Ken Natsuga1, Daisuke Sawamura1, Maki Goto1, Erina Homma1, Yuka Goto-Ohguchi1, Satoru Aoyagi1, Masashi Akiyama1, Yoshimitsu Kuroyanagi2 and Hiroshi Shimizu1
1Department of Dermatology, Hokkaido University Graduate School of Medicine, Sapporo, Japan, and 2Regenerative Tissue Engineering, Graduate School of Medical Sciences, Kitasato University, Sagamihara, Japan
Recessive dystrophic epidermolysis bullosa (RDEB) is an inherited skin disorder caused by mutations in the COL7A1 gene, which encodes collagen VII (COL7). Skin ulcers in RDEB patients are sometimes slow to heal. We describe here the therapeutic response of intractable skin ulcers in two patients with generalized RDEB to treatment with an allogeneic cultured dermal substitute (CDS). Skin ulcers in both patients epithelialized by 3–4 weeks after this treatment. Immunohistochemical studies demonstrated that the COL7 expression level remained reduced with respect to the control skin and that it did not differ significantly between graft-treated and untreated areas. Electron microscopy showed aberrant anchoring fibrils beneath the lamina densa of both specimens. In conclusion, CDS is a promising modality for treatment of intractable skin ulcers in patients with RDEB, even though it does not appear to increase COL7 expression. Key words: epidermolysis bullosa; collagen VII; cultured dermal substitute; fibroblast; growth factor.
(Accepted October 6, 2009.)
Acta Derm Venereol 2010; 90: 165–169.
Ken Natsuga, Department of Dermatology, Hokkaido University Graduate School of Medicine, North 15, West 7, Sapporo 060-8638, Japan. E-mail: natsuga@med.hokudai.ac.jp
Epidermolysis bullosa (EB) comprises a group of inherited bullous disorders that can be divided into three main phenotypes – epidermolysis bullosa simplex (EBS), junctional epidermolysis bullosa (JEB), and dystrophic epidermolysis bullosa (DEB) – depending on the level of skin cleavage (1). DEB is caused by mutations in the collagen VII gene (COL7A1), which encodes the main protein that forms anchoring fibrils beneath the dermal-epidermal junction (DEJ) (2). DEB is inherited as either autosomal dominant (DDEB) or recessive (RDEB) disease, each form having a different clinical presentation (2). Severe generalized RDEB (RDEB-sev gen) is characterized by a complete absence of collagen VII protein (COL7) from the DEJ and a total loss of anchoring fibrils ultrastructurally. A milder form of RDEB, generalized other RDEB (RDEB-O), always shows detectable but decreased COL7 expression at the DEJ. Patients with RDEB easily develop skin erosions at sites of trauma. These usually resolve spontaneously within several weeks, but occasionally lead to more persistent skin lesions or intractable ulcers.
Allogeneic tissues have been used to develop several therapeutic approaches for skin ulcers. Apligraf® (Organogenesis, Canton, MA, USA) is an allogeneic cultured skin substitute that consists of keratinocytes and fibroblasts supported on a scaffold (3). It is indicated for the treatment of venous ulcers (4). The application of Apligraf® to EB skin ulcers has been reported in approximately 30 cases thus far, with favourable results (5–7).
In parallel, Kubo & Kuroyanagi (8–11) have developed an allogeneic cultured dermal substitute (CDS) comprising a two-layered spongy matrix of hyaluronic acid and atelo-collagen containing fibroblasts. The efficacy of this CDS has been shown in animal models and some clinical trials (11–16). Recently, three patients with RDEB-sev gen were reported to have been treated successfully with CDS, although details regarding COL7 expression were not mentioned (17). Here, we confirm the efficacy of this CDS in the treatment of intractable skin ulcers in two RDEB-O patients, and we conducted immunohistochemical and ultrastructural investigation into whether the expression of COL7 is altered after this CDS treatment.
METHODS
Patients
Two patients with RDEB-O whose diagnosis was made by COL7A1 mutation analysis and electron microscopy had persistent skin ulcers on their feet that failed to respond to supportive care for more than 6 months.
Preparation of allogeneic CDS
The CDS was prepared as described previously (9, 11). Briefly, an aqueous solution of hyaluronic acid (HA) with a cross-linking agent was frozen to –85°C in a dish and then lyophilized to obtain an HA sponge. The sponge was thoroughly rinsed with distilled water to remove free cross-linking agent, then the hydrated HA sponge was frozen and lyophilized to obtain a purified HA sponge, which was immersed in a dish of atelo-collagen (AC) solution. Medical-grade AC was prepared by enzymatic cleavage of telopeptides on both ends of type I collagen molecules derived from porcine dermis. The hydrated HA sponge with AC was frozen and lyophilized to obtain a two-layered sponge of HA and AC. Both surfaces of the two-layered sponge were irradiated with an ultraviolet lamp to induce intermolecular cross-linking between AC molecules.
