Toshimitsu Fukui, Daisuke Watanabe, Yasuhiko Tamada and Yoshinari Matsumoto
Department of Dermatology, Aichi Medical University School of Medicine, Aichi, Japan



Toshimitsu Fukui, Daisuke Watanabe, Yasuhiko Tamada and Yoshinari Matsumoto
Department of Dermatology, Aichi Medical University School of Medicine, Aichi, Japan
Surgical resection is the first-choice therapy for extramammary Paget’s disease, but extensive resection is highly invasive and non-surgical treatments are sometimes preferred. Although photodynamic therapy (PDT) has been used for extramammary Paget’s disease for some time, recurrence and residual tumour cells are common. In the present study, five patients with extramammary Paget’s disease with a total of eight lesions first underwent carbon dioxide (CO2) laser abrasion, followed by 3 h of occlusive application of aminolaevulinic acid (ALA) and then 100 J/cm2 irradiation with a 630-nm excimer dye laser. This combination treatment regime was repeated every 2 weeks for a total of 3 times. Group 1 comprised two patients (five lesions) who received CO2 laser and ALA-PDT only. Group 2 comprised three patients (three lesions) who received CO2 laser and ALA-PDT for residual tumour cells following surgery. Follow-up examinations showed that seven lesions in five patients had not recurred after 12 months, suggesting the efficacy of the present method. Key words: extramammary Paget’s disease; photodynamic therapy; carbon dioxide laser.
(Accepted October 20, 2008.)
Acta Derm Venereol 2009; 89: 150–154.
Toshimitsu Fukui, Department of Dermatology, Aichi Medical University School of Medicine, 21 Karimata, Yasago, Nagakute, Aichi-gun, Aichi 480-1195, Japan. E-mail: toshisan@aichi-med-u.ac.jp
Topical photodynamic therapy (PDT) with 5-aminolaevulinic acid (ALA) is a potentially advantageous treatment modality for certain non-melanoma skin cancers, such as actinic keratosis, superficial basal cell carcinoma and Bowen’s disease (1). For extramammary Paget’s disease (EMPD), use of topical and systemic PDT has been reported in combination with surgery, radiation and chemotherapy (2). Shieh et al. (3) performed ALA-PDT to treat 16 lesions in 5 patients, and complete remission was achieved in 8 lesions (50%) at follow-up after 6 months, but recurrence was confirmed in 3 patients 3–4 months later. We previously performed ALA-PDT on 2 patients with EMPD. One patient showed postoperative recurrence and ALA-PDT was combined with radiotherapy. The other patient did not want to undergo surgical resection and PDT alone was performed. When EMPD recurred 2 months later, PDT was again performed on the peripheral area, resulting in remission. The patients experienced no urinary dysfunction following PDT, and aesthetically favourable results were obtained (4).
Raspagliesi et al. (5) performed methyl ALA-PDT (MAL-PDT) on 7 patients with postoperative recurrence of vulvar EMPD and reported clinical and histological cure rates of 57% and 21%, respectively. While complete cure of vulvar EMPD by MAL-PDT would be difficult, PDT would be useful for alleviating symptoms and treating postoperative recurrence.
Therefore, while PDT may be useful for treatment of EMPD, measures must be taken to improve its therapeutic effects by preventing the survival of residual tumour cells as well as early recurrence. In addition, long-term follow-up is necessary after PDT to assess therapeutic results. To improve therapeutic effects, we focused on improving ALA permeability. In recent years, Fang et al. (6) used the Erb:YAG laser (wavelength 2940 nm) to irradiate the dorsal skin of pigs and ablate the stratum corneum, reporting marked increases in permeability of externally applied ALA (6). We subsequently irradiated a total of eight lesions in five patients with EMPD with a carbon dioxide (CO2) laser, followed by 3 h of occlusive application of ALA, and then 100 J/cm2 irradiation with a 630 nm excimer dye laser (PDT EDL-1, Hamamatsu Photonics K.K., Hamamatsu, Japan). This combination treatment regime was repeated every 2 weeks for a total of 3 times. Seven lesions in five patients had not recurred by 12 months after therapy, suggesting the usefulness of the present protocol.
METHODS
Patients
Among patients who visited the Department of Dermatology at the University Hospital of Aichi Medical University and were clinically and histopathologically diagnosed with EMPD, the combination of CO2 laser irradiation and PDT was performed to treat a total of eight lesions in five patients after obtaining consent from the patients and their families. Specifically, we treated five lesions that recurred in two patients who did not wish to undergo surgery and were receiving topical ALA-PDT (by our previous PDT protocol; 50–100 J/cm2 of 630-nm excimer dye laser at each treatment, with a total of ≥ 500 J/cm2) and three lesions in three patients who displayed residual tumour cells postoperatively. The study protocol was approved by an appropriate institutional review board at Aichi Medical University.
