Hitoe Torisu-Itakura1,2, Eijun Itakura2,3, Rie Horiuchi4, Miyuki Matsumura4, Hiromaro Kiryu5, Taizo Takeshita1, Yuko Ohjimi6 and Masutaka Furue2
1Department of Dermatology, Saga Prefectural Hospital Koseikan, Saga, 840-8571, Departments of 2Dermatology and 3Anatomic Pathology, Kyushu University, Fukuoka, 4Department of Dermatology, Shunseikai Higuchi Hospital, Kasuga, Departments of 5Dermatology and 6Pathology, Fukuoka University, Fukuoka, Japan. E-mail: itakurah@jwci.org
Accepted October 30, 2008.
Sir,
Cutaneous ciliated cysts are rare benign lesions predominantly occurring on the lower extremities of young women. The morphological similarity of the cyst lining cells to the epithelium of Fallopian tubes suggests their Müllerian origin (1, 2). We present here a case of cutaneous ciliated cyst occurring on the leg of a Japanese woman of menopausal age.
CASE REPORT
A 51-year-old Japanese woman presented with a 2-year history of a mass in the posterior region of her left leg. According to the patient, the mass was painless, but had gradually increased in size. She had a medical history significant for cystic endometriosis of the ovaries at the age of 40 years. Physical examination revealed a soft, solitary mass, measuring 15 mm in diameter. There was no abnormality in the overlying skin. Laboratory investigation results including complete blood cell count and blood chemistry were normal. These finding were suggestive of a keratinous cyst. Accordingly, the lesion was removed completely under local anaesthesia. On surgical exploration, it became apparent that the mass was a round cyst with a slightly blue hue (Fig. 1). After surgical removal, examination of the cyst wall resulted in the escape of clear serous fluid from the cystic cavity.
Fig. 1. Intra-operative view of the mass following incision on the leg revealing a round cyst with a slightly blue hue.
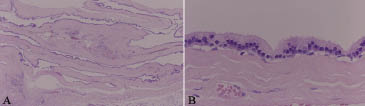
Histological sections were stained with haematoxylin and eosin, periodic acid-Schiff (PAS), Alcian blue and mucicarmine. Further sections were used for immunohistochemistry for cytokeratin (AE1/AE3), epithelial membrane antigen (EMA), S-100 protein, oestrogen receptor and progesterone receptor. Histo- pathological examination revealed a multi-loculated cyst located in the deep dermis (Fig. 2A). Simple cuboidal or columnar ciliated cells resembling Müllerian epithelium substantially lined the cyst wall. The cyst was surrounded by loose connective tissue without smooth muscle. There were a few small papillae projecting into the cystic cavities. Examination under high-power magnification revealed fine cilia on the luminal side of the epithelial lining (Fig. 2B). Inflammatory infiltrate was absent. Alcian blue staining showed slight positivity in the liminal side of the lining cells, although other mucin histochemistries with PAS or mucicarmine were negative. Immunohistochemical staining revealed strong membrane positivity to epithelial membrane antigen and diffuse cytoplasmic reaction to cytokeratin (AE1/AE3) in the epithelial component. There was focal nuclear staining for oestrogen receptor within the epithelial cells. Intranuclear staining for progesterone receptors was not identified. No staining of the epithelial cells was observed with S-100 protein.
Fig. 2. (A) The multi-loculated cyst lined by a substantially monolayered epithelium located in the deep dermis and subcutaneous tissue. (B) High-magnification view of ciliated cuboidal to columnar epithelium lining the cyst.
DISCUSSION
Cutaneous ciliated cysts occur almost exclusively in women. On electron microscopy, the ciliary shaft contains an array of nine peripheral microtubule pairs arranged in a circle around two single microtubules (3, 4). This finding is identical to that of normal human ciliated cells found in the epithelium of the airway, Fallopian tube, middle ear and in the ependymal lining of the brain and spinal cord. Also, similar immunohistochemical staining patterns for dynein, which functions as microtubule-based molecular motors, is seen in both cutaneous ciliated cysts and Fallopian tube epithelium (5). Positive nuclear staining for oestrogen receptor and/or progesterone receptor also supports the Müllerian histogenetic hypothesis (6, 7).
Heterotopic Müllerian duct cell migration during early embryogenesis has been proposed as an explanation for cutaneous ciliated cysts’ anatomical predilection for the lower extremities and buttocks. Al-Nafussi & Cardner (8) suggested that cells from the fimbrial ends of the Fallopian tubes developing from the Müllerian ducts could detach and become incorporated into the lateral mesoderm where the lower limb buds arise. These cells could then migrate and be arrested locally in the area of the lower back and abdomen or in the stream of the growing lower limb bud. These arrested cells should remain dormant until puberty when, under the influence of ovarian hormone stimulation, the heterotopic Müllerian epithelium produces serous fluid resulting in cystic formation.
Retroperitoneal Müllerian cysts have been described as another example of Müllerian cysts (9). These cysts may involve peritoneum and lymph nodes and occasionally arise in the mediastinum (10). Although the site of occurrence is different, cutaneous ciliated cysts are considered to be analogous to these extra-genitourinary Müllerian cysts, which are also believed to arise from Müllerian rests.
Typically, cutaneous ciliated cysts occur in young women during their adolescent or reproductive years, as these cysts remain quiescent until puberty when ovarian hormones probably stimulate them to grow and manifest clinically. According to the literature, the most common age range affected is between 12 and 42 years. The case described here involves a 51-year-old woman who presented with a cutaneous ciliated cyst, which had been dormant presumably until her menopausal age. Hormonal imbalance at menopausal age may affect a dormant Müllerian rest and may eventually develop the cyst. To our knowledge, this is the oldest patient in the literature with this rare cutaneous ciliated cyst.
As previous authors have pointed out, the term “cutaneous ciliated cyst” is confusing. In the cutaneous lesions, ciliated epithelium may be encountered in a bronchogenic cyst, thyroglossal duct cyst or vulvar cyst. These cysts are usually lined by ciliated epithelium, which is similar to that of a cutaneous ciliated cyst, histologically and ultrastructurally. However, distinctive features differentiate them from cutaneous ciliated cysts. Bronchogenic cysts, which usually occur in the neck, differ from cutaneous ciliated cysts in that they contain mucous glands and goblet cells. Thyroglossal duct cysts, which also typically occur in the neck, frequently contain thyroid follicles (11). Ciliated epithelium may be seen in some vulvar and vaginal cysts. Müllerian cysts, which are predominantly comprised of columnar, mucin-producing endocervical epithelium, have ciliated columnar, Fallopian-tube-like epithelium in two-thirds of cases. On the other hand, Gardner’s ducts (mesonephric) are lined by non-ciliated, low cuboidal epithelium and are thought to arise from vestigial remnants of the mesonephric (Wolffian) duct (12). Bartholin’s duct cyst and paraurethral (Skene’s) gland cysts, which are predominantly lined by transitional epithelium, may focally show ciliated columnar epithelium (13).
Ciliated metaplasia of eccrine or apocrine duct epithelia is another hypothesis for histogenesis of ciliated cysts. It has been advocated that rare unexplainable case reports of ciliated cysts at lower extremities in male patients (14, 15) may represent ciliated metaplasia of eccrine cysts (4, 5). We are in agreement with these authors that the cases of ciliated cysts on the foot are probably a separate pathogenetic entity.
We believe that cutaneous ciliated cysts are a distinct entity occurring in females, probably arising from hormonal activation of a Müllerian rest.
REFERENCES