Camilla Hörfelt1, Bo Stenquist1, Christina B. Halldin1, Marica B. Ericson1,2 and Ann-Marie Wennberg1
1Department of Dermatology, Sahlgrenska University Hospital and 2Department of Physics, Göteborg University, Göteborg, Sweden



Camilla Hörfelt1, Bo Stenquist1, Christina B. Halldin1, Marica B. Ericson1,2 and Ann-Marie Wennberg1
1Department of Dermatology, Sahlgrenska University Hospital and 2Department of Physics, Göteborg University, Göteborg, Sweden
This controlled study investigated single low-dose red light photodynamic therapy and methyl-aminolevulinate (MAL) for treatment of moderate to severe facial acne in 19 patients. The right cheek was treated with MAL (160 mg/g) for 3 h prior to illumination. The left cheek received red light only. Both cheeks were illuminated with narrow-band red light (635 nm) at a light dose of 15 J/cm2. The global severity of acne was assessed at baseline and at follow-up, 10 and 20 weeks after treatment. Fluorescence images, clinical photographs and skin surface biopsies were obtained. Both MAL-photodynamic therapy and control areas showed a significant decrease in acne score at follow-up; no significant difference was found compared with control. MAL-photodynamic therapy was associated with adverse effects such as erythema and stinging. Fluorescence images revealed poor selectivity of MAL-induced fluorescence to the acne lesions, suggesting a general photoablating mechanism rather than selective destruction of sebaceous glands. No significant reduction in Propionibacterium acnes or sebum excretion was found. Key words: acne; fluorescence imaging; methyl-aminolaevulinic acid; photodynamic therapy; Propionibacterium acnes; sebum.
(Accepted March 2, 2009.)
Acta Derm Venereol 2009; 89: 372–378.
Camilla Hörfelt, Department of Dermatology, Sahlgrenska University Hospital, Göteborg University, SE-413 45 Göteborg, Sweden. E-mail: camilla.s.horfelt@vgregion.se
Acne vulgaris affects 80% of the population at some time between the ages of 11 and 30 years (1). The anaerobic skin bacteria Propionibacterium acnes is implicated in the pathophysiology of acne vulgaris (2); however, the relationship between P. acnes and acne vulgaris is complex (3). Local therapy is often not sufficient for treatment of acne, and oral antibiotics are of limited value due to antibiotic-resistant P. acnes strains (4). Furthermore, many patients do not tolerate oral treatment with isotretinoin due to severe side-effects (5). Hence there is a need for development of alternative treatment modalities for acne.
There are many studies showing that light therapy has a positive effect on acne lesions (6–9). The mechanism of action appears to involve photodestruction of P. acnes following light exposure. P. acnes has an endogenous production of porphyrins (mainly coproporphyrins) (10–12). Photoactivation of porphyrins causes the formation of singlet oxygen and reactive radicals, which may kill the bacteria. Both blue and red light can be used for photoactivation; however, red light is used preferentially because of its better penetration into tissue (9).
Topical photodynamic therapy (PDT) is used for treatment of precancerous lesions and skin cancers (13). By topical application of 5-aminolevulinic acid (ALA) or its methylester methyl-aminolevulinate (MAL) elevated photosensitization is obtained. ALA or MAL is metabolized to protoporphyrin IX (PpIX) and in combination with red light singlet oxygen is produced, killing the tumour cells. Several studies have shown efficacy in using topical PDT for treatment of acne (14–17). The mode of action for PDT of acne is thought to be that ALA or MAL is taken up by the pilosebaceous unit (10). Thus PDT is believed to have a specific effect on the sebaceous glands (10, 12); however, the complete mechanism behind PDT of acne is not yet fully understood.
In a previous dose-finding study by our group, a low light dose was found to be preferable when performing ALA-PDT for treatment of acne (18), since the lower light dose was associated with far fewer side-effects. MAL-PDT has previously been shown to be effective in the treatment of acne (19) using two consecutive MAL-PDTs at 37 J/cm2, performed 2 weeks apart, but there is a lack of studies investigating the effect of single session MAL-PDT. The aim of the present split-face controlled study was to investigate the efficacy of a single topical MAL-PDT in patients with moderate to severe facial acne. Fluorescence imaging has been used as a monitoring tool to study the amount of endogenous porphyrins produced by P. acnes, and to evaluate photosensitization after application of MAL. In addition, we determined whether the quantities of sebum excretion and P. acnes were affected by MAL-PDT.
