Atopic dermatitis (AD) has been sub-classified into extrinsic and intrinsic types according to the presence or not of allergen-specific IgE antibodies. Although total serum IgE levels are frequently elevated in AD, their potential to predict allergen-specific IgE (asIgE) has rarely been studied. We investigated 103 children with AD and suspected allergen-specific sensitization. A thorough clinical examination, a structured medical history and total serum IgE and asIgE measurements were performed. Fifty-three male and 50 female patients, median age 35 months (range 3 months to 17 years), were recruited. Sixty-three percent of patients were asIgE positive, while 37% did not reveal such IgE antibodies; median total serum IgE levels were 224.0 kU/l (14–12,013 kU/l) and 25.2 kU/l (0–4352 kU/l), respectively. Associations of asIgE status with atopic co-morbidity and total serum IgE levels were statistically significant. At a cut-off total serum IgE level of 106 kU/l (sensitivity 68.7%; specificity 92.3%), positive and negative predicted values (93.6% and 64.3%, respectively) were determined. Clinical decision points predictive of positive asIgE results were identified in 90%, 95% and 99% of patients, respectively. Total serum IgE values were significantly associated with the asIgE status of investigated patients. However, these preliminary data warrant further large-scale investigations before total serum IgE levels can be regarded as a clinically useful parameter between patients with extrinsic atopic dermatitis and intrinsic atopic dermatitis. Key words: IgE; children; atopic dermatitis.
(Accepted October 20, 2008.)
Acta Derm Venereol 2009; 89: 257–261.
Hagen Ott, Department of Dermatology and Allergology, University Hospital Aachen, Pauwelsstrasse 30, DE-52074 Aachen, Germany. E-mail: hagen.ott@post.rwth-aachen.de
Atopy has been defined as “a personal or familial tendency to produce IgE antibodies in response to low doses of allergens, usually proteins” (1). In this context, an elevated level of total serum IgE (tIgE) is still considered as a possible indicator of atopic sensitization and a predictor of allergic diseases such as seasonal rhinoconjunctivitis, bronchial asthma or atopic dermatitis (AD) (2).
AD represents one of the most common diseases in childhood, with increasing incidence throughout the last decades and a current cumulative prevalence of up to 20% in Western countries (3, 4). Two clinical patterns of AD have been identified. First, the intrinsic variant of AD (ADi) is observed in 15–45% of patients and characterized by a lack of IgE-mediated sensitization. Accordingly, no allergen-specific IgE antibodies (asIgE) can be determined by in vitro or in vivo diagnostic tools. In contrast, the extrinsic AD type (ADe) occurs in the majority of affected children and is associated with the presence of asIgE against patient-specific patterns of inhalant and/or nutritive allergens. More importantly, both types of AD differ with regard to further immunological parameters, age of onset and clinical phenotypes (5, 6). In particular, patients with ADi develop first symptoms at an earlier age, display a milder disease severity and rarely suffer from additional atopic conditions, especially bronchial asthma (7). Hence, identifying children with IgE-mediated sensitization as the clinical hallmark of ADe is useful for both further diagnostic work-up and effective allergological treatment.
However, very few investigators have discussed tIgE assessment, and its application in adult and paediatric allergy trials has hitherto been limited to the study of bronchial asthma. By contrast, AD has been investigated by only a few research groups (8–10). Thus, it was the aim of the present study to assess the clinical performance of tIgE as a predictor of IgE-mediated sensitization and its possible role to distinguish between the extrinsic and the intrinsic form of AD.
Patients and Methods
Study population
We retrospectively studied a total of 103 consecutive infants and children referred to our interdisciplinary centre of pediatric allergology and pneumology for the evaluation of AD and suspected IgE-mediated hypersensitivity. In all patients, the diagnosis of AD had been established by a paediatric allergologist/dermatologist performing a thorough clinical examination and applying a structured questionnaire adhering to the UK Working Party’s diagnostic criteria for AD (11).
Retrospective data analysis was performed in accordance with ethical standards on human experimentation and with the Declaration of Helsinki of 1975, as revised in 1983.
