Atrichia with papular lesions is a rare autosomal recessive condition characterized by complete irreversible hair loss during the first months of life and papules that appear during early childhood. Atrichia with papular lesions is frequently misdiagnosed as alopecia universalis, despite increasing reports of its prevalence and the presence of well-defined diagnostic criteria. Most cases of atrichia with papular lesions have been reported in consanguineous families residing in small geographical regions, but the increasing number of sporadic cases of unrelated individuals suggests that atrichia with papular lesions is more common than previously thought. Mutations in the human hairless gene on chromosome 8p12 have been implicated in this disease. Here, we report two novel heterozygous mutations in an Australian family and a novel homozygous mutation in 2 Arab siblings. We also revise the diagnostic criteria for atrichia with papular lesions in order to clarify its uniqueness and distinguishing features from alopecia universalis. Key words: hair loss; alopecia universalis; mutation; atrichia with papular lesions.
(Accepted February 5, 2008.)
Acta Derm Venereol 2008; 88: 346–349.
Abraham Zlotogorski, Department of Dermatology, Hadassah - Hebrew University Medical Center, Jerusalem IL-91120, Israel. E-mail: zloto@cc.huji.ac.il
Atrichia with papular lesions (APL; papular atrichia, OMIM 209500) is a rare autosomal recessive condition characterized by complete irreversible hair loss during the first months of life that mimics alopecia universalis, followed by widespread papules that appear during early childhood. Linkage to chromosome 8p12 was initially reported in 1998 (1–3), and the identification of mutations on the human hairless gene (HR) in this chromosomal region have been implicated in its pathogenesis. There are 30 known mutations, including nonsense, missense, deletion, insertion, splice site and compound mutations (4–7). The HR gene encodes a putative zinc finger transcription factor protein that is exclusively expressed in the brain and skin (1). In APL, the absence of this protein results in highly dysregulated hair cycles (8) and permanently immature hair follicle structures, resulting in papules that are made up of follicular cysts filled with cornified material (9).
Zlotogorski et al. (9) described 12 clinical and laboratory criteria for diagnosing APL, which included atrichia, papules, and a family history of consanguinity. APL is still under-diagnosed, despite established diagnostic criteria and increasing reports of its sporadic prevalence. It is important to recognize APL and differentiate it from alopecia areata, as treatments for APL are futile, and treatments for refractive alopecia areata can have significant side-effects. Previous reports of APL have concentrated on certain Mediterranean and Pakistani populations due to the high incidence of consanguinity in these regions. However, the increasing reports of novel compound mutations outside these geographic boundaries suggest that APL is not exclusive to consanguineous families and is more prevalent than previously thought. The first report of a compound heterozygous mutation in a non-consanguineous individual was in 2002 (10), thereafter followed by another 5 reports (4, 11, 12). Here, we report 2 novel heterozygous mutations in an Australian family and a novel homozygous mutation in 2 Arab siblings. We also revise the diagnostic criteria for APL, with the aim of further clarifying and simplifying its diagnosis and distinguishing features from alopecia universalis.
CASE REPORTS
Case 1
A 2-year-old Australian boy presented for assessment of alopecia totalis with no associated nail, teeth or sweating abnormalities. His parents were unrelated, and his father was of Italian and his mother of Australian-British descent. The few scalp hairs present at birth were shed by 1–2 weeks of age and no hair had grown subsequently. He had previously been treated unsuccessfully for alopecia areata with topical corticosteroids. On examination, there was complete atrichia and sparse eyebrows. Eyelashes were present bilaterally. A few smooth and milia-like papules were present on his scalp, cheeks and upper arms (Fig. 1a). There were also whitish hypopigmented streaks on his scalp.
Fig. 1. (a) Dermal papules on the extensor surface of the arm in case 1. These papules can be difficult to differentiate clinically from keratosis pilaris but, histologically, these are follicular cysts filled with cornified material. (b) Complete scalp atrichia with a few papules in case 2.
Case 2
A 14-year-old Arab girl presented for assessment of universal alopecia with no teeth, nail or sweating abnormalities. She also had a 9-year-old brother who was similarly affected. Both of them had full scalps of hair at birth, but most hairs were shed by 3 months of age, leaving only a few that they also lost by the age of 1 year. Their parents, who were first cousins, and their 11-year-old brother, were unaffected. In both affected siblings, examination revealed complete atrichia (Fig. 1b), and sparse eyebrows and eyelashes. The boy had numerous smooth and whitish papules on the face, but, interestingly, the girl reported that the majority of her facial papules had regressed with age. Both siblings had papules on the scalp and in the elbow and knee regions.
Scalp biopsy was declined in both cases due to the potential for psychological trauma.
MATERIALS AND METHODS
Genomic DNA was extracted from cases 1 and 2 and their families, after obtaining written informed consent. All HR gene exons and splice junctions were amplified via polymerase chain reaction (PCR) and the PCR products were purified in Centriflex Gel Filtration Cartridges (Edge Biosystems, Gaithersburg, MD, USA). Direct sequencing was performed in an ABI Prism 310 Automated Sequencer, using the ABI Prism Big Dye Terminator Cycle Sequencing Ready Reaction Kit (PE Applied Biosystems, Foster City, CA, USA), as described previously (13).