METHODS
Patients
A total of 23 patients (9 men, 14 women; age range 19–37 years) with moderate to severe inflammatory facial acne vulgaris (Pillsbury grade II–III) (20) and Fitzpatrick skin type I–III were enrolled in a prospective controlled study. The study was performed according to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the local ethics committee. All subjects provided written informed consent before any study-related procedure was undertaken.
None of the patients had been treated previously with oral isotretinoin. Systemic antibiotics were discontinued for one month and topical treatments for at least 2 weeks prior to the study. These wash-out periods have been applied in other studies (17). Patients were asked not to wash or use any emollient for 12 h immediately prior to each visit. They were treated within 14 days of the screening visit. The patients were photographed prior to treatment and fluorescence images were obtained before application of MAL, after incubation with MAL, after illumination and at follow-up visits.
Methyl-aminolevulinate cream
Each patient was treated with MAL cream on the right cheek, while the left cheek served as control, receiving red light only. The treatment area was defined by the area of a circular template (10 cm in diameter). The MAL cream (160 mg/g, Metvix®, PhotoCure ASA, Oslo, Norway) was applied evenly to the template placed on the right cheek. The cream was applied in a 1 mm thick layer and covered with an adhesive occlusive dressing (Tegaderm® and 3M Micropore; Beiersdorf A/S, Birkeroed, Denmark). After 3 h, the cream was wiped off gently.
Illumination
Illumination was performed using non-coherent red light from an Aktilite® CL 128 lamp (Photocure, Oslo, Norway) (average wavelength 635 nm, light dose 15 J/cm2 and a fluence rate of approximately 63 mW/cm2). The right and the left cheek were treated sequentially. The illuminated area was defined by covering the parts of the face not receiving illumination using double-folded green sheets.
Follow-up
Patients were followed up 1, 10 and 20 weeks after treatment. At each visit clinical acne scores and the patients’ own evaluations of treatment outcome were recorded. In addition, fluorescence imaging, P. acnes counting and sebum measurements were performed as described below. Furthermore, all adverse events were recorded. All but four patients attended the follow-up visits. The premature discontinuation was related to treatment failure in two patients, military service in the third and an injury that required treatment with antibiotics in the fourth. Thus 19 patients completed the study.
Assessment of acne score
Moderate inflammatory facial acne vulgaris was defined as at least 10 inflammatory lesions (papules and pustules) and more than 10 non-inflammatory lesions (open and closed comedones) counted within an area defined by a circular template. Severe acne was defined as at least 10 inflammatory lesions and presence of cystic lesions, or more than 15 inflammatory lesions. The number of acne lesions was counted manually by the investigator for both treatment site and control site. Counting was performed at baseline, i.e. before treatment, and at the follow-up visits. The number of inflammatory and non-inflammatory lesions was assessed by marking each counted lesion with a pen to ensure that each lesion was only registered once. The global severity of acne was assessed by the investigator using the 4-point Pillsbury rating scale (20) used in our clinic in previous acne studies.
Assessment of treatment outcome
The treatment outcome was assessed by recording the acne score, as described above. In addition to the investigator’s recording of acne score, the clinical success was also rated by the patients.
Fluorescence imaging
Fluorescence imaging was performed using a fluorescence imaging device (21), Photo Demarcation System 1, Prototype 5 (Medeikonos AB, Göteborg, Sweden). The equipment consists of Hg-lamps for fluorescence excitation, 365 ± 5 nm and 405 ± 5 nm, and a filtered CCD camera to record the porphyrin fluorescence in the range 610–700 nm. The size of the images was 512 × 512 pixels, corresponding to an area of 10 × 10 cm. The output images consist of grey level images with 12-bit resolution.
Propionibacterium acnes count
The quantity of P. acnes in the skin was determined using a method introduced by Mills & Kligman (22). This method has been described in detail in a previous study (18). The content of the sebaceous follicle is extracted by obtaining a skin surface biopsy using a quick setting cyano-acrylate polymer. The extract is thereafter transferred to a culture dish and the number of colony-forming units of P. acnes calculated.