Laboratory investigations
Venous blood samples of all patients were collected during the first patient visit to our department and the obtained serum probes were aliquoted and stored at –20ºC until further analysis. Determinations of tIgE and asIgE levels were performed with a widely used, commercially available fluorescence enzyme immunoassay (FEIA) as proposed by the manufacturer (UniCAP™, Phadia, Uppsala, Sweden). We assessed asIgE titres against a screening panel of inhalative and nutritive allergen extracts purchased from the same supplier (manufacturer’s code): timothy grass pollen (g6), birch pollen (t3), dermatophagoides pteronyssinus (d1), cat dander (e1), dog dander (e5), egg white (f1), cow’s milk (f2), codfish (f3), wheat (f4), peanut (f13) and soy (f14). Total and specific IgE levels were quantified in protein units designated as kU/l with a lower detection limit of 0.35 kU/l according to the product manual.
Statistics
The presence of asIgE antibodies was used as response variable during logistic regression analysis evaluating its association with tIgE levels and further anamnestic variables, i.e. allergic co-morbidity and family history of parental atopy.
Receiver operating characteristic (ROC) analysis was performed in order to study the effect of varying tIgE thresholds on the numerical outcome of FEIA-based asIgE detection. The corresponding ROC curves were obtained by plotting the true positive rate, i.e. the rate of correctly identified positive asIgE results, against the false positive rate for all possible tIgE cut-off points. As a measure of clinical usefulness, i.e. the test’s performance in separating patients suffering from either ADi or ADe, the according AUC (area under the ROC curve) value was computed for obtained tIgE levels. Sensitivity and specificity with corresponding 95% confidence intervals (CI) as well as positive (PPV) and negative predictive values (NPV) were also calculated using the tIgE cut-off point leading to the highest accuracy, i. e. the maximum value for the sum of sensitivity and specificity.
We determined 90%, 95% and 99% predictive decision points for at least one positive asIgE result at a given tIgE level using the logistic regression analysis method proposed by Sampson (12) employing the formula P = 1/e–α–βx+1, where x is the continuous diagnostic test parameter, P is the probability of a positive asIgE result given the value x, and α and β are the model parameters of the corresponding logistic regression model.
All statistical analyses were performed using the S Plus™ 6.1 statistical software package (Insightful Corp., Seattle, USA), and MedCalc™ Version 6.1.1 (MedCalc Software, Mariakerke, Belgium) was used for plotting of ROC curves.
Results
A total of 103 infants, children and adolescents (53 males, 50 females) with a median age of 35 months (range 3 months–17 years) entered this study. Sixty-three percent of these individuals were considered as atopic, revealing at least one asIgE measurement above 0.35 kU/l, while 38 patients (37%) did not reveal any allergen-specific sensitization. Within the total patient population, 35 children (34%) displayed additional symptoms of food allergy, while allergic rhinitis and bronchial asthma were observed in 31 (30%) and 43 (42%) patients, respectively. A positive parental history of atopy was common as mothers of 46 (45%) and fathers of 36 (35%) patients suffered from bronchial asthma and/or allergic rhinitis. In contrast, a history of maternal or paternal AD was recorded in only 19 (18%) and 14 (13%) children, respectively.
As summarized in Table I, separate analysis of ADe and ADi patients revealed significantly different prevalences of demographic and clinical parameters at median tIgE levels of 224 kU/l (14–12013 kU/l) in the ADe group and 25 kU/l (0–4352 kU/l) in children with the ADi phenotype.
Table I. Demographic and clinical characteristics of the recruited patient population with atopic dermatitis (AD) (n = 103)
| | Extrinsic AD (n = 65) | Intrinsic AD (n = 38) |
| Median age at first visit, months (range) | 44 (4–212) | 23 (3–172) |
| Total serum IgE, kU/l (range) | 224.0 (14–12013) | 25.2 (0–4352) |
| Gender, n (%) |
| Male | 39 (60) | 14 (37) |
| Female | 26 (40) | 24 (63) |
| Atopic co-morbidity, n (%) |
| Food allergy | 31 (48) | 4 (11) |
| Allergic rhinitis | 25 (39) | 7 (18) |
| Asthma | 36 (55) | 7 (11) |
| Family history of atopy, n (%) |
| Maternal asthma ± allergic rhinitis | 30 (46) | 16 (42) |
| Paternal asthma ± allergic rhinitis | 26 (40) | 10 (26) |
| Maternal atopic eczema | 13 (20) | 6 (16) |
| Paternal atopic eczema | 10 (15) | 4 (11) |
Furthermore, assessment of asIgE recognition patterns revealed that the house dust mite extract (D. pteronyssinus) elicited the highest rate of positive results within the group of inhalant allergens (n = 29, 28%), whereas hen’s egg was the most frequently recognized food allergen (n = 37, 36%). The complete data on asIgE prevalence as well as mean asIgE levels for each investigated allergen in patients with asIgE-positive ADe are summarized in Table II.
