Josefin Lysell1, Desiree Wiegleb Edström1, Annika Linde2, Göran Carlsson3, Johan Malmros-Svennilson3, Anders Westermark4, Jan Andersson5 and Carl-Fredrik Wahlgren1
1Department of Dermatology, Karolinska University Hospital, Solna, Stockholm, 2The Swedish Institute for Infectious Disease Control (SMI), Solna, 3Childhood Cancer Unit, Astrid Lindgren Children’s Hospital, 4Department of Maxillofacial Surgery, and 5Division of Infectious Diseases, Department of Medicine, Karolinska University Hospital, Solna, Stockholm, Sweden
Hydroa vacciniforme is a rare, usually quite severe, photodermatosis. Association with Epstein-Barr virus infection and a possibly increased risk of lymphoproliferative malignancy have been demonstrated. We describe here four patients with Epstein-Barr virus-associated hydroa vacciniforme treated with acyclovir/valacyclovir therapy with a good clinical response. The children were reported to have less fatigue, fewer eruptions, less scarring, and increased ability to spend time outdoors without provoking new eruptions. This was also in agreement with clinical observations. However, one patient progressed into an anaplastic lymphoma kinase-1-negative anaplastic large-cell lymphoma in the upper jaw. This was preceded by an increase in EBV viral load. Acyclovir/valacyclovir therapy is a safe treatment. Further studies are required to confirm these results. Key words: acyclovir; valacyclovir; child; Epstein-Barr virus; lymphoma; oral ulcer; photosensitivity.
(Accepted February 9, 2009.)
Acta Derm Venereol 2009; 89: 393–397.
Josefin Lysell, Department of Dermatology, Karolinska University Hospital, Solna, SE-171 76 Stockholm, Sweden. E-mail: josefin.lysell@karolinska.se
Hydroa vacciniforme (HV) is a rare photosensitivity disorder affecting children. It is characterized by erythema, vesiculopapules, bullae, necrotic crusts and scarring on sun-exposed areas. The disease is usually sporadic and, in general, heals spontaneously by late adolescence (1, 2). Severe cases may have systemic manifestations, such as fever and malaise (3). Histologically, HV skin lesions demonstrate epidermal necrosis associated with dense lymphocytic infiltration in the dermis (1, 3). Although no causation has been identified, the association of Epstein-Barr virus (EBV) infection with HV has been demonstrated previously (e.g. 2, 4, 5). We describe here four patients with HV. Three of the four had documented elevated levels of EBV DNA copies in their peripheral blood and a considerable number of infiltrating cells with EBV-encoded small nuclear RNA (EBER) in cutaneous lesions. EBER is expressed only in full viral replication. As well as therapy including rigorous ultraviolet (UV) protection and topical glucocorticoids, all the patients received oral acyclovir with a positive clinical response. To our knowledge, the effect of acyclovir treatment in HV has not been reported previously.
One patient progressed into an anaplastic lymphoma kinase-1-negative anaplastic large-cell lymphoma in the right upper jaw. The risk of lymphoproliferative malignancy in children with HV and chronic EBV infection should be kept in mind, and we recommend internal investigation and close follow-up.
Case reportS
Case 1
A 6-year-old boy with a 12-month history of typical HV skin lesions, photosensitivity, fatigue and intermittent low-grade fever was admitted to our clinic. At onset of disease one year earlier he had also had ocular symptoms diagnosed as keratitis. He had a medical history of toddler’s diarrhoea, but was otherwise healthy. The parents recalled no infections preceding onset of the skin lesions.
