrence of M. haemophilum was restricted to areas with large water reservoirs (2) or were due to coral-related injuries (9), more recent reports have also identified clusters of reported cases in urban areas (10). Potential modes of infection with M. haemophilum are currently speculative and may include inhalation and ingestion. Due to the high frequency of cutaneous lesions as the initial presentation in the course of infection, inoculation of micro-organisms via unnoticed microtraumata is also conceivable (2, 11). In this context it may be of interest that clusters of infections were also reported from one medical centre suggesting iatrogenic infections, although the mode of transmission could not be identified (12).
A limited number of M. haemophilum infections have been reported in patients receiving immunosuppressive therapies for chronic inflammatory diseases, such as Crohn’s disease (2), lupus erythematosus (13) or rheumatoid arthritis (2, 14). While our patient, who received a maintenance therapy with azathioprine and low-dose corticosteroid, initially developed cutaneous lesions, 2 of the 3 previously reported patients with M. haemophilum infection and underlying rheumatoid arthritis initially presented with lymphadenopathy and one patient with synovial involvement (2).
In a case series of 13 immunocompromised adults with M. haemophilum infection communicated by Strauss et al. (10), cutaneous lesions were the most common initial sign of infection and most frequently developed on the extremities, often overlying the joints (15–17). Infrequently, panniculitis and fistula formation are observed. Localized skin infection may disseminate to other sites probably by haematogenous spread rather than following lymphatic drainage.
There are currently no treatment guidelines for M. haemophilum infections (4). Susceptibility testing had revealed sensitivity of M. haemophilum to rifamycin, amikacin, ciprofloxacin, clarithromycin and clofazimine, and to a somewhat lesser extent to streptomycin, whereas most isolates were resistant to isoniazid (18). After start of the antibiotic treatment, initial deterioration and even spreading of skin lesions may occur. It is recommended to apply a combination of two antibiotic drugs to minimize the risk of relapses and the development of resistance. Furthermore, antibiotic therapy should be maintained for at least 12 months. In cases presenting with osteomyelitis or lung involvement, treatment with a triple combination including a macrolide, a quinolone and rifamycin may be necessary (18).
REFERENCES
1. Sompolinsky D, Lagziel A, Naveh D, Yankilewitz T. Mycobacterium haemophilum sp. Nov., a new pathogen of humans. Int J Syst Bacteriol 1978; 28: 67–75.
2. Saubolle MA, Kiehn TE, White MH, Rudinsky MF, Armstrong D. Mycobacterium haemophilum: microbiology and expanding clinical and geographic spectra of disease in humans. Clin Microbiol Rev 1996; 9: 435–447.
3. Bruijnesteijn van Coppenraet ES, Kuijper EJ, Lindeboom JA, Prins JM, Claas ECJ. Mycobacterium haemophilum and lymphadenitis in children. Emerg Infect Diseases 2005; 11: 62–68.
4. Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. ATS mycobacterial Diseases Subcommittee; An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 2007; 15; 175: 367–416.
5. Samra Z, Kaufmann L, Zeharia A, Ashkenazi S, Amir J, Bahar J, et al. Optimal detection and identification of Mycobacterium haemophilum in specimens from pediatric patients with cervical lymphadenopathy. J Clin Microbiol 1999; 37: 832–834.
6. Bruijnesteijn van Coppenraet ES, Lindeboom JA, Prins JM, Claas ECJ, Kuijper EJ. Real-time PCR assay using fine-needle aspirates and tissue biopsy specimens for rapid diagnosis of mycobacterial lymphadenitis in children. J Clin Microbiology 2004; 42: 2644–2650.
7. Wang SX, Sng LH, Leong HN, Tan BH. Direct identification of mycobacterium haemophilum in skin lesions of immunocompromised patients by PCR-restriction endonuclease activity. J Clin Microbiology 2004; 42: 3336–3338.
8. van Coppenraet LS, Smit VT, Templeton KE, Claas EC, Kuijper EJ. Application of real-time PCR to recognize atypical mycobacteria in archival skin biopsies: high prevalence of mycobacterium haemophilum. Diagn Mol Pathol 2007; 16: 81–86.
9. Smith S, Taylor GD, Fanning EA. Chronic cutaneous Mycobacterium haemophilum acquired from coral injury. Clin Infect Dis 2003; 37: e100–e101.
10. Straus WL, Ostroff SM, Jernigan DB, Kiehn TE, Sordillo EM, Armstrong D, et al. Clinical and epidemiologic characteristics of Mycobacterium haemophilum, an emerging pathogen in immunocompromised patients. Ann Intern Med 1994; 120: 118–125.
11. Dobos KM, Quinn FD, Ashford DA, Horsburgh CR, King CH. Emergence of a unique group of necrotizing mycobacterial diseases. Emerg Infect Dis 1999; 5: 367–378.
12. White MH, Papadopoulos EB, Small TN, Kiehn TE, Armstrong D. Mycobacterium haemophilum infections in bone marrow transplant recipients. Transplantation 1995; 60: 957–960.
13. Teh CL, Kong KO, Chong APY, Badsha H. Mycobacterium haemophilum infection in an SLE patient on mycophenolate mofetil. Lupus 2002; 11: 249–252.
14. Darling TN, Sidhu-Malik N, Corey GR, Allen NB, Kamino H, Murray MC. Treatment of mycobacterium haemophilum infection with an antibiotic regimen including clarithromycin. Br J Dermatol 1994; 131: 376–379.
15. Dever LL, Martin JW, Seaworth B, Jorgensen JH. Varied presentations and responses to treatment of infections cased by mycobacterium haemophilum in patients with AIDS. Clin Infect Dis 1992; 14: 1195–1200.
16. Geisler WM, Harrington RD, Wallis CK, Harnisch JP, Liles C. Broad spectrum of dermatologic manifestations caused by mycobacterium haemophilum infection. Arch Dermatol 2002; 138: 229–230.
17. von Stebut E, Wiest K, Braeuninger W. Chronic infiltrates and persisting ulcerations on the arms and legs. Arch Dermatol 2005; 141: 897–902.
18. Shah MK, Sebti A, Kiehn TE, Massarella SA, Sepkowitz KA. Mycobacterium haemophilum in immunocompromised patients. Clin Infect Dis 2001; 33: 330–337.