Table II. Cumulative IgE recognition patterns to inhalant and food allergens in children with extrinsic atopic dermatitis defined by at least one positive allergen-specific IgE antibody test result (n = 65)
| Allergen source (manufacturer’s code) | Prevalence of sensitization (%*) | IgE level (kU/l) Mean (SD) |
| Food allergens |
| Codfish (f3) | 11 (12) | 1.9 (11.1) |
| Cow’s milk (f2) | 24 (23) | 1.61 (7.5) |
| Wheat (f4) | 24 (23) | 2.56 (10.4) |
| Soy (f14) | 25 (24) | 2.0 (19.2) |
| Peanut (f13) | 31 (30) | 4.6 (14.0) |
| Hen’s egg (f1) | 37 (36) | 3.6 (11.1) |
| Inhalant allergens |
| Birch pollen (t3) | 16 (16) | 7.9 (24.7) |
| Timothy grass pollen (g6) | 18 (17) | 6.31 (19.2) |
| Cat dander (e1) | 24 (23) | 8.0 (21.3) |
| Dog dander (e5) | 27 (26) | 5.7 (18.2) |
| D. pteronyssinus (d1) | 29 (28) | 11.31 (28.5) |
*% of total population; SD: Standard deviation
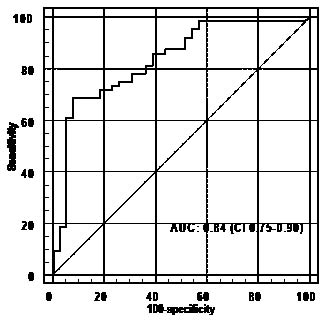
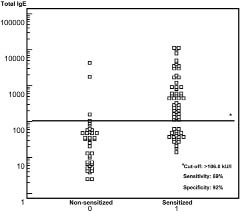
Bivariate logistic regression analysis revealed a statistically significant association between allergen-specific sensitization and atopic co-morbidity, i.e. additional asthma (p = 0.0035), allergic rhinitis (p = 0.0106) and food allergy (p = 0.0004). Total serum IgE-levels were also associated with the presence of specific IgE antibodies (p = 0.0368) while a positive parental history of allergy or AD was not significantly correlated (data not shown). ROC analysis of tIgE levels in sensitized and non-sensitized patients resulted in a tIgE cut-off value of 106 kU/l yielding an optimal value of accuracy with a sensitivity of 68.7% (CI 55.9–79.8) and a specificity of 92.3% (CI 79.1–98.3) while the PPV and the NPV were determined at 93.6% and 64.3%, respectively; the according AUC value was 0.84 (CI 0.75–0.90) (Figs 1 and 2).
Fig. 1. Receiver operating characteristic curve and corresponding area under the curve (AUC) value with corresponding 95% confidence interval (CI). As an established measure of test performance, the obtained AUC value (0.84) reflects the potential of total tIgE serum levels to differentiate between patients with extrinsic and intrinsic atopic dermatitis.
Fig. 2. Distribution of total tIgE antibody levels in patients with sensitized and non-sensitized atopic dermatitis. The line represents tIgE serum cut-off value obtained by receiver operating characteristic analysis.
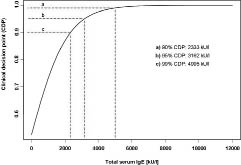
We additionally calculated clinical decision points (CDP) for a positive outcome of asIgE analysis that have been considered valuable parameters in other clinical settings, particularly in the diagnosis of paediatric food allergy (12, 13). As a result, FEIA tIgE data predictive of positive asIgE results in 90%, 95% and 99% of patients could be identified and are demonstrated in Fig. 3.
Fig. 3. Clinical total serum immunoglobulin E (tIgE) decision points (CDP) predictive of at least one positive allergen-specific IgE result in 90%, 95% and 99% of investigated patients.