The histological picture in skin biopsy was in accordance with HV. A photo-test showed normal minimal erythemal dose (MED) for UV-B radiation (UVB) (xenon arc lamp, XBO 150 Watt) 24 mJ/cm2 and normal MED for UV-A radiation (UVA) > 20 J/cm2 (UVA SUN 3000, Mutzhas Co, Munich, Germany). A provocation test with UVA 70 J/cm2 (UVA SUN 3000), showed slight pigmentation and UVB 3 MED (UV 208 Waldmann, Germany) with local erythema. The patient had skin-type IV according to Fitzpatrick. Routine blood chemistry was normal. ANA-, SSA-, SSB-antibody tests and porphyria investigation in urine/faeces/blood were negative. Quantitative polymerase chain reaction (PCR) assay for EBV DNA in serum (6) showed 7400 EBV genome/ml (Table I). Detection of EBV-infected cells in skin biopsy by in situ hybridization showed abundant EBER-positive cells. Serology for EBV showed EBV virus capsid antigen IgG > 1280, IgM < 40, EBV early antigen IgG 320D and EBV nucleus antigen A Ig 5, in accordance with a relatively recent EBV infection (7). Two years later, follow-up serology showed no significant change. Treatment was started with acyclovir twice daily at a total dose of 28 mg/kg/24 h. At the follow-up visits, the parents and the patient reported decreased photosensitivity. The patient could stay outdoors longer with fewer new eruptions, and these tended to be more superficial and seldom scarring. The parents reported that their son was more alert and had less need for sleep than before acyclovir treatment was initiated. Fever was now absent. This patient again had keratitis and, interestingly, this was treated successfully with topical acyclovir.
Table I. Epstein-Barr virus (EBV) viral load and serology in four cases of hydroa vacciniforme
| Case (year of birth) | Sample to laboratory (date) | Material | EBV PCR | EBV VCA | EBV EA D or R2 | EBNA | p107 = EBNA 1 |
| Genome/ml | IgG | IgM | IgG | Ig3 | IgG | IgM |
| Case 1 (1997) | 8.4.2005 | Serum | 7400 | ≥ 12801 | < 40 | 320 D2 | 5 | < 100 | < 100 |
| Acyclovir treatment initiated |
| | 21.9.2005 | Plasma | 480,000 | | | | | | |
| | 30.9.2005 | Plasma | < 10 | | | | | | |
| | 10.10.2005 | Plasma | 10–900 | | | | | | |
| | 3.11.2005 | Plasma | 2800 | | | | | | |
| | 12.5.2005 | Serum | 10–900 | | | | | | |
| | 1.3.2007 | Serum | 10–900 | | | | | | |
| | 17.4.2007 | Plasma | 10–900 | 640 | < 40 | 80 | ≤ 5 | < 100 | 330 |
| Case 2 (1994) | 25.4.2005 | Serum | < 200 | 1280 | < 20 | 80 | nd | > 1000 | < 100 |
| Case 3 (1999) | 23.11.2004 | Serum | 2800 | 2560 | < 40 | 320 | ≥ 204 | > 1000 | 280 |
| Acyclovir treatment initiated |
| | 6.10.2005 | Plasma | 1270 | | | | | | |
| | 13.8.2007 | Serum | 30,100 | | | | | | |
| | 20.8.2007 | Serum | 10,800 | | | | | | |
| | 16.11.2007 | Serum | 19,000 | | | | | | |
| Rituximab treatment initiated |
| | 5.12.2007 | Serum | 600 | | | | | | |
| | 18.12.2007 | Serum | 0 | | | | | | |
| | 21.12.2007 | Serum | 540 | | | | | | |
| Case 4 (2001) | 19.4.20065 | | | | | | | | |
| Acyclovir treatment initiated |
| | 31.5.2006 | Plasma | 7500 | | | | | | |
| | 20.6.2006 | Serum | nd | 5120 | < 40 | 1280 | 80 | > 1000 | 240 |
| | 20.6.2006 | Plasma | 4 500 | | | | | | |
| | 18.10.2006 | Serum | 50–500 | | | | | | |
| | 5.7.2007 | Serum | 8200 | | | | | | |
| | 26.2.2008 | Serum | 9100 | | | | | | |
1titration was ended at 1280.
2D=the diffuse component, antibodies often characteristics of recent infections. R= the restricted component, antibodies may remain for a long time after the primary infections.
3Anticomplement staining; does not separate antibody classes.