RESULTS
Case 1 was a compound heterozygote for a maternally-derived nonsense mutation and a paternally-derived insertion mutation. The nonsense mutation, Q719X, resulted from a C→T transition that produced a premature stop codon in exon 9 of the HR gene (Fig. 2a). The insertion mutation, 342insCCAGG, resulted from the insertion of 5 base pairs in exon 3 of the HR gene (Fig. 2b) and was associated with a frameshift and an early termination codon at position 364 of the HR gene. Patient 2 and her brother carried a homozygous mutation that resulted from a duplication of 16 base pairs (ATGGCTCACACGGCAC) in exon 3 of the HR gene (Fig. 2c). This mutation was associated with a frameshift and an early stop codon at the end of the inserted amino acid sequence at position 417 of the HR gene. Together, this is the first report of insertion mutations in exon 3 of the HR gene.
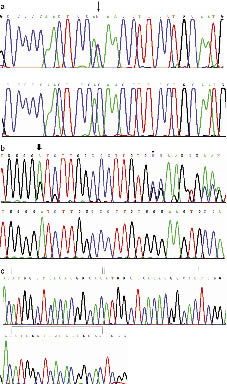
Fig. 2. (a) Nonsense mutation, Q719X, in exon 9 of the human hairless (HR) gene (arrow). Upper panel: patient 1; lower panel: unrelated control. (b) Heterozygous insertion of 5 bp (342insCCAGG) in exon 3 of the HR gene (thin arrow). Upper panel: patient 1; lower panel: unrelated control. A known SNP, rs12675375, is indicated by the thick arrow. (c) Homozygous 16-bp duplication in exon 3 of the HR gene. The bars indicate the duplicated sequence. Upper panel: patient 2; lower panel: unrelated control.
DISCUSSION
In the past, APL was considered to be rare, as most reported cases were of homozygous mutations in consanguineous families (9). Increasing sporadic reports of APL in non-consanguineous individuals in different populations indicate that its prevalence may be underestimated due to the lack of awareness and frequent misdiagnosis as its phenocopy, alopecia universalis. The rarer condition, vitamin-D-dependent rickets, also mimics APL and presents with atrichia in the first few months of life and papules made up of follicular cysts filled with cornified material within the first few years of life.
Interestingly, there is very little phenotypic variation in APL despite various mutations in the HR gene that have been described. These and all previously described mutations for APL are distributed along the HR gene with no particular sharing of “hot spots” or common mutations. The current Arab family originated from a small geographical region near Jerusalem, where 3 other affected families with APL were reported previously. One would expect there to be a founder mutation, but, interestingly, this is the fourth different mutation described in this region, and the tenth novel mutation in Israel (4). Therefore, it is important to sequence all coding regions, including exon-intron junctions of the entire gene. In APL, most affected individuals are born with full heads of hair, which shed in the first few months of life to progress invariably to universal alopecia. Case 1 had only a few scalp hairs present at birth and he also had preserved eyelashes, suggesting that some degree of phenotypic variation could occur. There was also a history of regression of facial papules in case 2 with time. The regression of papules in older age groups has actually been our consistent observation, although the reason for this is unclear (14). There are no mature hair follicle structures present in APL, due to the ineffective programming of hair cycle dynamics early in life. It is therefore unlikely that this regression is a result of hormonal influence on absent hair follicles that are usually hormone-responsive.
Although histological assessment forms part of the diagnostic criteria, a scalp biopsy is not always feasible in younger children due to its invasive nature and potential for causing psychological trauma. In most cases, confirmation of diagnosis with genetic testing is adequate to complement a good clinical history and physical examination. The above-mentioned factors, learnt through increasing experience with diagnosing APL, and the common clinical observations that have been reported in approximately 70 cases of APL in the literature, calls for a timely revision of the diagnostic criteria initially described by Zlotogorski et al. (9).
We propose to divide the diagnostic criteria into 5 major and 5 minor criteria, whereby 4 out of 5 major criteria are required to make the diagnosis of APL and the minor criteria are supplementary to this diagnosis (Table I). The major criteria would include the permanent and complete absence of scalp hairs, eyebrows and eyelashes by the first few months of life, the presence of few to widespread smooth, whitish or milia-like papules on the face, scalp, arms, elbows, thighs or knees from infancy or childhood, findings on scalp histology that support the diagnosis of APL, and the confirmation of diagnosis with mutations in the HR gene through genetic testing. Since atrichia with papular lesions and similar histological findings can also be seen in vitamin-D-dependent rickets, the clinical and molecular exclusion of this condition is also an important major criterion.