CO2 laser assembly
The CO2 laser (COL-1040; Nidek K.K., Tokyo, Japan) has a wavelength of 10,600 nm and is equipped with a scanning mode and repeat action function. Using the skin of 6 healthy volunteers, 4, 6, 8 or 10 Watt (W) was irradiated twice and biopsy was then performed 2 or 3 weeks after the last treatment for histological analysis.
Production of protoporphyrin IX
Production of protoporphyrin IX (PpIX) in normal skin and CO2 laser-irradiated skin 3 h after applying 20% ALA ointment were measured by using a spectrophotometer (m&m Co., Ltd. Tokyo, Japan). The ratio of absorbance at 636 nm and 500 nm was taken as an indicator of PpIX production.
Treatment
With each lesion, local anaesthesia was performed using 1% xylocaine (containing epinephrine). After irradiating with the CO2 laser up to 1 cm away from the margin of the lesion, the crust was removed. After applying 20% ALA ointment to the lesions, which were sealed with plastic wrap and covered with aluminium foil to eliminate exposure to light for approximately 3 h. Subsequently, the treatment site was irradiated with pulsed laser light at a wavelength of 630 nm at 100 J/cm2 using an excimer dye laser (Hamamatsu Photonics K.K). Each lesion was irradiated 3 times with a total of 300 J/cm2. The above procedures were repeated every 2 weeks for a total of 3 times.
Two weeks after the third irradiation, a skin biopsy was performed on all lesions. Patients were followed every 3 months for up to 12 months of therapy. At each follow-up visit, the treated site was thoroughly examined visually and by palpation. If recurrence was suspected, skin biopsy was performed to confirm histopathologically the presence or absence of recurrence.
RESULTS
Pilot experiments in haelthy skin
Before carrying out CO2 laser-PDT in the patient, the dose-response of CO2-laser was established in healthy skin. At 4 W, only degeneration of the stratum corneum was seen. At 6 W, degeneration was seen from the stratum corneum to the stratum spinosum of the epidermis, but few changes were evident in the basal cell layer. With 8 W, vacuolization was seen in basal cells. With 10 W, partial degeneration of the subepidermal papillary layer was seen (Fig. 1). Subsequently, the output of the CO2 laser was set at 8 or 10 W for EPMD lesions.
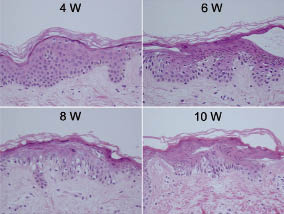
Fig. 1. Histological examination of healthy human skin treated with CO2 laser abrasion. 4 Watt: the stratum corneum was slightly damaged. 6 Watt: degeneration was visible from the stratum corneum to the stratum spinosum of the epidermis, but few changes were evident in the basal cell layer. 8 Watt: vacuolization was seen in basal cells. Finally, 10 Watt: partial degeneration of the subepidermal papillary layer was visible.
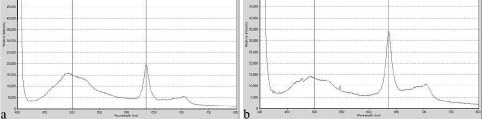
We also confirmed the production of PpIX using spectrophotometry. Production of PpIX was elevated after external application of ALA in healthy skin that was irradiated by the CO2 laser (Fig. 2).
Fig. 2. 5-aminolaevulinic acid (ALA)-induced protoporphyrin IX production in healthy human skin measured using spectrophotometry. (a) ALA was applied under polythene occlusion. Absorbance ratio (636.00/500.00) = 1.3126. (b) ALA was applied after CO2 laser (10 W) ablation = 2.5691.
Patie’t results
Table I shows therapeutic results for the 5 patients. Group 1 comprised patients who received ALA-PDT only, while Group 2 comprised patients who received ALA-PDT due to positive resection margins at surgery.