Cell banking was established as described previously (9, 11). The piece of skin used in this study was derived from a young donor who was free from infectious viruses such as hepatitis B and C (HBV and HCV), human immunodeficiency virus (HIV) and human T-lymphotropic virus (HTLV), and who tested negative in the treponema pallidum hemagglutination test (TPHA), in compliance with the ethical guidelines of St. Marianna University Graduate School of Medicine (Kanagawa, japan). Fibroblasts were isolated by enzymatic treatment. Cultivation of fibroblasts was initiated in culture medium to establish cell banking, as described (18). Viral infection of the cells, including HBV, HCV, HIV, HTLV and parvovirus, was excluded.
The fibroblasts cryopreserved in cell banking were thawed and cultured to obtain an adequate number of cells. These fibroblasts were seeded on a two-layered spongy matrix and cultured for one week. The number of fibroblasts seeded on the two-layered sponge was adjusted to 1.0 × 105 cells/cm2. The resulting CDS was cryopreserved according to a previously described method (8, 19). Prior to clinical application, a polystyrene dish containing the CDS was placed in a foam polystyrene box at room temperature for 30 min and then floated in a water bath at 37°C.
Treatment regimens
After giving their informed consent, the patients received this CDS therapy. The surface of the designated skin ulcer was rinsed with saline solution. After thawing, then rinsing in lactated Ringer’s solution, the CDS was applied to the wound surface, together with a gauze dressing to protect the CDS. The CDS was fixed with the bandage, and there were no restrictions on patient activity at any time after the CDS was in place. A new CDS was applied twice a week for the first 2 weeks and then once a week afterwards.
Immunofluorescence
Skin biopsies were taken from both patients under local anaesthesia from non-blistered and grafted skin areas after re-epithelialization. Follow-up biopsies were at 4 weeks (Patient 1) and 3 weeks (Patient 2) after the first CDS treatment, respectively, and one week after the last CDS application. The specimens were embedded in optimum cutting temperature (OCT) compound (Miles Scientific, Naperville, IL, USA). Immunofluorescence staining was performed on 5-micron cryosections of skin with the monoclonal antibody LH7:2 (recognizing the NC-1 domain of COL7) (20). To estimate the amount of COL7, serial dilution of LH7:2 was performed to 1:10, 1:20, 1:40, 1:80, 1:160, 1:320, 1:640 and 1:1280. Labelling was visualized using fluorescein isothiocyanate (FITC)-conjugated goat anti-mouse immunoglobulin (Ig)G.
Electron microscopy
Skin biopsies were taken from Patient 2 under local anaesthesia from the intact and grafted skin areas after complete epithelialization. Skin biopsy samples were fixed in 2% glutaraldehyde solution, post-fixed in 1% OsO4, dehydrated, and embedded in Epon 812 (TAAB Laboratories Ltd, Aldermaston, Berkshire, UK). The samples were sectioned at 1 µm thickness for light microscopy and ultrathin sectioned for electron microscopy (at 70 nm thickness). The thin sections were stained with uranyl acetate and lead citrate and examined by transmission electron microscopy (Hitachi H7100, Hitachi, Tokyo, Japan).
CASE REPORTS
Patient 1
A 51-year-old female with RDEB-O had a history of three cutaneous squamous cell carcinomas (SCC), the details of which have been described elsewhere (21). COL7A1 gene mutation analysis revealed that the patient was a compound heterozygote for c.5443G >A (p.G1815R) and c.5818delC (22, 23). She presented with an intractable ulcer, measuring 30 × 11 mm, on the back of her right foot, which had failed to respond to conservative, supportive therapy for 10 months (Fig. 1A). A skin biopsy specimen from the ulcer showed no findings suggestive of SCC. The CDS treatment was performed at site of the ulcer, and epithelialization of the lesion was observed within 4 weeks after the onset of treatment (Fig. 1B). Labelling of the DEJ in the patient’s non-grafted and grafted skin samples with anti-COL7 antibody LH7:2 revealed no significant difference in the intensity of COL7 staining (Figs 2A, B). Both samples showed positive up to 1:160 dilution of the antibody as compared to 1:640 in normal skin (data not shown).
Fig. 1. Clinical response to allogeneic cultured dermal substitute (CDS) treatment (A). A skin ulcer measuring 30 × 11 mm on the back of the right foot in Patient 1. The ulcer had not healed for 10 months. (B) Re-epithelialization at 4 weeks after CDS treatment, although small erosions persist. (C) A skin ulcer measuring 21 × 20 mm on the right heel of Patient 2. The ulcer had persisted despite conservative treatment for 6 months. (D) Complete re-epithelialization 3 weeks after CDS treatment. The biopsy sites are indicated by arrows.
Fig. 2. Collagen VII (COL7) immunofluorescence study using LH 7:2 antibody (1:80 dilution). COL7 labelling in grafted skin samples (Patient 1; A, Patient 2; C) and non-blistered skin sample (Patient 1; B, Patient 2; D) shows the same intensity of staining at the dermal-epidermal junction (DEJ). Normal human skin (E) shows more intense staining at the DEJ than do patients’ skin samples (original magnification × 100). Arrows indicate DEJ.