4end point titration is not always performed when EBNA antibodies are detected, has no informative value on single samples.
5Acyclovir treatment was initiated before EBV samples were taken on another indication when patient was admitted to inpatient ward.
PCR: polymerase chain reaction; VCA: virus capsid antigen; EA: early antigen; EBNA: EBV nuclear antigen; Ig: immunoglobulin; nd: not done.
To exclude progression into lymphoma the patient was referred to a paediatric oncologist in 2005. Investigation was negative with no signs of lymphoma. The large increase in EBV viral load (Table I) is thought to have been a laboratory error.
This patient has continued to have episodes with eruptions and fatigue. Acyclovir has been given in a total dose of 14–28 mg/kg/24 h, for shorter periods (one to several weeks), when symptoms have been present, with good response reported by patient and parents.
Case 2
A 9-year-old boy, born in Syria, was referred to us with a 4-year of history of vesiculopapules developing into necrotic crusts on sun-exposed skin areas. Earlier he had been diagnosed, both in Syria and the Netherlands, as having actinic prurigo. This boy also had had periods of ocular symptoms diagnosed as conjunctivitis since onset of disease. The clinical picture was typical of HV. Investigation at our clinic showed a histological picture in skin biopsy in accordance with HV. Routine blood chemistry showed no abnormalities. A photo-test showed normal MED for UVB 28 mJ/cm2 and normal MED for UVA > 20 J/cm2. Provocation tests with UVA 75 J/ cm2 and UVB 2 MED were negative. The patient had skin-type III according to Fitzpatrick. At the age of 11 years, 6 years after the onset of disease, blood samples were taken for detection of EBV, and skin biopsy for detection of EBER-positive lymphoid cells. A quantitative PCR assay for EBV DNA in serum showed < 200 EBV genome/ml (Table I). Serology for EBV was in accordance with a past EBV infection. Detection of EBV-infected cells in skin biopsy with in situ hybridization showed abundant EBER-positive cells. Treatment was started with acyclovir five times daily at a total dose of 27 mg/kg/24 h. Three weeks after initiation, acyclovir treatment was stopped. Already two days after starting this therapy, the patient had become irritable, hyperactive, restless, and more tired and sleepy. Such symptoms have been described when acyclovir is given in too high a dosage. These side-effects made the parents reluctant to accept further acyclovir treatment even at a lower dosage. Interestingly, after these 3 weeks of acyclovir therapy the patient’s HV had improved. He could stay outdoors for longer periods and more often without developing eruptions. Six months later, he could be discharged from our outpatient clinic, < 6.5 years after onset of the disease.
Case 3
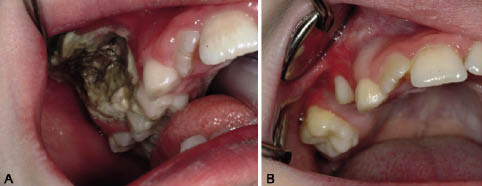
A 4-year-old girl was referred to our outpatient clinic for vesiculopapules on sun-exposed areas. The previous summer the parents had noticed a few transient vesicles. The following spring, during a ski trip, an acute eruption of abundant vesicles on sun-exposed areas occurred in the face. The parents also reported that their child had fatigue and increased need for sleep. No symptoms of infection preceding onset were reported. The clinical picture and skin biopsy were in accordance with HV. A photo-test showed a low MED for UVB with 4 mJ/cm2 threshold, whereas MED for UVA > 20 J/cm2 was normal. Provocation tests with UVA 50 J/cm2 and UVB 3 MED were negative. The patient had skin-type II according to Fitzpatrick. Routine blood chemistry showed no abnormalities. ANA-, SSA-, SSB-antibody tests were negative, as was a porphyria investigation in urine/faeces/blood. Quantitative PCR assay for EBV in serum showed 2800 EBV genome/ml (Table I). Serology for EBV was in accordance with past EBV infection. A skin biopsy with in situ hybridization showed EBER-positive cells. After investigation, acyclovir therapy was started twice daily at a total dose of 40 mg/kg/24 h. At the follow-up visit, the parents reported less photosensitivity and only a few new lesions, but without scarring. Their daughter was also more alert with less need to sleep. Unfortunately, this patient developed a malignant T-cell lymphoma in the right maxilla, diagnosed with a biopsy, at the age of 8 years. It started as an aphtous-like ulcer and progressed to a necrotic ulcer surrounding the primary molars (Fig. 1a). Primarily, fine-needle aspiration cytology, and a small biopsy only revealed unspecific mucositis. Only after resection of the whole necrotic area and two teeth was the diagnosis confirmed as an ALK-1-negative anaplastic large-cell lymphoma with EBV positivity and CD30 T cells proliferation. The lymphoma was treated with the collaborative European ALCL 99 protocol. Each course of chemotherapy, in total six, was started with rituximab (Mabthera®, 375 mg/m2 body surface area) to reduce EBV-containing CD20+ B lymphocytes.