Sebum measurement
The sebum measurement was performed by briefly pressing a plastic film from the sebumeter against the skin for 30 sec Samples were acquired from a site located 3 cm lateral to the alar rim on both cheeks. Care was taken to ensure that samples were obtained from the same location at each visit. A Sebumeter Combi SM810/CM825/PH900 (Courage Khazaka Electronic, Köln, Germany) was used for photometric analysis of the sebum content immediately after obtaining the sample. The sebum content is expressed in µg sebum/cm2.
Data analysis
The fluorescence images from the cheek treated with light only (control) were analysed with respect to the number of highly fluorescent pores before illumination, after illumination and at follow-up visits, using Matlab Image Processing Toolbox (Mathworks Inc., Natick, MA, USA). Images from the MAL area were assessed visually in order to investigate the selectivity of fluorescence to the acne lesions. The results of the analysis of the fluorescence images were compared with the clinical assessment.
Statistical analysis
It was calculated that more than 17 patients were required to detect an improvement in acne score with a power of 90% at a significance level of 5%. The differences between MAL-PDT area and control area concerning the change in lesion counts, acne score, quantity of P. acnes, and sebum content were analysed using Wilcoxon signed-rank test for continuous variables and Sign test for ordinal variables.
RESULTS
Clinical assessment
The patient and lesion characteristics at baseline are presented in Table I. As shown, the baseline counts of both inflammatory lesions, i.e. papules, pustules and cysts, and non-inflammatory lesions (comedones) were similar in both facial regions allocated to either MAL-PDT (right cheek) or light only control (left cheek). Based on the investigator’s global severity assessment, acne was graded as moderate in 8 patients and severe in 15 patients at baseline. Significant reductions in acne score (p < 0.01) were obtained at follow-up visits after 10 and 20 weeks for both MAL-PDT and control. No significant difference in acne score was observed between the groups. The distribution of recorded Pillsbury grade at baseline and follow-up (week 10 and 20) for the two different treatment locations is shown in Table II.
Table I. Patient and lesion characteristics at baseline, intent to treat population (n = 23)
| MAL-PDT (n = 23) | Control (n = 23) | |
| Global severity; n (%) | ||
| Moderate | 8 (35) | 8 (35) |
| Severe | 15 (65) | 15 (65) |
| Inflammatory lesion type; median (range) | ||
| Papules | 4 (1–7) | 3 (0–6) |
| Pustules | 7 (1–13) | 7 (1–15) |
| Nodulo-cystic lesions per patient; n (%) | ||
| 0 | 10 (44) | 13 (57) |
| 1 | 6 (26) | 6 (26) |
| 2 or more | 7 (30) | 4 (17) |
| Comedones per patient; n (%) | ||
| < 10 | 1 (4) | 1 (4) |
| > 10 | 22 (96) | 22 (96) |
MAL: Methyl-aminolevulinate; PDT: photodynamic therapy.
Table II. Frequency distribution of recorded Pillsbury grade at baseline and follow-up (week 10 and 20) for the 2 different treatment locations receiving either methyl-aminolevulinate-photodynamic therapy (MAL-PDT) or serving as control, i.e. treated with light only
| Pillsbury gradea | I | II | III | Total | ||||
| MAL-PDT | Control | MAL-PDT | Control | MAL-PDT | Control | MAL-PDT | Control | |
| Baseline | 0 | 0 | 8 | 9 | 15 | 14 | 23 | 23 |
| Week 10 | 7 | 7 | 10 | 12 | 5 | 3 | 22 | 22 |
| Week 20 | 7 | 8 | 9 | 8 | 3 | 3 | 19 | 19 |
aPillsbury grade; I: Acne with few or a lot of comedones with little or no inflammation; II: Acne with comedones, pustules and inflammatory lesions; III: Acne consisting of comedones, pustules and deeper inflammatory lesions.
Fig. 1 shows the average numbers of inflammatory acne lesions at baseline and at follow-up visits for both treatment locations, MAL-PDT and control. The numbers of papules and pustules were significantly reduced at the two follow-up visits at both the MAL-PDT and the control sites. The reduction in number of cysts observed at follow-up was only significant after 10 weeks. The number of patients with more than 10 non-inflammatory lesions (comedones) at baseline and at both follow-up visits is shown in Fig. 2. Also, the number of comedones was found to be significantly reduced at both treatment locations (MAL-PDT and control), equally at 10 and 20 weeks, as illustrated by Fig. 2. No significant differences were obtained by comparing the MAL-PDT and the control sites, for either the inflammatory lesions (Fig. 1) or the non-inflammatory lesions (Fig. 2). This result implies that the numbers of inflammatory and non-inflammatory acne lesions were reduced in both cheeks, although only the right cheek received MAL-PDT.