Genetic testing is the gold standard for diagnosis, since it can clearly distinguish alopecia universalis and vitamin-D-dependent rickets from APL. The minor criteria would include a possible family history of consanguinity, normal growth and development, the presence of white hypopigmented streaks on the scalp, the absence of secondary or body hair growth, and the lack of response to any treatment modality.
Table I. Revision of diagnostic criteria for atrichia with papular lesions
|
MAJOR CRITERIA
(4 out of 5 required for diagnosis)
• Permanent and complete absence of scalp hairs by the first few months of life.
• Few to widespread smooth, whitish, or milia-like papules on the face, scalp, arms, elbows, thighs or knees from infancy or childhood.
• Replacement of mature hair follicle structures by follicular cysts filled with cornified material in scalp histology.
• Mutation(s) in the human hairless gene through genetic testing.
• Clinical and/or molecular exclusion of vitamin-D-dependent rickets.
|
|
MINOR CRITERIA
(supplementary criteria)
• Family history of consanguinity.
• Absence of secondary axillary, pubic, or body hair growth and/or sparse eyebrows and eyelashes.
• Normal growth and development, including normal bones, teeth, nails and sweating.
• Whitish-hypopigmented streaks on the scalp.
• Lack of response to any treatment modality.
|
This revision aims clearly to distinguish APL from the more common alopecia universalis and the rarer vitamin-D-dependent rickets, to aid in its correct diagnosis and also highlights another milestone in our understanding of this condition since its initial description a decade ago.
ACKNOWLEDGEMENTS
We would like to thank both patients and their families for their participation in this study, and Ms Sofia Babay for expert technical assistance. This study was supported in part by the Authority for Research and Development, Hebrew University of Jerusalem (AZ).
REFERENCES
1. Ahmad W, Faiyaz ul Haque M, Brancolini V, Tsou HC, ul Haque S, Lam H, et al. Alopecia universalis associated with a mutation in the human hairless gene. Science 1998; 279: 720–724.
2. Nothen MM, Cichon S, Vogt IR, Hemmer S, Kruse R, Knapp M, et al. A gene for universal congenital alopecia maps to chromosome 8p21–22. Am J Hum Genet 1998; 62: 386–390.
3. Sprecher E, Bergman R, Szargel R, Raz T, Labay V, Ramon M, et al. Atrichia with papular lesions maps to 8p in the region containing the human hairless gene. Am J Med Genet 1998; 80: 546–550.
4. Ashoor GG, Greenstein RM, Lam H, Martinez-Mir A, Zlotogorski A, Christiano AM. Novel compound heterozygous nonsense mutations in the hairless gene causing atrichia with papular lesions. J Dermatol Sci 2005; 40: 29–33.
5. Betz RC, Indelman M, Pforr J, Schreiner F, Bauer R, Bergman R, et al. Identification of mutations in the human hairless gene in two new families with congenital atrichia. Arch Dermatol Res 2007; 299: 157–161.
6. Kim H, Wajid M, Kraemer L, Shimomura Y, Christiano AM. Nonsense mutations in the hairless gene underlie APL in five families of Pakistani origin. J Dermatol Sci 2007; 48: 207–211.
7. Wali A, Ansar M, Khan MN, Ahmad W. Atrichia with papular lesions resulting from a novel insertion mutation in the human hairless gene. Clin Exp Dermatol 2006; 31: 695–698.
8. Panteleyev AA, Botchkareva NV, Sundberg JP, Christiano AM, Paus R. The role of the hairless (HR) gene in the regulation of hair follicle catagen transformation. Am J Pathol 1999; 155: 159–171.
9. Zlotogorski A, Panteleyev AA, Aita VM, Christiano AM. Clinical and molecular diagnostic criteria of congenital atrichia with papular lesions. J Invest Dermatol 2002; 118: 887–890.
10. Henn W, Zlotogorski A, Lam H, Martinez-Mir A, Zaun H, Christiano AM. Atrichia with papular lesions resulting from compound heterozygous mutations in the hairless gene: A lesson for differential diagnosis of alopecia universalis. J Am Acad Dermatol 2002; 47: 519–523.
11. Indelman M, Bergman R, Lestringant GG, Peer G, Sprecher E. Compound heterozygosity for mutations in the hairless gene causes atrichia with papular lesions. Br J Dermatol 2003; 148: 553–557.
12. Paller AS, Varigos G, Metzker A, Bauer RC, Opie J, Martinez-Mir A, et al. Compound heterozygous mutations in the hairless gene in atrichia with papular lesions. J Invest Dermatol 2003; 121: 430–432.
13. Ahmad W, Zlotogorski A, Panteleyev AA, Lam H, Ahmad M, ul Haque MF, et al. Genomic organization of the human hairless gene (HR) and identification of a mutation underlying congenital atrichia in an Arab Palestinian family. Genomics 1999; 56: 141–148.
14. Zlotogorski A, Martinez-Mir A, Green J, Lamdagger H, Panteleyev AA, Sinclair R, et al. Evidence for pseudodominant inheritance of atrichia with papular lesions. J Invest Dermatol 2002; 118: 881–886.