Discussion
Although serum IgE antibodies represent only a very small fraction of the entire human immunoglobulin repertoire, they play an important clinical role and can be regarded as one of the key features of atopic disease pathogenesis in both children and adults (14). Accordingly, tIgE levels have been identified as clinically useful parameters in adult-onset asthma indicating airway hyperresponsiveness in a dose-dependent pattern (15). Furthermore, several investigators described an age-related relationship between a pathological methacholine challenge and tIgE titres in asthmatic children (16). Surprisingly, only very few studies have assessed the role of tIgE in childhood AD, and have focused mainly on the link between tIgE and disease severity (8, 9, 17). Nevertheless, tIgE levels are frequently raised in this population and they are still used as a parameter to discern ADe from ADi in routine patient management (18).
In our study, 63% of the investigated children revealed at least one inhalant or nutritive sensitization and were therefore regarded as having ADe, while 37% where classified as ADi patients. This is in accordance with previous reviews describing an ADe frequency of 55–70% in most paediatric studies, although higher prevalences have been observed depending on the analysed patient population (5, 19). Moreover, 34% of our patients suffered from additional symptomatic food allergy, which is in agreement with previous investigations including hospital-based groups of children suffering from AD, although lower prevalences have been reported in other clinical settings (20, 21). The comparatively high prevalence of concurrent bronchial asthma (41%) was most probably due to the fact that our outpatient clinic is also specialized in paediatric asthma care, which might have caused a certain patient selection bias.
Specific IgE sensitization patterns of included ADe patients corresponded to the results of other paediatric AD trials, particularly with regard to house dust mite as the dominating inhalant allergen and hen’s egg as one of the principal allergenic food proteins (22, 23). Interestingly, the association of allergen-specific sensitization with concurrent atopic diseases such as asthma (p = 0.0035), allergic rhinitis (p = 0.0106) and food allergy (p = 0.0004) was highly significant. This clearly strengthens the concept of ADe as a characteristic clinical syndrome consisting of eczema, IgE-mediated sensitization and additional allergic conditions. In this regard, established and widely-used classifications of AD, such as the UK Working Party’s diagnostic criteria employed in this investigation, obviously lack the necessary discriminatory power to distinguish between phenotypically similar intrinsic and extrinsic disease courses. Yet, our data clearly support the notion of ADi as a distinct clinical entity, also termed “atopiform dermatitis” by other study groups, which is associated with significantly less atopic co-morbiditiy, lower numbers of atopic first-degree relatives and an earlier age of onset compared with ADe. Hence, more specific diagnostic criteria incorporating allergen-specific IgE as a mandatory criterion should be developed to facilitate future genetic and therapeutic studies with well-defined, homogenous patient populations of either ADe or ADi patients (7).
Similarly, our analyses revealed a significant correlation of tIgE levels and positive asIgE test results (p = 0.0368), which has also been observed previously in adult patients with AD and house dust mite sensitization (24). For further clarification, ROC curves were employed to investigate the ability of tIgE to differentiate truly positive (sensitized) patients with an elevated tIgE test result from truly negative (non-sensitized) patients without raised tIgE levels. As a result, the identified tIgE cut-off was associated with low sensitivity (68.7%) and high specificity (92.3%). The overall test performance appeared adequate as indicated by an elevated AUC value (0.84). These results are corroborated by Perkin and co-workers, who studied a population-based birth cohort and were able to demonstrate that a tIgE cut-off > 51 kU/l at the age of 12 months determined specific IgE-mediated sensitization with a sensitivity of 22.0% and a specificity of 95.8% (2). At first glance, these data imply that tIgE values exceeding the described cut-off levels are able to confirm a suspected allergen-specific sensitization, whereas tIgE levels below this value do not exclude atopic sensitization due to a low degree of sensitivity.
Still, with regard to additional diagnostic steps and further therapeutic interventions, the major function of tIgE screening in daily clinical practice should consist in reliably discerning ADe from ADi in a maximum number of patients. In this regard, positive predictive values, which could also be computed for tIgE levels detected in our study, are known to depend critically on symptom prevalence in the tested patient population. Hence, we additionally calculated clinical decision points indicating the amount of tIgE that is associated with a pre-chosen probability of positive asIgE measurements. This approach has been chosen previously by us and several other study groups to predict clinical reactivity in children with suspected food allergy (12, 13, 25, 26). To the best of our knowledge, however, determination of clinical decision points has never been performed with tIgE levels predicting the asIgE status in children with AD.
