Kathrin A. Giehl1, Matthias Schmuth2, Antonella Tosti3, David A. De Berker4, Alexander Crispin5, Hans Wolff1 and Jorge Frank6,7
Department of Dermatology, 1Ludwig-Maximilian University, Munich, Germany, 2Medical University Innsbruck, Austria, 3University of Bologna, Italy, 4University of Bristol, UK, 5Department of Medical Informatics, Biometry and Epidemiology, Ludwig-Maximilian University, Munich, Germany, 6Department of Dermatology, and 7GROW – School for Oncology and Developmental Biology, Maastricht University Medical Center (MUMC), The Netherlands
The autosomal dominantly inherited hair disorder pili annulati is characterized by alternating light and dark bands of the hair shaft. Concomitant manifestation of pili annulati with alopecia areata has been reported previously on several occasions. However, no systematic evaluation of patients manifesting both diseases has been performed. We studied the simultaneous or sequential occurrence of pili annulati and alopecia areata in individuals diagnosed in different European academic dermatology units. We included 162 Caucasian individuals from 14 extended families, comprising 76 affected and 86 unaffected family members. Statistical analysis showed that the frequency of alopecia areata among patients with pili annulati was higher than within the general population. Five of our patients with pili annulati have gone through severe episodes of alopecia areata. We cannot rule out that the currently unknown genetic defect underlying pili annulati might also confer an increased risk for the development of a more pronounced manifestation of alopecia areata. Based on the current data, and considering the low number within individual families of patients affected by both diseases, however, a direct association between pili annulati and alopecia areata seems unlikely. Key words: pili annulati; hair shaft abnormality; alopecia areata; hair loss.
(Accepted December 7, 2010.)
Acta Derm Venereol 2011; 91: XX–XX.
Kathrin Giehl, Department of Dermatology, Ludwig- Maximilian University, DE-80337 Munich, Germany. E-mail: Kathrin.Giehl@med.uni-muenchen.de
Pili annulati (PA) (OMIM 180600) is a rare autosomal dominantly inherited hair shaft abnormality, first noted by Landois in 1866 (1). Since 1950 only approximately 30 cases have been reported (2).
Clinically, the scalp hair of patients with PA has a shiny appearance due to alternating light and dark bands of the hair shaft (2). Scanning and transmission electron microscopy revealed that these bands reflect air-filled cavities within the hair shaft cortex (3, 4). Although intermittent breaks in the hair shafts are associated with these cavities, most patients with PA do not report increased hair fragility (5, 6).
A locus for PA has been shown on chromosome 12p24.32–24.33 (7, 8). A previous study of hair follicle morphology indicates that the disease may arise from a defect that putatively affects a regulatory element involved in the assembly of structural proteins within the extracellular matrix (9).
In contrast to PA, alopecia areata (AA) is a polygenetic, immune-mediated disorder of the hair follicle that has an unpredictable, and sometimes self-limiting, clinical course and affects approximately 1–2% of the general population (10).
The concomitant manifestation of PA and AA is well documented (11–18). However, these were mostly single case reports and there are no studies in which extended families with PA have been analysed for the occurrence of AA. We therefore sought to elucidate in a cohort of PA patients and families whether there is an association with AA.
MATERIALS and methods
Patients and families
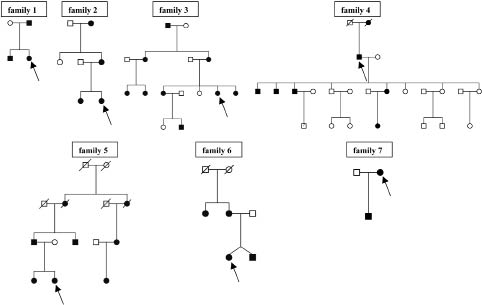
We analysed 162 Caucasian individuals from 14 Italian, German, Austrian, English and American PA families between January 2001 and October 2007 (Fig. 1). All subjects provided informed consent for inclusion in the study and completed a clinical questionnaire. Institutional review board approval for this study was waived. Patients revealing PA and AA were further characterized in-depth (Fig. 2a and Table I).