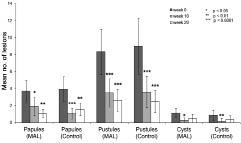
Fig. 1. Mean number of inflammatory lesions for the treatment site undergoing methyl-aminolevulinate-(MAL) photodynamic therapy and the control site (Control) at baseline, and at follow-up visits 10 and 20 weeks after treatment. Asterisks indicate significance level of difference compared with baseline.
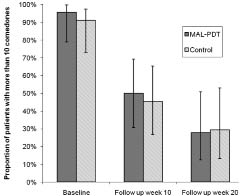
Fig. 2. Proportion of patients with more than 10 comedones at baseline, and at follow-up visits 10 and 20 weeks after treatment. MAL: methyl-aminolevulinate; PDT: photodynamic therapy.
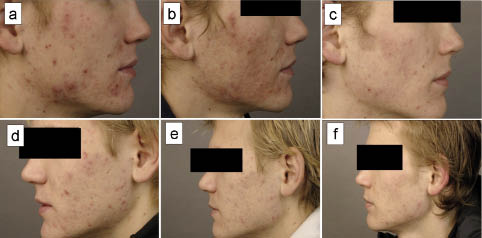
Clinical photographs from a typical patient before and after treatment are presented in Fig. 3. As shown, the acne has improved at the 20-week follow-up visit for both treatment locations, MAL-PDT and control. No new lesions were observed on either cheek. One week after treatment, erythema and hyperpigmentation were present on the MAL-treated site, and the acne had worsened.
Fig. 3. Clinical photographs of a patient with acne severity III according to Pillsbury, treated with methyl-aminolevulinate-photodynamic therapy (a–c): and control (d–f). (a) and (d) at baseline, (b) and (e) one week after treatment, and (c) and (f) at follow-up visit after 20 weeks.
Patients’ assessment
The assessment of treatment outcome made by the patients themselves at the follow-up visit 20 weeks after treatment is summarized in Fig. 4. A majority of the patients assessed that their acne had improved on both cheeks, i.e. MAL-PDT (15 patients) and control (14 patients). Seven patients experienced a “marked improvement” in their acne, and this number was the same for both MAL-PDT and control. No statistically significant difference between MAL-PDT and control was observed.
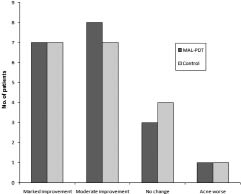
Fig. 4. Patients’ own assessments of improvement in acne at follow-up visit 20 weeks after treatment with methyl-aminolevulinate-photodynamic therapy (MAL-PDT) and control.
Evaluation of fluorescence images
Fluorescence images, obtained at baseline and before any treatment procedure, showed the presence of numerous small and highly fluorescent pores in 14 out of 18 patients. The high fluorescence of the pores is due to the presence of endogenous porphyrins produced by P. acnes. However, no significant correlations were found between the number of highly fluorescent pores and acne severity, the number of lesions or the quantity of P. acnes.
Fluorescence images, obtained after 3 h incubation with MAL cream, were compared with clinical photographs at baseline. In 6 of the18 fluorescence images, inflammatory lesions were observed as spots with enhanced porphyrin fluorescence after incubation of MAL. In these images, larger and more inflammatory lesions were observed to exhibit a higher fluorescence, as illustrated in Fig. 5. In the other 12 images, the patients exhibited homogeneously high porphyrin fluorescence in the MAL-treated area, and no lesions were visible (Fig. 6). Inflammatory lesions were indeed visible in the clinical photographs of these 12 patients, which implies a lack of selectivity for the MAL to acne lesions. Scars from old acne lesions with no inflammation did not show any accumulation of porphyrin in 4 patients.
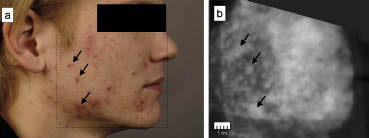
Fig. 5. Example of selective fluorescence after methyl-aminolevulinate treatment in a patient with inflammatory acne lesions. (a) Clinical photograph. (b) Fluorescence image. Arrows indicate location of inflammatory lesions.
