Philipp Rehberger1,2, Petra Beckheinrich-Mrowka1, Uwe-Frithjof Haustein1 and Michael Sticherling1,3
1Department of Clinical and Experimental Dermatology, University of Leipzig, Leipzig, 2Department of Dermatology, Technical University of Dresden, Dresden, and 3University of Erlangen, Erlangen, Germany
Systemic sclerosis is a connective tissue disorder with unclear aetiology and pathogenesis. However, there is evidence that microvascular changes belong to the early symptoms of the disease. These are associated with increased serum levels of markers of endothelium activation, such as adhesion molecules and growth factors. The stable prostacyclin analogue iloprost is licensed for vascular symptoms (Raynaud’s phenomenon) and was recently shown to exert short-term effects on these markers. In this study, serum samples (n = 13) from patients with systemic sclerosis were examined for serum levels of vascular cell adhesion molecule-1 (VCAM-1), intercellular cell adhesion molecule-1, E-selectin, endothelin-1 and vascular endothelial growth factor over 6 months after iloprost infusions in order to detect possible long-term effects. Iloprost significantly reduced initially elevated levels of these markers, partly until the end of the observation period (E-selectin, VCAM-1, endothelin-1). These effects provide serological evidence for the benefits of iloprost infusions that are seen clinically in patients with systemic sclerosis. Key words: scleroderma; Raynaud’s phenomenon; adhesion molecules; prostacyclin; iloprost.
(Accepted December 1, 2008.)
Acta Derm Venereol 2009; 89: 245–249.
Philipp Rehberger, Department of Dermatology, Technical University of Dresden, Fetscherstr. 74, DE-01307 Dresden, Germany. E-mail: Philipp.Rehberger@uniklinikum-dresden.de
Systemic sclerosis (SSc) is a generalized connective tissue disorder characterized by a wide spectrum of microvascular, fibrotic and immunological abnormalities with as-yet incompletely understood pathogenesis. Vascular complaints such as Raynaud’s phenomenon are common and early symptoms in SSc (1). They may precede fibrosis for long periods, thereby hinting at the substantial involvement of endothelial cells in the pathology of SSc (2). Auto-antibodies and other factors that have not yet been clearly identified lead to damage of endothelial cells and vascular leakage with subsequent tissue oedema (3). Activated endothelial cells in turn will upregulate the expression of adhesion molecules on their cell surfaces to recruit immune cells and to release fibroblast-activating mediators. High levels of soluble adhesion molecules, such as intercellular adhesion molecule 1 (sICAM-1), vascular adhesion molecule 1 (sVCAM 1), E-selectin and P-selectin, have been detected in patients with SSc (4). They show a positive correlation with their in situ expression in lesional skin as well as the clinical disease severity (5). Therefore, these parameters might be used for the observation of the disease course and its progression.
Iloprost represents a stable prostacyclin analogue and has been shown to reduce the number, duration and severity of attacks and to improve acral ischaemic ulcers (6). Furthermore, a significant change in the serum levels of adhesion molecules could be detected shortly after infusions with iloprost (7). Whether these effects are transient or long-lasting has not been clarified. The aim of the present study was to investigate the long-term effects of iloprost infusions on disease activity related factors such as expression of soluble adhesion molecules in patients with SSc.
MATERIALS AND METHODS
Patient selection and clinical data
Six consecutive serum samples were obtained from 13 patients (Table I) before, immediately after, and 1, 2, 3 and 6 months after the last administration of iloprost (Ilomedin®, Schering, Berlin, Germany). Patients received intravenous infusions of iloprost over a period of 6-h each day for 5–7 days (0.5–2.0 ng/kg bodyweight/min; altogether 50 μg iloprost per day) for Raynaud’s phenomenon (12/13 patients) and digital ulcers (7/13 patients). Three patients decided to withdraw before the end of the study due to personal reasons not related to the medication. The patients with SSc fulfilled the criteria defined by the American College of Rheumatology and did not exhibit diagnostic features of other connective tissue diseases. All patients had the limited cutaneous form of SSc according to the classification proposed by LeRoy et al. (8). All patients were female with a median (± standard deviation) age of 59.8 ± 15.5 (range 34–78) years.