Fig. 1. Case 3. (a) A necrotic ulcer in the gingival mucosa spread from the alveolar process into the buccal mucosa. It also traversed the alveolar crest into the palatal side. The primary molars were extracted and the necrotic area excised en bloc. Histological examination revealed an ALK-1-negative anaplastic large cell lymphoma with Epstein-Barr virus positivity and CD30 T-cells proliferation. (b) The same area 6 months later. The first premolar is erupting in the normal position. The reddish colour of the mucosa is often seen around an erupting tooth.
In November 2005 a large increase in EBV-load in the peripheral blood was seen (Table I). At that time the patient’s skin symptoms were under control, and no other symptoms of illness were reported. In August 2007, prior to development of lymphoma, EBV DNA was temporarily increased to 30,100 copies. At this time the acyclovir dosage was 32 mg/kg/24 h. Because the serum concentration of acyclovir was low, the treatment was changed to valacyclovir twice daily at a total dose of 60 mg/kg/24 h. The serum level of acyclovir then increased without an increase in the potential toxic metabolite CMMG (9-carboxymethoxymethylguanine).
Clinically, the patient is currently doing well with no signs of lymphoma at her last follow-up. Her ulceration has healed (Fig. 1b). She remains on valacyclovir 60 mg/kg/24 h. Quantitative EBV PCR is still positive at a low level.
Case 4
A 5-year-old girl was referred to our clinic for vesicles and papules turning into necrotic crusts in the face, on the ears and back of the hands. She had had low-grade fever since onset of skin lesions and an ulcer in the gum. The clinical picture and skin biopsy were in accordance with HV. Photo-testing showed normal MED for UVB 32 mJ/cm2 and normal MED for UVA > 20 J/cm2, provocation tests with UVA 50 J/cm2 and UVB 2 MED were negative. The patient had skin-type IV according to Fitzpatrick. Routine blood chemistry was negative, as were ANA-, SSA-, SSB- antibody tests and porphyria investigation in urine/faeces/blood. Quantitative PCR assay for EBV in plasma showed 7500 EBV genome/ml. Serology for EBV was in accordance with past infection. Skin biopsy showed abundant EBER-positive cells with in situ hybridization. Acyclovir therapy was initiated twice daily at a total dosage of 64 mg/kg/24 h. On follow-up visits, less photosensitivity, fewer skin lesions, less scarring, no further fever and less fatigue were reported. The acyclovir dosage was gradually increased because serum concentrations were low, present dosage being 72 mg/kg/24 h. Acyclovir treatment has been given continuously since onset of disease, initially in suspicion of herpes simplex virus, explaining why therapy was started before EBV results. This patient has had intermittent and transient problems with ulcers in the gum since onset of disease, diagnosed by an oral surgeon as gingivitis and aphtous ulcers. No biopsy has yet been performed from these ulcers. She is monitored by paediatric oncologists and dermatologists. No signs of lymphoma have been found.