Fig. 1. Pedigrees of the seven families studied. Individuals with both pili annulati (PA) and alopecia areata (AA) are indicated by an arrow. Due to the high number of family members, only the most relevant individuals from family 4 are depicted here. The black symbols show affected individuals, the white unaffected individuals.
Fig. 2. Simultaneous manifestation of pili annulati (PA) and alopecia areata (AA) in a 38-year-old Caucasian female of Italian origin. (a) Patchy hair loss indicative of AA. (b) Dermoscopy at 20× magnification depicting PA (black arrows) as well as yellow dots and dystrophic hair (pink arrows) characteristic for AA. (c) PA at higher magnification (70×).
Table I. Clinical characteristics of the seven patients with strong pili annulati phenotype as well as alopecia areata (AA) in this study. There was no resolution of PA after the AA episodes.
|
Family
|
Sex
|
Country
|
Onset of AA (years)
|
Episodes of AA
|
Body site affected with AA
|
|
1
|
F
|
Italy
|
12
|
2×; duration 1 year
|
Whole body
|
|
2
|
F
|
UK
|
12
|
1×; duration 1 year
|
Whole body
|
|
3
|
F
|
Italy
|
38
|
2×; duration 8 years
|
Scalp (20%)
|
|
4
|
M
|
Austria
|
27
|
1×; duration unknown
|
Scalp (10%)
|
|
5
|
F
|
UK
|
13
|
2×; still ongoing
|
Scalp (80–100%)
|
|
6
|
F
|
Italy
|
9
|
5×; varying duration
|
Scalp (20%)
|
|
7
|
F
|
Italy
|
51
|
1×; duration unknown
|
Scalp (30%)
|
Statistics
Statistical analysis comparing the prevalence of AA in PA patients and unaffected family members was carried out by means of Fisher’s exact test. A two-sided p-value of < 0.05 was regarded as significant. The test was performed using SAS version 9.2 for Windows (SAS Institute, Cary, NC, USA).
Diagnosis and follow-up
After clinical assessment, samples were obtained by cutting 50 or more hairs at the scalp surface. Prior to examination, approximately 20 hairs were mounted in air and afterwards in water. Subsequently, hair shafts were examined by trans-illuminated light microscopy using a FotoFinder dermoscope microscope (Teachscreen Software, Bad Birnbach, Germany). Scalp dermoscopy was performed in two patients (Fig. 2b). In 6 of the 7 index patients (of families 1–3 and families 5–7) the diagnosis of PA was made after they had initially contacted a dermatologist for AA. While the initial diagnosis was usually made in different participating centres, a single dermatologist (KG) confirmed these diagnoses and performed a clinical examination and questionnaire of patients and families prior to inclusion.
Whenever possible, additional follow-up information from all patients with both PA and AA was gathered by telephone consultation 1–6 years after the diagnosis had been made (Table I).
Results
Families, pedigrees, and mode of inheritance
Of the 162 individuals from 14 families studied 76 (47%) had PA, whereas the other 86 (53%) were unaffected. In 7 of the 14 PA families (50%) an individual with concomitant AA could be detected (Table I and Fig. 1). In none of the families studied did more than one patient have an episode of AA.
Patients with both pili annulati and alopecia areata
Among the 7 patients with PA and concomitant AA (6 females, 1 male) the mean age of onset of AA was 23 years. They were not related to each other and resided in Italy (families 1, 3, 6, 7), England (families 2 and 5), and Austria (family 4).
In all 7 patients, PA was exclusively restricted to the scalp. Five of these individuals had had more severe episodes of AA (alopecia totalis or universalis). The prevalence of AA was higher in patients with PA than in unaffected family members. Seven out of 76 individuals affected by PA also had AA, whereas none of the 86 unaffected family members showed PA (p = 0.043).
In the patients with PA, episodes of AA lasted between a few months and 8 years, with four individuals reporting on more than one episode. During the follow-up telephone consultations all additional episodes of AA were documented (Table I). In three patients, loss of more than 80% of the entire body hair was observed (patients 1, 2 and 5). Whereas AA showed intervals of partial to complete remission in all affected patients, PA always persisted.