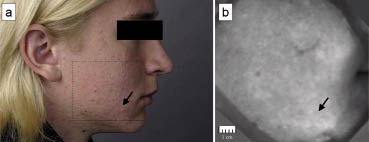
Fig. 6. Example of homogenous fluorescence after methyl-aminolevulinate treatment in a patient with acne. (a) Clinical photograph. (b) Fluorescence image. Arrows indicate location of inflammatory lesions.
The photobleaching of porphyrins of P. acnes was assessed by obtaining a fluorescence image immediately after irradiation of the light only (control site) treatment site. After the light only (control) treatment the number of highly fluorescent pores was assessed. Only 8 of the originally 14 images in which highly fluorescent pores were present showed a decreased number of fluorescent pores after treatment. In 6 patients, the fluorescence remained the same before and after illumination. Thus no correlation was found between the decreased number of highly fluorescent pores and treatment efficacy.
Also the photobleaching of the MAL-treated location was assessed by fluorescence imaging. Apparent photobleaching of MAL fluorescence after irradiation was present in 13 patients. No correlation between photobleaching and improvement in acne score was observed, but 4 of the patients with apparent photobleaching in the MAL-treated area also reported serious local adverse events (AEs) for the corresponding treatment location.
Assessment of sebum excretion rate and Propionibacterium acnes acnes
Neither the sebum excretion rate nor the quantity of P. acnes decreased significantly after treatment. The average sebum excretion rates (± standard deviation) at baseline were 68 ± 47 µg sebum/cm2 (MAL) and 72 ± 54 µg sebum/cm2 (control). No significant change in sebum secretion was noted at follow-up of both groups after 10 and 20 weeks. The average quantity of P. acnes at baseline was 4 × 105 ± 10 × 105 and 1 × 105 ± 2 × 105 for MAL and control, respectively. No significant change in the quantity of P. acnes was found in the MAL and control group at follow-up.
Adverse events
All patients reported local AEs at the one-week follow-up, all being related to the treatment site of MAL-PDT. No patient reported any AE for the control site treated with light only. The reported treatment-related local AEs were erythema, dryness, stinging, exfoliation and hyperpigmentation, graded as none, mild, moderate or serious. Erythema was observed in all patients except one. Four patients had more serious erythema and one had serious exfoliation. No correlation with AEs and skin type was seen.
Five patients experienced serious AEs. In four of these patients the fluorescence images revealed that apparent photobleaching took place during irradiation. The fluorescence images of the fifth patient were not analysed due to poor quality. All local AEs were resolved by the time of the follow-up at week 10, except for two patients with hyperpigmentation. One of those was resolved at the 20 weeks follow-up, but for the other patient hyperpigmentation remained for additional 12 weeks, i.e. in total 8 months after treatment. During illumination, patients experienced moderate to severe pain on the MAL-treated site and no pain at the control location. None of the included patients discontinued due to AEs.
DISCUSSION
The results of this controlled split-face study performing single treatment low light dose MAL-PDT with red light in patients with moderate to severe inflammatory facial acne show no advantage of the side treated with MAL-PDT compared with the control side treated with light only. Both treatment protocols, i.e. MAL-PDT and control, showed a moderate clinical improvement at follow-up. Also the patients themselves experienced a significant improvement in their acne on both cheeks; however, all patients reported AEs for the MAL-PDT treated location. The reason for choosing a split-face study design was to ensure that both sides, either treated with MAL-PDT or functioning as control, should be exposed to similar conditions, e.g. moisturizing creams and daylight. The study was designed to be unblinded because of our experience from earlier studies, in which it was easy to determine which was the MAL-treated side due to the presence of slight irritation after MAL application. Therefore a blinded study would have been misleading since true blindness is difficult to obtain.
The results of the present study differ somewhat from a former study by our group, in which a significantly greater reduction in the total number of inflammatory lesions was found with MAL-PDT compared with placebo PDT (19). In both studies we found a reduction in non-inflammatory lesions in both groups (MAL-PDT and placebo-PDT), but no statistically significant difference was observed between the groups (19). The major difference in the treatment protocol between the two studies is that the former study was based on two consecutive MAL-PDTs, performed 2 weeks apart, at a light dose of 37 J/cm2, corresponding to the normal dose in routine PDT of actinic keratosis and basal cell carcinomas at our clinic. In the present study, a light dose of 15 J/cm2 was applied. This lower dose is less than half the dose applied in the earlier study. The lower dose was chosen based on another dose-finding study investigating ALA-PDT for treatment of acne (18). In that study, a single treatment protocol was used and no difference in treatment effect was observed comparing high (50 J/cm2) and low (30 J/cm2) light dose using a broadband lamp; however, the side-effects and pain during treatment were more pronounced using the high light dose protocol.