Table I. Clinical characteristics of Paget’s disease lesions treated with carbon dioxide (CO2) laser abrasion and 5-aminolaevulinic acid-photodynamic therapy (ALA-PDT) and the outcome at follow-up. All lesions were treated with CO2 laser abrasion and topical 20% ALA-PDT.
| Patient number | Age (years)/sex | Location of lesions | Prior failed therapies | CO2 laser + PDT margin (cm) | Clinico-patho-logical results | Outcome at follow-up | |||
| After 3 months | After 6 months | After 12 months | Total F/U (months) | ||||||
| Group 1 | |||||||||
| 1 | 81/M | Penile base | ALA-PDT | 1.0 | CR | CR | CR | CR | 18 |
| 2 | 84/F | Genitala | ALA-PDT | 1.0 | CR | CR | CR | CR | 17 |
| Group 2 | |||||||||
| 3 | 66/F | Cutaneous vulvar and perianal | Excision | 1.0 | CR | CR | CR | CR | 15 |
| 4 | 76/F | Extra urethra and cutaneous vulvar | Excision | 0.5 | CR | CR | CR | CR | 12 |
| 5 | 83/F | Labia majora and cutaneous vulvar | Excision | 1.0 | CR | CRb |
|
| 3 |
aIn case 2 the original lesion was divided into four parts. Three parts were treated and one was used as a non-treated control.
bCase 5 died of other causes.
CR: complete response (100% clearance); F/U: follow-up after last treatment.
Case 1 had received 630 J/cm2 of topical ALA-PDT, but had changed to the present protocol due to recurrence, and no recurrence was seen 18 months later (Fig. 3). Case 2 had been treated multiple times with topical ALA-PDT (total 1050 J/cm2) due to broad distribution of the lesion on both labia majora. However, as the big lesion recurred, it was divided into four sections (upper and lower sections on each side) and the present protocol was used to perform ALA-PDT three times, achieving complete remission in two sections. In Group 2, case 3 was treated using the present protocol (ALA-PDT three times) due to detection of residual tumour cells from the external urethral orifice to around the perianal region following surgical resection, and no recurrence was seen 15 months later. Case 4 also showed residual tumour cells at the external urethral orifice following resection, but recurrence was not seen 12 months after following the present protocol. Case 5 had residual tumour cells from the vagina to the perianal region following surgery. Two weeks after treatment using the present protocol, biopsy confirmed complete remission. Although no recurrence had been seen for 3 months, the patient died of intracranial haemorrhage.

Fig. 3. Case 1. Extramammary Paget’s disease in the penile region. (a) Depigmented macules and erythema were observed prior to combination therapy with carbon dioxide (CO2) laser and aminolaevulinic acid-photodynamic therapy (ALA-PDT). (An adhesive tape strip holds the penis in place). (b) Numerous Paget’s cells were present within the epidermis (haematoxylin and eosin (H&E); original magnification × 200). (c) Scaling had remitted 2 weeks after combination therapy and (d) No residual Paget’s cells were seen at the treated site (original magnification × 200).
DISCUSSION
EMPD is an intraepithelial neoplasia affecting mainly the genital region in elderly patients (7). Paget’s cells generally remain confined to the epidermis and prognosis is good. However, invasive EMPD is frequently associated with regional lymph-node metastasis and has a poor prognosis (8).
Standard treatment is surgical excision with intraoperative margin control. As EMPD occurs in areas that are important for sexual activities and excretion, damage due to surgical invasiveness and radiotherapy can markedly lower the patient’s quality of life. As an alternative therapy, because normal structures and functions are not compromised and aesthetically favourable results are achieved, PDT has been used in the treatment of EMPD (2). However, the rate of recurrence remains high, and Shieh et al. (3) concluded that lesions > 5.5 cm in diameter and those with a dense infiltration of Paget’s cell or greater adnexal involvement did not respond favourably to topical ALA-PDT. In order to increase the therapeutic efficacy of ALA-PDT, sufficient uptake of ALA by tumour cells and appropriate irradiation from a light source are critical. We therefore examined the usefulness of laser dermabrasion and excimer irradiation.
Fang et al. (6) irradiated the dorsal skin of pigs with an Erb:YAG laser (wavelength 2490 nm) to ablate the stratum corneum. Compared with controls, the permeability of externally applied ALA increased 4- to 305-fold. Instead of using the Erb:YAG laser, we irradiated EMPD lesions with 8–10 W of CO2 laser in scanning mode, then applied ALA-PDT externally. In Group 1, complete remission was achieved 12 months later for the two lesions in cases 1 and 2. In Group 2, residual tumour cells were seen around the anus and urethral orifice in cases 3 and 4, and re-operation would have required a change in the urethral passage or compromised rectal function. With the present protocol, tumour cells disappeared, and favourable findings were obtained without causing disorders of urination or defecation.