Discussion
In different, mainly anecdotal, case reports, a putative aetiopathological association between these disorders has been discussed (13–18). We provide here a systematic study on the concomitant manifestation of PA and AA.
Within members of the same PA family we observed intra- and inter-individual phenotypic differences in disease severity. The clinical symptoms are mostly subtle and the disorder is easily overlooked (2, 18). In line with this notion, 6 of the 7 patients who manifested both diseases were diagnosed with PA only after an episode of AA led to consultation with a dermatologist. In contrast to PA, AA cannot be missed easily (19).
Even though patients with PA often report that nobody else in their family is affected, relatives may be affected less severely and be unaware of the disease. Indeed, apart from the index patients, we identified several additional family members who were affected by PA (Fig. 1). An additional difficulty in making the diagnosis of PA is that there are few if any complications (2, 5). PA has to be differentiated from monilethrix (20, 21) and pseudopili annulati. The latter shows similar banding of the hair shaft due to periodic twisting and an elliptic shape in cross-section of the hair shaft, but can be excluded by light microscopy (22).
Based on approximately 30 reports on PA since 1950 and 20 single case reports published prior to 1921, the simultaneous occurrence with AA has been described in only nine cases (6, 11–18). In three of these previous reports an amelioration or disappearance of the PA phenotype was observed when AA became manifest and hair re-grew later on (15, 18, 23). In our cohort, however, we did not observe any amelioration or resolution of PA after the onset of AA. In line with this observation, five of the other patients previously reported elsewhere also did not experience any improvement in, or disappearance of, PA after the initial episode of AA. However, in all these cases follow-up data were not available and, thus, the course of the disease is not clear (11, 12, 14, 16, 17).
To date, the specific genetic defect causing PA has not yet been identified (24). Therefore, it is difficult to predict whether the unknown gene involved in the pathogenesis of PA could also contribute to the development of AA.
Interestingly, we found within our PA families a significantly higher prevalence of 9% for concomitant AA (95% confidence interval (CI): 4–18%) when comparing individuals affected by PA with unaffected individuals (0%; 95% CI: 0–4%). Although this percentage is higher than the currently reported AA frequency rate of 1–2% within the general population (10) we do not have hard evidence for a link between these disorders. Therefore, we consider it rather unlikely that there is a direct association between PA and AA, mainly for two reasons. First, in none of the PA families studied here, or in the patients reported elsewhere, could two or more individuals affected by both hair disorders be detected (11–18). Secondly, none of the previously published susceptibility loci for AA (25) coincide with the candidate region for PA (8, 9). Thus, if at all, such an association would probably be rather weak and not as strong as that of, for example AA and Down’s syndrome or autoimmune polyglandular syndrome (26). Furthermore, it should be considered that the previous reports suggesting a putative association between PA and AA (13–18) harbour the risk of selection bias, where a wrong assumption developed through the way the data were collected and selected, in particular when dealing with small samples (27).
The clinical co-manifestation of a rare disorder such as PA and a quite common condition such as AA should be evaluated critically, even though it is tempting to speculate that a hitherto unknown genetic defect giving rise to PA might also predispose for AA. Considering the latter, it may well be that mutations in this unknown gene also confer a structural or immunological weakness of the hair shaft that makes patients with PA more susceptible to the development of AA. Still, we would then have expected to find more individuals with both clinically overt PA and AA within our PA cohort.
Although apparently rare, the simultaneous occurrence of AA in patients with PA could be confirmed in our PA cohort. However, the total number of patients with both conditions identified to date seems too low to draw far-reaching conclusions. This may, in part, be due to the fact that the diagnosis of PA is easily overlooked. Considering the current data, a direct association between these two disorders seems rather unlikely.
ACKNOWLEDGEMENTS
The authors are grateful to the patients and their families for their interest and participation in this study. This work was supported by grants from the programme for “Förderung für Forschung und Lehre” (FöFoLe) of the Ludwig-Maximilians University of Munich.
References