Discussion
The association between HV or HV-like skin lesions and EBV infection has been demonstrated previously, although no clear aetiology has been established for HV. The question as to whether EBV infection may be associated with other photosensitivity disorders was addressed by Iwatsuki et al. (2), who determined the background levels of EBER-positive cells in other inflammatory skin disorders, including chronic photosensitivity dermatitis (5 cases), pityriasis lichenoides (5 cases), discoid lupus erythematosus (5 cases) and panniculitis (5 cases). They found no EBER-positive cells in these tissue sections. In the same paper, patients were divided into three different groups: probable, definite and severe HV; the severe group having a much higher risk of progression into malignancy. Of 11 patients with severe HV, 5 children progressed to overt EBV-associated malignant lymphoma with a natural killer (NK)/T-cell phenotype. The severe group was defined as patients with HV-like eruptions, facial swelling, indurated nodules on sun-protected as well as sun-exposed areas, high-grade fever and liver damage. The eruptions also tended to become more severe with age, unlike the typical course of HV. The histology of the severe type was similar to normal HV. Serology to EBV in the severe group tended to be abnormal, consistent with a chronic active EBV infection. These patients had higher levels of EBV-DNA in the peripheral blood associated with NK-cell lymphocytosis. Hypersensitivity to mosquito bites was also reported in the severe group. Patients with severe HV have been reported from Asia (8) and Latin America (9, 10).
We describe here four patients with clinically and histologically diagnosed HV with associated EBV infection. Skin biopsy from all four cases showed occurrence of EBER-positive cells by in situ hybridization. After EBV investigation, our patients were treated with oral acyclovir twice daily with a good response. The children were reported to have less fatigue, fewer eruptions, less scarring, and increased ability to stay outdoors without provoking new eruptions. This was also in line with clinical observations. The positive effect occurred within 2–4 weeks of therapy. The concentration of acyclovir and its toxic metabolite CMMG were monitored in the last two cases.
The effect of ganciclovir/acyclovir/valacyclovir on EBV replication/release has been questioned (11–13). Previous studies have not demonstrated any clinical effect on infectious mononucleosis. However, these studies revealed significant inhibition of EBV replication in oropharynx by acyclovir and inhibition of EBV release from irradiated B lymphoblastoid cell-lines by acyclovir and ganciclovir. Nevertheless, the clinical effect of acyclovir/valacyclovir treatment in our current patients can hardly be ignored, although it needs to be confirmed. Dosage and which type of antiviral drug to be used can be discussed.
Another approach is to reduce the number of EBV-infected cells, the vast majority of which are mature B lymphocytes expressing the surface antigen CD20. Thus rituximab (a monoclonal chimerical human/mouse anti-CD20-antibody) can be used for elimination of the pool of EBV-infected cells. Even though rituximab treatment is effective for chronic EBV infection/EBV-associated CD20+ lymphoma (14), we consider the treatment of a usually benign disease such as HV, with such a potent and new drug, to be ethically questionable.
Oral ulcers are not frequently reported in HV (15). However, polychromatic UVA has induced such lesions in a patient with HV (16), and EBV is associated with gingivitis and chronic periodontitis (17). In this case report, one patient had recurrent transient oral ulcers, which increased when the child was exposed to sun. Furthermore, one patient developed malignant lymphoma in the oral mucosa, which has not been reported previously in patients with HV. One could assume that our patients’ problems in the oral mucosa are probably associated with their HV and chronic EBV infections, and that this must be remembered in the follow-up of these patients.
Although most patients with typical HV have a good prognosis, the risk of progression to lymphoproliferative disorders must not be neglected. To establish risk factors for a more severe form of HV and to decide what variables to follow and whom to contact if progression is threatening is of great importance. The inability of the patient’s immune response to handle the EBV infection, resulting in an increasing load of EBV in peripheral blood, should lead to referral to a paediatric oncologist for internal investigation and follow-up. Children with EBV-associated HV should be monitored by dermatologists and paediatricians, working in close co-operation.
The authors declare no conflict of interest.
References