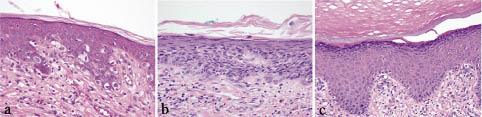
Ablation by CO2 laser, as used in the present study, can reduce the number of Paget’s cells (Fig. 4), but this alone is often insufficient to achieve complete remission (9), and deep irradiation can cause scarring. However, good results were obtained in combination with ALA-PDT. The production of PpIX was elevated after external application of ALA in healthy skin by the CO2 laser irradiation (Fig. 2). Also, Jun et al. (10) recently showed that when a section of healthy skin was cultured ex vivo and ALA was subsequently administered, PpIX production in pilosebaceous units was observed over time. There is reason to believe therefore that after CO2 laser irradiation, ALA quickly penetrates skin appendages and promotes PpIX production. Thus combining CO2 laser abrasion with ALA-PDT it probably destroys Paget’s cells that have invaded skin appendages too.
Fig. 4. Histological findings of extramammary Paget’s disease with carbon dioxide (CO2) laser and combination (CO2 laser and photodynamic therapy) treatment. (a) Before treatment. (b) Residual Paget’s cells were seen after CO2 laser treatment. (c) Tumour cells had disappeared after combination therapy. The massive hyperkeratosis probably occurred as post-inflammatory effect by this treatment (H&E; original magnification × 200).
Further to destroing the stratum corneum the CO2 laser may cause thermal degeneration of melanin in the genitalia. Melanin pigmentation in the genitalia is relatively high in Asians, including Japanese. Therefore, the subsequent excimer dye laser can penetrate deeper due to reduced absorption by melanin. Importantly, EMPD has a tendency to invade along skin appendages, and therapy that reaches deep tissue is required. In conclusion, with the present protocol, the lesion is first ablated using a CO2 laser, while the subsequent combination of ALA-PDT creates a synergistic effect in the treatment of EMPD, enabling long-term maintenance of complete remission.
The authors declare no conflict of interest.
REFERENCES
1. Morton CA, Brown SB, Collins S, Ibbotson S, Jenkinson H, Kurwa H, et al. Guidelines for topical photodynamic therapy: report of a workshop of the British Photodermatology Group. Br J Dermatol 2002; 146: 552–567.
2. Henta T, Itoh Y, Kobayasi M, Ninomiya Y, Ishibashi A. Photodynamic therapy for inoperable vulval Paget’s disease using δ-aminolaevulinic acid: successful management of a large skin lesion. Br J Dermatol 1999; 141: 347–349.
3. Shieh S, Dee AS, Cheney RT, Frawley NP, Zeitouni NC, Oseroff AR. Photodynamic therapy for the treatment of extramammary Paget’s disease. Br J Dermatol 2002; 146: 1000–1005.
4. Mikasa K, Watanabe D, Kondou C, Kobayashi M, Nakaseko H, Yokoo K, et al. 5-aminolevulinic acid-based photodynamic therapy for the treatment of two patients with extramammary Paget’s disease. J Dermatol 2005; 32: 97–101.
5. Raspagliesi F, Fontanelli R, Rossi G, Ditto A, Solima E, Hanozet F, et al. Photodynamic therapy using a methyl ester of 5-aminolevulinic acid in recurrent Paget’s disease of the vulva: A pilot study. Gynecol Oncol 2006; 103: 581–586
6. Fang JY, Lee WR, Shen SC, Fang YP, Hu CH. Enhancement of topical 5-aminolaevulinic acid delivery by erbium: YAG laser and microdermabrasion: a comparison with iontophoresis and electroporation. Br J Dermatol 2004; 151: 132–140.
7. Shepherd V, Davidson EJ, Davies-Humphreys J. Extramammary Paget’s disease. Br J Gynecol 2005; 112: 273–279.
8. Jones RE, Austin C, Ackerman AB. Extramammary Paget’s disease. A critical reexamination. Am J Dermatopathol 1979; 2: 101–132.
9. Choi JB, Yoon ES, Yoon DK, Kim DS, Kim JJ, Cho JH. Failure of carbon dioxide laser treatment in three patients with penoscrotal extramammary Paget’s disease. Br J Urol Int 2001; 88: 297–298.
10. Jun MS, Han I, Choi HS, Kim M, Kim JC. In vitro and ex vivo protoporphyrin IX expression induced by 5-aminolevulinic acid in human pilosebaceous unit. J Dermatol Sci 2005; 40: 68–70.