Intriguingly, the obtained tIgE thresholds for a probability of 90% (2333 kU/l), 95% (3162 kU/l) and 99% (4995 kU/l) were found to be extremely high, which might be attributable to the general propensity of AD patients to develop strongly elevated tIgE levels. This would be in line with the maximum tIgE values observed in both ADi (4352 kU/l) and ADe (12.013 kU/l) patients included in the current investigation. Yet, these results have to be interpreted with caution since tIgE reference values have been shown to be influenced by a comprehensive set of clinical variables, such as patient age (27), disease severity (8, 9), atopic co-morbidity (14) or the choice of IgE detection methods employed for in vitro or in vivo testing (28).
Of note, elevated tIgE values in both ADe and ADi demonstrate that individual IgE repertoires are not composed of allergen-specific IgE antibodies alone. Thus, patient-inherent determinants apparently influence tIgE homeostasis in affected patients. In this context, recent genomic studies have identified susceptibility genes predisposing to elevated tIgE levels irrespective of allergen-specific sensitization. Most importantly, polymorphisms within the high-affinity IgE receptor (FCεRI) gene have been found to be associated with the synthesis of unspecific IgE antibodies in high quantities and with unknown function (29). Furthermore, genetically determined cornification defects, such as loss-of-function mutations within the filaggrin gene, are likely to predispose for an impaired epidermal barrier function and secondary IgE synthesis in patients with AD (30).
In conclusion, the results of our study suggest that there is a statistical association between IgE levels and the presence of asIgE antibodies in children with AD. In addition, clinical tIgE decision points predicting atopic sensitization can be calculated in this group of patients. However, the limited sample size in the present study hampers the extrapolation of our findings to other patients. Therefore, we believe that these preliminary data have to be validated in further large-scale studies or systematic reviews of previously published data before tIgE levels can be regarded as a clinically useful differentiator between the extrinsic and the intrinsic variant of AD.
The authors declare no conflict of intetest.
References
1. Johansson SG, Hourihane JO, Bousquet J, Bruijnzeel-Koomen C, Dreborg S, Haahtela T, et al. A revised nomenclature for allergy. An EAACI position statement from the EAACI nomenclature task force. Allergy 2001; 56: 813–824.
2. Perkin MR, Strachan DP, Hc W, Lack G, Golding J; ALSPAC Study Team. The predictive value of early life total immunoglobulin E measurement in identifying atopic children in a population-based birth cohort study. Pediatr Allergy Immunol 2006; 17: 118–124.
3. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. Lancet 1998; 351: 1225–1232.
4. Asher MI, Montefort S, Bjorksten B, Lai CK, Strachan DP, Weiland SK, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet 2006; 368: 733–743.
5. Park JH, Choi YL, Namkung JH, Kim WS, Lee JH, Park HJ, et al. Characteristics of extrinsic vs. intrinsic atopic dermatitis in infancy: correlations with laboratory variables. Br J Dermatol 2006; 155: 778–783.
6. Kusel MM, Holt PG, de Klerk N, Sly PD. Support for 2 variants of eczema. J Allergy Clin Immunol 2005; 116: 1067–1072.
7. Brenninkmeijer EE, Spuls PI, Legierse CM, Lindeboom R, Smitt JH, Bos JD. Clinical differences between atopic and atopiform dermatitis. J Am Acad Dermatol 2008; 58: 407–414.
8. Laske N, Niggemann B. Does the severity of atopic dermatitis correlate with serum IgE levels? Pediatr Allergy Immunol 2004; 15: 86–88.
9. Hon KL, Lam MC, Leung TF, Wong KY, Chow CM, Fok TF, et al. Are age-specific high serum IgE levels associated with worse symptomatology in children with atopic dermatitis? Int J Dermatol 2007; 46: 1258–1262.
10. Ohman S, Johansson SG. Allergen-specific IgE in atopic dermatitis. Acta Derm Venereol 1974; 54: 283–290.
11. Williams HC, Burney PG, Pembroke AC, Hay RJ. Validation of the U.K. diagnostic criteria for atopic dermatitis in a population setting. U.K. Diagnostic Criteria for Atopic Dermatitis Working Party. Br J Dermatol 1996; 135: 12–17.
12. Sampson HA. Utility of food-specific IgE concentrations in predicting symptomatic food allergy. J Allergy Clin Immunol 2001; 107: 891–896.