Table I. Clinical and laboratory data of female patients with limited cutaneous systemic sclerosis and Raynaud’s phenomenon in order of increasing age
| Patient | Age (years) | Duration of disease (years) | Internal organ involvement | Digital ulcers | ANA titre | ATA | ACA | RPIII | Concomitant diseases | Concomitant medication (remained stable during follow-up period) |
| 1 | 34 | 15 | – | + | 1:10,000 | – | + | – | – | Isradipine, imidapril |
| 2 | 34 | 15 | – | + | 1:10,000 | – | + | – | – | – |
| 3 | 35 | 16 | – | + | 1:40,000 | – | + | – | – | Isradipine, imidapril, beraprost |
| 4 | 52 | 35 | P, G, C | + | 1:1,280 | – | – | – | Arterial hypertension | Pentoxifylline, molsidomine, piretanide, metoclopramide, valsartan, hydrochlorothiazide |
| 5 | 61 | 21 | C | + | 1:10,000 | – | + | – | Hypothyroidism | Levothyroxine |
| 6 | 64 | 2 | P | – | 1:2,500 | – | – | – | Osteoporosis | Levothyroxine, risedronic acid, calcium |
| 7 | 64 | 12 | G | – | 1:10,000 | – | + | – | – | Omeprazole, pentoxifylline |
| 8 | 65 | 13 | P, G | – | 1:10,000 | – | + | – | – | Omeprazole, pentoxifylline |
| 9 | 68 | 41 | P | – | 1:40,000 | – | + | – | Arterial hypertension | Bisoprolol |
| 10 | 69 | 42 | P | – | 1:40,000 | – | + | – | Arterial hypertension, depression | Bisoprolol, trimipramine |
| 11 | 77 | 42 | P | – | – | – | – | – | – | Pentoxifylline, losartan |
| 12 | 77 | 34 | P, G | + | 1:640 | + | – | – | Leg ulcer, osteoporosis | Nifedipine, losartan, calcium, magnesium, vitamin E |
| 13 | 78 | 35 | P, G | + | 1:1,280 | + | – | – | Osteoporosis, mitral valve insufficiency | Nifedipine, losartan |
P: pulmonary; G: gastrointestinal; C: cardiac; ANA: antinuclear antibody; ATA: anti-topoisomerase-I-antibody; ACA: anti-centromere antibody; RPIII: RNA polymerase III.
Detection of circulating adhesion molecules
Circulating sICAM-1, sVCAM-1, sE-selectin, vascular endothelial growth factor (VEGF) and endothelin-1 (ET-1) were measured by quantitative sandwich enzyme immunoassay technique using commercial immunoassay kits (R&D, Oxford, UK) according to the manufacturer’s instructions. A standard curve and positive control samples were included in each test. Serum levels (95% confidence intervals (95% CI)) in control samples from healthy adults as stated by the manufacturer’s manual using these assay kits were used as reference values: sICAM-1: 115–306 ng/ml (mean value: 211 ng/ml); sVCAM-1: 395–714 ng/ml (mean value: 553 ng/ml); sE-selectin: 29.1–63.4 ng/ml (mean value: 46.3 ng/ml); VEGF: 62–707 pg/ml (mean value: 220 pg/ml) and human ET-1: 0.71–2.3 pg/ml (mean value: 1.2 pg/ml). The lower detection limit for sICAM-1 is less than 0.35 ng/ml, for sVCAM-1 2.0 ng/ml, for sE-selectin 0.1 ng/ml; for VEGF 9.0 pg/ml and for human ET-1 0.16 pg/ml.
Statistical analysis
Statistical analysis was carried out using the Friedman test to detect differences of samples of all time-points (significant for p-values F = p < 0.05) and the Wilcoxon rank-sum test to detect differences between 2 time-points. p-values < 0.05 were considered significant (*p < 0.05; #p < 0.005; +p < 0.0005).
