Edoardo Zattra1, Renato Zambello2, Filippo Marino3, Matteo Bordignon3 and Mauro Alaibac1*
1Dermatology Unit, 2Hematology Unit and 3Pathology Unit, University of Padua, Via C. Battisti 206, IT-35128 Padova, Italy. *E-mail: mauro.alaibac@unipd.it
Accepted November 25, 2010.
Mantle cell lymphoma (MCL) is a clinical entity characterized by the proliferation of CD5-positive antigen-naive pregerminal centre B cells within the mantle zone that surrounds normal germinal centre follicles (1). This lymphoma is associated with the chromosomal translocation t(11,14)(q13;q32), which is in turn responsible for cyclin D1 over-expression (2–4). The prognosis of MCL is usually poor, with a median survival time of 3–5 years (5). Skin involvement is rare in MCL, although in some cases cutaneous manifestations are the first symptom (6). Skin involvement suggests a disseminated disease and is often associated with blastoid cytological features (7). The existence of primary cutaneous MCL is controversial. Primary MCL is not included in the World Health Organization–European Organisation for Research and Treatment of Cancer (WHO–EORTC) classification for cutaneous lymphomas (8). We describe here the clinical, histopathological, immunohistochemical and molecular findings of a case of primary cutaneous MCL.
CASE REPORT
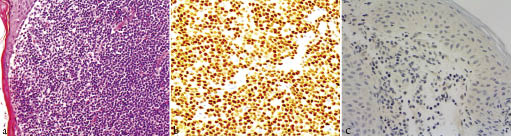
In October 2007, a 77-year-old man presented with several diffuse cutaneous erythematous nodules and plaques involving all body areas (Fig. 1). The first papular lesions appeared in 2005 and extended progressively in size and number. The first biopsy, performed in February 2006 in another unit, was consistent with the diagnosis of insect bite reaction. A second biopsy was therefore performed, which revealed the presence of atypical cells with a centrocytoid appearance (Fig. 2a). Immunohistochemistry showed the following phenotypical characteristics: cyclin D1+ (Fig. 2b), BCL2+, CD20+, CD22+, CD79a+, CD2–, CD3– (Fig. 2c), CD4–, CD5+, CD7–, CD8–, CD10–, CD23–, TiA1–. Molecular investigations for immunoglobulin heavy chain (IgH) gene rearrangement revealed the presence of a clonal population of B cells. On the basis of the histological, immunohistochemical and genotypical data, a diagnosis of cutaneous localization of MCL was made. White cell differential count and lymphocyte subpopulations were within normal ranges. Computed tomography scans of the head and neck, thorax, abdomen and pelvis showed no pathological findings. Total body positron emission tomography did not reveal any systemic involvement. A bone marrow biopsy was negative. A diagnosis of primary cutaneous MCL was therefore made. The patient was referred to the Haematology Unit, where a regimen of orally administered etoposide (100 mg/day on 5 consecutive days a month, for 11 months) and corticosteroids (prednisone 25 mg/day on 5 consecutive days a month, for 11 months) was utilized. The patient was then maintained on low-dose steroid (prednisone 5mg/day). After 28 months of regular follow-up, the patient has almost complete remission of the cutaneous manifestations.

Fig. 1. (a) Diffuse erythematous nodules and plaques involving the back. (b) Large erythematous plaque with erosions and crusts on the gluteal area.
Fig. 2. (a) Histology of a skin biopsy, showing the massive neoplastic infiltrate consisting of atypical cells with a centrocytoid appearance (haematoxylin and eosin (H&E) stain, ×40). (b) Neoplastic lymphocytes exhibiting strong immunohistochemical staining for cyclin D1. (c) Negative staining of skin-infiltrating cells for the pan-T-cell marker CD3 (immunoperoxidase stain, ×40).
DISCUSSION
Secondary involvement of the skin in MCL has been described in several cases (7, 9–13), whereas primary cutaneous MCLs have only exceptionally been reported (14, 15). The present case was characterized clinically by an aggressive clinical course with multiple plaques and nodules involving the trunk and extremities. Immunohistochemically, cyclin D1 was strongly expressed. Since expression of cyclin D1 in normal lymphoid cells is very low to undetectable, and only hairy-cell leukaemia shows moderate expression, positive immunohistochemistry for cyclin D1 is pathognomonic for MCL. Expression of cyclin D1 is indirect evidence of the t(11;14), which, depending on the methods used (e.g. PCR, Southern blot analysis, and cytogenetics), can be detected in approximately 35–66% of cases of MCLs.
A primary cutaneous lymphoma, according to the WHO–EORTC definition (8), is a lymphoma that presents in the skin with no evidence of extracutaneous disease at the time of presentation. Our patient showed no signs of extracutaneous involvement at presentation or at 28 months after diagnosis. We thus consider this case a primary cutaneous MCL. Primary cutaneous MCL is not included in the WHO-EORTC classification for cutaneous lymphomas. At present, in this classification, cutaneous B-cell lymphomas (CBCLs) are divided into indolent and intermediate subtypes. Indolent CBCLs include marginal zone B-cell lymphoma (incorporating the previous entities immunocytoma and plasmacytoma) and primary cutaneous follicular centre lymphoma, while intermediate CBCL include the primary cutaneous diffuse large B-cell lymphoma, leg type. In our patient, the cutaneous manifestations were disseminated and showed a tendency to progressive cutaneous dissemination. For this reason, the patient was treated with chemotherapy, which usually is not utilized for the indolent forms of CBCL. The cutaneous biological behaviour of the present case of primary cutaneous MCL was more similar to the leg-like subset of CBCL. The lesions in our patient were disseminated, large, and had a tendency to ulcerate. This behaviour is not generally observed in the indolent forms of CBCL, in which cutaneous lesions are often localized, less numerous, have a slow progression, and do not show a tendency to ulcerate.
In conclusion, we confirm that MCL can be observed primarily in the skin without systemic involvement. The clinical behaviour of primary cutaneous MCL is probably less aggressive than the systemic counterpart, and this is consistent with the view that the skin microenvironment favourably modulates the aggressiveness of lymphoproliferative disorders.
REFERENCES