13. Garcia-Ara MC, Boyano-Martinez MT, Díaz-Pena JM, Martín-Muñoz MF, Martín-Esteban M. Cow’s milk-specific immunoglobulin E levels as predictors of clinical reactivity in the follow-up of the cow’s milk allergy infants. Clin Exp Allergy 2004; 34: 866–870.
14. Wuthrich B, Schmid-Grendelmeier P. The atopic eczema/dermatitis syndrome. Epidemiology, natural course, and immunology of the IgE-associated (“extrinsic”) and the nonallergic (“intrinsic”) AEDS. J Investig Allergol Clin Immunol 2003; 13: 1–5.
15. Jaakkola MS, Ieromnimon A, Jaakkola JJ. Are atopy and specific IgE to mites and molds important for adult asthma? J Allergy Clin Immunol 2006; 117: 642–648.
16. Kono M, Mochizuki H, Arakawa H, Kato M, Tokuyama K, Morikawa A. Age-dependent relationship between bronchial hyperresponsiveness to methacholine and total serum IgE level in asthmatic children. Ann Allergy Asthma Immunol 2001; 87: 33–38.
17. Aral M, Arican O, Gul M, Sasmaz S, Kocturk SA, Kastal U, et al. The relationship between serum levels of total IgE, IL-18, IL-12, IFN-gamma and disease severity in children with atopic dermatitis. Mediators Inflamm 2006; 2006: 73098.
18. Akdis CA, Akdis M, Bieber T, Bindslev-Jensen C, Boguniewicz M, Eigenmann P, et al. Diagnosis and treatment of atopic dermatitis in children and adults: European Academy of Allergology and Clinical Immunology/American Academy of Allergy, Asthma and Immunology/PRACTALL Consensus Report. J Allergy Clin Immunol 2006; 118: 152–169.
19. Schmid-Grendelmeier P, Simon D, Simon HU, Akdis CA, Wüthrich B. Epidemiology, clinical features, and immunology of the “intrinsic” (non-IgE-mediated) type of atopic dermatitis (constitutional dermatitis). Allergy 2001; 56: 841–849.
20. Schäfer T. The impact of allergy on atopic eczema from data from epidemiological studies. Curr Opin Allergy Clin Immunol 2008; 8: 418–422.
21. Werfel T, Breuer K. Role of food allergy in atopic dermatitis. Curr Opin Allergy Clin Immunol 2003; 4: 379–385.
22. Kemp AS. Egg allergy. Pediatr Allergy Immunol 2007; 18: 696–702.
23. Kramer U, Lemmen C, Bartusel E, Link E, Ring J, Behrendt H. Current eczema in children is related to Der f 1 exposure but not to Der p 1 exposure. Br J Dermatol 2006; 154: 99–105.
24. Hansen SK, Deleuran M, Johnke H, Thestrup-Pedersen K. House dust mite antigen exposure of patients with atopic dermatitis or psoriasis. Acta Derm Venereol 1998; 78: 139–141.
25. Celik-Bilgili S, Mehl A, Verstege A, Staden U, Nocon M, Beyer K, et al. The predictive value of specific immunoglobulin E levels in serum for the outcome of oral food challenges. Clin Exp Allergy 2005; 35: 268–273.
26. Ott H, Baron JM, Heise R, Ocklenburg C, Stanzel S, Merk HF, et al. Clinical usefulness of microarray-based IgE detection in children with suspected food allergy. Allergy 2008; 63: 1521–1528.
27. Kulig M, Tacke U, Forster J, Edenharter G, Bergmann R, Lau S, et al. Serum IgE levels during the first 6 years of life. J Pediatr 1999; 134: 453–458.
28. Hamilton RG, Adkinson NF, Jr. 23. Clinical laboratory assessment of IgE-dependent hypersensitivity. J Allergy Clin Immunol 2003; 111: S687–S701.
29. Potaczek DP, Sanak M, Mastalerz L, Milewski M, Gawlewicz-Mroczka A, Szczeklik A. Genetic polymorphisms of the novel FCERIA gene region: relation to total serum IgE levels. Ann Allergy Asthma Immunol 2007; 98: 500–501.
30. Weidinger S, Illig T, Baurecht H, Irvine AD, Rodriguez E, Diaz-Lacava, et al. Loss-of function variations within the filaggrin gene predispose for atopic dermatitis with allergic sensitizations. J Allergy Clin Immunol 2006; 118: 214–219.