RESULTS
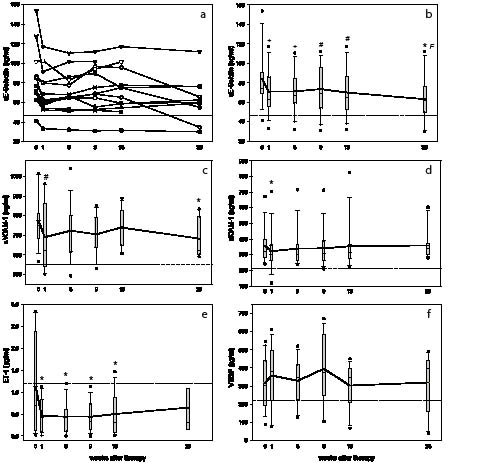
All patients tolerated the iloprost infusion therapy well. The most common side-effects were flushing and headache, which disappeared after dose reduction. A considerable variation in serum concentration and time course for each parameter and patient could be observed (shown in Fig. 1a for E-Selectin). Therefore, box plot-graphs were used for presentation of the data (Fig. 1b–f). Results are shown as means for duplicate wells. The serum concentration of sE-Selectin (Fig. 1b), sVCAM-1 (Fig. 1c), and sICAM-1 (Fig. 1d) were distinctly elevated before therapy and were significantly reduced by therapy for at least 2 months as in the case of sICAM-1. For sE-selectin and sVCAM-1, the concentrations were still significantly reduced after 6 months compared with before treatment. Concentrations of ET-1 (Fig. 1e) showed a wide range across individuals with the mean close to the reference value of healthy volunteers. ET-1 levels showed a significant decrease following therapy, which was still detectable after 13 weeks. Elevated concentrations of VEGF (Fig. 1f) tended to be slightly raised after therapy but remained generally unaffected. There was no correlation between either the involvement of internal organs or the specificity or with titres of the autoantibody or serum levels of the evaluated serological parameters. All 12 of 13 patients reported a reduction in the frequency and severity of Raynaud’s phenomenon and 6 of 7 patients reported a decreased size of digital ulcers.
Fig. 1. (a–f) Iloprost significantly reduces the serum levels of adhesion molecules for a long period, whereas serum levels of vascular endothelial growth factor (VEGF) remain unaffected. (a) Individual data for E-selectin from the 13 patients in the study. (b) Box plot presentation of E-selectin. (c) Soluable vascular adhesion molecule 1 (sVCAM-1). (d) Soluable intercellular adhesion molecule 1 (sICAM-1). (e) Endothelin-1 (ET-1). (f) VEGF. Mean value of healthy volunteers (---) and mean of patients (–). Statistical significances refer to the first value before therapy (Wilcoxon test: +p < 0.0005, #p < 0.005, *p < 0.05) and to all time-points (Friedman test: F = p < 0.05).
DISCUSSION
Raynaud’s phenomenon is regarded as a clinical manifestation of disturbed vascular function and a frequent and early feature of SSc (1–3). The activation of endothelial cells by auto-antibodies and other unidentified mechanisms leads to increased expression of adhesion molecules on the cell surface. These are also detectable in soluble form in the serum (4). E-selectin is only expressed and released by activated endothelial cells under the influence of pro-inflammatory enzymes.VCAM-1 can also derive from epithelial cells, dendritic cells and macrophages, whereas ICAM-1 can be synthesized by epithelial cells, granulocytes, hepatocytes and smooth muscle cells. Altogether, serum levels of these adhesion molecules have been shown to correlate with inflammatory activity of SSc as measured by erythrocyte sedimentation rate and leukocyte count and clinical disease activity (4, 5).