Fluorescence imaging has been used previously for investigating the selectivity of PpIX formed after application of ALA or MAL in tumours (23) and acne (17). Other authors have showed a selective fluorescence in acne lesions after application of MAL (17); however, selectivity towards inflammatory acne lesions was only found in 6 out of the 18 images in our study. Instead a more homogeneous sensitization was observed in the majority of patients (12 out of 18). The homogenous sensitization suggests that a general superficial photoablation of the treated area takes place rather than a selective treatment of the sebaceous glands. This is further verified by the fact that the patients suffering from serious AEs also found to exhibit a high degree of photobleaching of the MAL-treated area after irradiation. This finding agrees well with the result from Wiegell et al. (24) showing an association between the amount of PpIX fluorescence before illumination and pain during PDT.
We could not find a correlation between the number of highly fluorescent pores, acne severity, the number of lesions and the quantity of P. acnes. This is confirmed by other studies showing that there is no correlation between severity of acne and the quantity of P. acnes (25). Instead it seems to be each patient’s immunological response to the bacteria that decides the severity of the acne (25).
The obtained treatment effect of the control side, treated with red light only and no applied sensitizer, is justified by other studies (9). The results of this study were, however, surprising since it is believed that photoactivation of the porphyrins of P. acnes is expected to contribute to the treatment, particularly if no external photosensitizer is used. Thus photobleaching was expected. A possible reason might be that the photoactivation of P. acnes is not the sole contributor to the treatment effect for red light only. Since P. acnes is an anaerobic bacterium, and oxygen is needed for the photodynamic process, it is likely that the anaerobic environment in the pores is lowering the efficiency of the photodynamic action. Seaton et al. (26), suggest that light treatment increases the production of transforming growth factor (TGF-β), which promotes resolution of inflammation. Thus the improvement on the cheek treated with light only could be explained by anti-inflammatory properties by influencing cytokine release from macrophages or other cells (27, 28). Another contributing factor could be a systemic immunological effect related to a reaction at the MAL-PDT side.
No significant change in either the quantity of bacteria extracted or the sebum excretion rate was found at any time on either treatment site. Also other previous reports have failed to show reduced quantity of P. acnes after PDT (15, 18) and treatment with visible light (29). Concerning sebum excretion the reports are more contradictory. For example, some authors show a significant decrease in sebum excretion after a single dose of PDT (12), while others verify our results that the sebum excretion is not affected (15). Our findings imply that MAL-PDT does not affect the bacterial flora of the skin in a clinically significant manner, and the destruction of P. acnes and sebaceous gland cannot be the sole mechanism of action for PDT in acne.
The findings of this study could be a step forward in determining the optimal parameters when performing topical PDT for treatment of acne vulgaris. It seems that when using single treatment and low light dose (15 J/cm2), MAL-PDT shows improvement in acne score, although the improvement is not significantly higher than the control treatment receiving light only. The improvement in acne persisted for 20 weeks for the comedones, papules and pustules, but not for the cysts. Earlier studies have shown that when two consecutive treatments are performed, at a higher light dose, i.e. 37 J/cm2, MAL-PDT is more effective than low light only. The findings from this study suggest that MAL-PDT for treatment of acne needs a higher dose than 15 J/cm2 and more than one treatment to be more effective than a single treatment of red light. Hence, there is a desire to optimize the treatment to obtain a long-lasting effect. Further studies investigating repeated light treatments or combinations with other topical treatments will help to clarify the best treatment protocol for acne.
ACKNOWLEDGEMENTS
Financial support for this study was obtained from the Sahlgrenska University Hospital. The authors thank biomedical technician Ellinor Mattson for valuable help with the culture of P. acnes, and Martin Gillsted for skilful help with photographs, statistics and technical details.
Conflicts of interest: Dr Wennberg has participated in clinical trials with Galderma International, Photocure, 3M and Fujisawa. She has previously received honoraria for lectures from Galderma International, PhotoCure, 3M and Fujisawa and Schering-Plough.
REFERENCES

