Adrian Heaps1, Nashat Hanna2, Margaret Stanley3 and Peter Goon3*
1Department of Immunology, St Mary’s Campus, Norfolk Place, Imperial College, 2Department of Genito-urinary Medicine, St Mary’s Hospital, London, and 3Department of Pathology, University of Cambridge, Tennis Court Road, Cambridge CB2 1QP, UK. *E-mail: pg336@cam.ac.uk
Accepted December 1, 2008.
Sir,
Human papillomavirus (HPV) is the causative agent of certain benign and malignant tumours. HPV subtypes 6 and 11 cause approximately 90% of cases of genital warts (the most common sexually transmitted disease) (1, 2) and virtually all cases of recurrent respiratory papillomatosis (3, 4). They are classified as low-risk for carcinogenesis, whilst the high-risk subtypes, such as 16 and 18, cause approximately 70% of cases of cervical cancer worldwide (5, 6). There has been intense public interest recently in the HPV prophylactic vaccines for the prevention of cervical cancer (7, 8).
Since HPV infection is primarily a peripheral infection (and not a systemic one), the study of the immune response at the site of infection is a necessity in understanding and designing better therapies. We have examined the feasibility of studying the lymphocytes infiltrating ano-genital warts as a model for studying HPV infection and associated immune responses in the periphery.
Material and Methods
Ano-genital warts were surgically excised as part of treatment for patients attending a wart clinic in St Mary’s Hospital, London. All worts were processed within 2 h of excision. Patients were randomly selected from this clinic and gave informed written consent for their samples to be used, under existing ethical approval from the local ethics committee. A standard enzyme digestion protocol (9) with 70-micron filtration to retrieve cells was compared with a mechanized tissue dissociator (BD Medimachine™, Becton-Dickinson, Oxford, UK), used according to the manufacturer’s instructions. Twenty samples were analysed for each technique and wart-infiltrating lymphocytes were counted via a haemocytometer with Trypan Blue staining. Several samples were subjected to flow cytometric analyses for common lymphocyte cell markers such as CD3, CD4, CD8, gamma-delta receptor, etc. All antibodies were purchased from Becton Dickinson UK. Flow cytometry was performed on a Beckman-Coulter XL machine (Beckman-Coulter, Bedfordshire, UK) and analyses were performed using Coulter Expo 32 software.
RESULTS
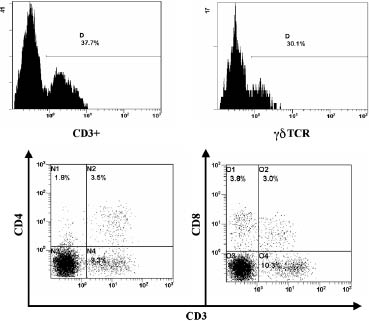
The total cell numbers retrieved for each group of 20 samples treated by the two methods were: (i) enzyme digestion (range 40,000–36,800,000), median = 2,852,350; and (ii) machine dissociation (range 205,000–20,000,000), median = 2,669,875. All samples showed less than 5% cell death with trypan blue staining. Using the non-parametric Mann-Whitney U test (2-tailed test), the median values between the 2 groups did not differ significantly p = 0.73623. The time taken for each protocol was, however, different, with approximately 1.5 h for enzyme digestion and lymphocyte harvesting, compared with 0.5 h for machine dissociation. Flow cytometry further revealed that it was possible to determine phenotypic markers for some of these cells (Fig. 1) using either method. Prolonged enzyme digestion or machine processing resulted in decreased cell numbers and staining (data not shown).
Fig. 1. The top two panels show the presence of CD3+ T cells and gdTCR+ cells within cells extracted from warts from one patient (enzyme digestion). Double staining was not available. The bottom two panels demonstrate the isolation of typical CD4+ and CD8+ T cells from the warts of another patient (machine dissociation). D = Gated on positive cells.
DISCUSSION
We show here that mechanized tissue dissociation of warts is a more efficient method than a standard enzyme digestion protocol and it enabled us to retrieve sufficient cells from some lesions for further analytical studies, such as with flow cytometry or cell culture.
The study of cellular immune responses in HPV infection, particularly in warts, has been relatively neglected in recent years (10). Treatment for HPV infection is primarily through ablative methods that have high recurrence rates (11). The advent of a quadrivalent prophylactic HPV vaccine (Gardasil™) will help to prevent wart infections in the future but does not increase the range of therapeutic options. We suggest that the protocols described above will be valuable tools for the study of the commonest sexually transmitted disease, HPV genital warts, for the delineation of important immune parameters and will thus aid in the design of better immunotherapy and vaccines for HPV diseases.
ACKNOWLEDGEMENTS
This work was supported by the British Skin Foundation. One of the authors (PG) is also supported by Cancer Research UK and both MS and PG by an unrestricted educational grant from Sanofi Pasteur MSD.
Conflict of interest: PG and MS act as consultants to Sanofi Pasteur MSD, Lyon, France. MS also acts as consultant to Merck Research Laboratories, Westpoint, USA and GSK Biologicals, Rixensart, Belium.
REFERENCES