The stable prostacyclin analogue iloprost is well established in the treatment of Raynaud’s phenomenon in SSc (6, 9) and has previously been shown to be effective in our own studies (7). The mechanism of action is explained by its vasodilatory effect on arteries and veins, by inhibition of the adenosine diphosphate-dependent platelet aggregation, by anti-thrombotic and fibrinolytic as well as anti-fibrotic effects and by reduction of the release of vasoconstrictory mediators and anti-inflammatory activity (10). The effect of iloprost on the Raynaud‘s phenomenon is remarkable. The mechanisms of persisting clinical improvement for several weeks have, however, not been studied until now.
In accordance with the findings of other investigations (4, 7), our patients exhibited increased serum concentrations of soluble adhesion molecules ICAM-1, VCAM-1 and E-selectin before therapy that could be significantly decreased by treatment with iloprost. This might reflect the reduced activation of endothelial cells with resulting lower expression of adhesion molecules and decreased production of cytokines (10). Consecutively, lymphocyte migration into adjacent tissue is reduced, which adds to the beneficial clinical effects (11). We were able to show that this decrease of adhesion molecules is not only a short-time and limited effect, but is persisting for a longer period of time. Serum concentrations of sE-Selectin and sVCAM-1 were seen to be decreased as long as 6 months after infusion. However, clinical symptoms of Raynaud‘s phenomenon generally improve during warmer periods of the year and patients may suffer less severely and frequently from their SSc. Since in this study the last serum aliquots were taken in early summer, seasonal effects have to be taken into account in the reduction of circulating adhesion molecules.
Other factors possibly involved in the pathogenesis of SSc include modulation of the vascular tonus mediated by both vasodilators (e.g. prostaglandin) and vasoconstrictors (endothelin) (1, 12). This could be interpreted as a vasotonic imbalance in favour of vasoconstriction. ET-1 is one of the most potent vasoconstrictors and was shown to affect the proliferation of fibroblasts and the synthesis of proteins of the extracellular matrix (13). Furthermore, it is able to modulate fibroblast function and increase their surface expression of ICAM-1. In patients with SSc, increased levels of ET-1 were found in the serum and in the bronchoalveolar lavage, with a possible connection between ET-1 blood levels and the extent of microvascular damage in SSc (14). The mean level of ET-1 in our patients was close to the reference value for healthy volunteers established by the manufacturer. However, levels of ET-1 were significantly reduced following therapy, which confirms the results of our previous study (7). We were able to demonstrate that this decrease in ET-1 persists for an extended period of time up to the end of the study period after 6 months.
A disturbed angiogenesis is yet another possible pathogenic factor of SSc. In healthy skin, angiostatic (e.g. endostatin) and angiogenic factors (e.g. VEGF, transforming growth factor (TGF)-β) are kept in balance (1–3). An imbalance in favour of the latter was found in physiological wound healing and malignant tumours. In SSc, perivascular infiltration and loss of capillaries lead to a decreased blood flow, ischaemia and resulting clinical manifestations such as ”rat bite” necrosis followed by insufficiency of angiogenesis. Clinical states such as hypoxia normally induce angiogenesis, which was, however, found to be decreased or absent in SSc (2). Contrary to our previous study (7), data from other groups (15) as well as our own present findings showed elevated serum concentrations of VEGF that are in line with increased concentrations of potent inducers of VEGF, such as TGF-β found in SSc. These findings suggest that angiogenesis is not sufficiently activated despite the presence and even elevation of VEGF (2). Iloprost was shown to further elevate VEGF concentrations. This increase might be able to equalize the imbalance between angiostatic and angiogenic factors and to induce sufficient angiogenesis.
Taken together, our study has shown that one cycle of 5–7 daily infusions of iloprost is capable of influencing parameters of disease activity and possibly the clinical course of SSc, not only for a short time after therapy, but for up to 6 months, depending on the parameter measured. Differences in the duration of effects for each marker could be explained by different mechanisms of their induction and modulation as well as by the clinical heterogeneity and different stages of disease among patients enrolled in this study. Altogether, however, these results provide further support for the clinical benefits of iloprost infusions in patients with SSc.
Acknowledgement
This work was supported partly by Schering, Germany, now Bayer Healthcare Germany.
REFERENCES