Patient 2
A 38-year-old female had been diagnosed with RDEB-O. She also had IgA nephropathy and was being treated with corticosteroids. DNA analysis revealed a recurrent COL7A1 mutation c.5932C>T (p.R1978X) (23) and a novel mutation c.8029G>A (p.G2677S). She presented with a recalcitrant ulcer, measuring 21 × 20 mm, on her right heel, which had failed to respond to conservative therapy for the previous 6 months (Fig. 1C). Complete epithelialization of the lesion was observed 3 weeks after the beginning of CDS treatment (Fig. 1D). Labelling of the DEJ in the patient's non-blistered and grafted skin with LH7:2 revealed the same intensity of COL7 staining (Figs 2C, D). Both of the samples showed positive at the DEJ up to 1:320 dilution of the antibody (data not shown). Ultrastructurally, the anchoring fibrils from the patient's grafted skin samples were short, thin sub-lamina-densa structures (Fig. 3A) with the same features as those observed in the non-grafted skin samples (Fig. 3B).
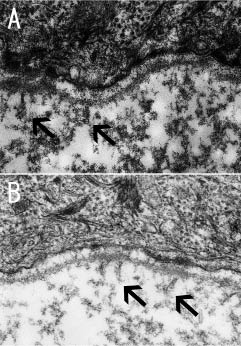
Fig. 3. Ultrastructural features of the sub-lamina densa region and basement membrane zone in the grafted and non-grafted skin of Patient 2. Discernible anchoring fibril-like structures (arrows) are observed beneath the lamina densa at the grafted skin site (A), as well as at the non-grafted skin site (B) (original magnification × 30,000).
DISCUSSION
Patients with EB have severe skin fragility and chronic wounding, which affect them physically and emotionally. Various controlled trials have been attempted with EB patients, including administration of phenytoin, topical bufexamac, aluminium chloride hexahydrate and oxytetracycline, although none of these has been uneqivocally successful (24). Experimental models of EB treatment have shown some promising results, but there are tremendous difficulties in translating such therapies into practical treatments for human patients (25). Ex vivo gene therapy for one patient with JEB (26) and allogeneic cell therapy for patients with RDEB (27) have been described in the literature. Allogeneic tissue-engineered skin grafts have also been used for patients with RDEB. McGrath et al. (28) reported that cultured keratinocyte allografts did not significantly improve wound healing in 10 patients with RDEB. Apligraf®, a composite of cultured fibroblasts and keratinocytes, showed favourable results in 12 patients with RDEB (5, 6).
The main role of anchoring fibrils, of which COL7 is the main component, is in maintaining normal epidermal-dermal adherence between the basal lamina and the underlying superficial dermis. Besides this adhesive role, COL7 also aids and facilitates in the attachment and migration of keratinocytes and fibroblasts (29), and COL7 dysfunction can result in delayed wound healing (30). Indeed, COL7 staining is observed in the wound bed and neodermis in acute wound healing (31). This is the first study to assess COL7 expression of patients with RDEB after CDS treatment by immunofluorescence and electron-microscopy. In both of our cases, increased expression of COL7 after this CDS treatment could not be confirmed. Some technical difficulties in detecting a small increase in the protein could explain this result, because patients with RDEB-O who participated in this study expressed reduced but detectable amounts of COL7 in the baseline. It is also possible COL7 released from allogeneic fibroblasts could have been degraded in the wound bed instead of depositing at the DEJ.
The fibroblasts contained in the CDS release various cytokines and growth factors that play major roles in modulating wound healing. These cytokines and growth factors include vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF), hepatocyte growth factor (HGF), keratinocyte growth factor (KGF), platelet-derived growth factor (PDGF), transforming growth factor (TGF)-beta1, and interleukins (IL)-6 and IL-8 (32, 33). These cytokines and growth factors may have contributed to accelerated wound healing in our patients, although the cytokine levels in the skin samples were not assessed.
This study demonstrated that CDS treatment potentially benefits patients with RDEB-O. Former studies also demonstrated that intractable ulcers of patients with RDEB-sev gen improved after CDS treatment (17). An application of CDS without fibroblasts could be used as a negative control and would have improved our study. We have reported previously a comparative study of CDS with and without cultured fibroblasts on animal models (34). However, it is not always ethically easy to design a control study in human clinical trials. Furthermore, in our study, we selected two RDEB patients whose persistent foot ulcers failed to respond to supportive care for more than 6 months and there were no other similar foot ulcer for a comparative study.
The clinical improvement observed after CDS treatment is promising, and no restrictions on patient activity are needed. However, it is not practical to apply CDS to all ulcers of RDEB patients, because multiple ulcers are typically found on the whole body of RDEB. Intractable ulcers in RDEB patients, which do not respond to supportive care for several weeks, should be the main target of CDS treatment.
In conclusion, our study clearly demonstrates the efficacy of this CDS in the treatment of intractable skin ulcers in RDEB patients. Further examination to elucidate the mechanism of this treatment is required.
REFERENCES