The aim of this retrospective study was to assess the efficacy and tolerance of intravenous rituximab in multifocal primary cutaneous follicle centre lymphomas (PCFCL). Eleven patients with a multifocal PCFCL were treated with rituximab (MabThera®) administrated intravenously. After four infusions, an objective response was observed in 90% of patients, and one month after all the infusions (median of 6 infusions) all the patients had an objective response and complete remission was obtained in 7 of 11 patients (64%). Follow-up ranged from 9 to 65 months (median: 30 months). Local disease recurrence was observed in five patients. The median progression-free survival time after the end of treatment was 23.6 months. This study is the largest series of patients with multifocal primary PCFCL treated with intravenous rituximab. This therapy is a safe and effective treatment and could represent an excellent alternative treatment to radiotherapy. Key words: cutaneous lymphoma; rituximab; follicle centre lymphoma.
(Accepted January 12, 2011.)
Acta Derm Venereol 2011; 91: 00–00
Brigitte Dréno, Skin Cancer Unit, Nantes University Hospital, 1 place Alexis Ricordeau, FR-44093 Nantes Cedex, France. E-mail: brigitte.dreno@wanadoo.fr
Primary cutaneous B-cell lymphomas (CBCL) account for 25% of cutaneous lymphomas. The recent World Health Organization (WHO)-European Organization for Research and Treatment of Cancer (EORTC) classification of cutaneous lymphomas distinguished three major categories of CBCL: primary cutaneous follicle centre lymphoma (PCFCL) and primary cutaneous marginal zone lymphoma, together representing 75% of CBCL, and primary cutaneous diffuse large B-cell lymphoma, leg-type (1). PCFCL is characterized by an indolent course, with a disease-specific 5-year survival exceeding 95%, but a high incidence of recurrence (20–75% of patients) (2).
Because PCFCL is relatively rare, there is no established standard therapy evaluated based on evidence in a large number of patients. Currently, local treatment modalities, including surgery and local radiotherapy, are the most widely applied (2–6). However, these treatments cannot be used in cases involving large areas or with multiple lesions (multifocal PCFCL).
Rituximab is a chimeric human-mouse monoclonal IgG1 antibody that targets the CD20 antigen expressed by most human B lymphocytes (both benign and malignant). Rituximab induces cell death by different pathways, in particular apoptosis, complement-mediated lysis and antibody-dependent-cell-mediated cytotoxicity (7, 8). It is the first approved targeted treatment in the field of oncology and, since 1997, it has been used in patients with non-Hodgkin’s B-cell lymphomas (NHL). It has consequently changed the standard of care for these patients. Recent data from large randomized clinical trials confirm that the addition of rituximab to standard chemotherapy regimens improves both response rates and survival outcomes in patients with follicular NHL and diffuse large B-cell lymphoma, the two most common subtypes of NHL (9). Based on these results, rituximab has been tested in the treatment of cutaneous lymphomas and especially PCFCL. These reports concern mainly case reports in which rituximab was used in intralesional applications or intravenous perfusions (10). However, there are only three reports concerning series of patients with PCFCL treated by rituximab intravenously. These three reports included, respectively, 8 (11), 10 (12) and 11 patients (13) with both localized or multifocal lesions of PCFCL. The aim of our study was to assess the efficacy and tolerance of intravenous rituximab focusing on multifocal PCFCL that cannot be treated with local regimens.
Patients and methods
Patients
In this retrospective study, we enrolled all the adult patients, seen between 2004 and 2009 in our Skin Cancer Unit, for a multifocal PCFCL (proven histologically) and who had been treated with intravenous rituximab. Multifocal skin disease was defined as at least two skin lesions that did not fit into one radiation field.
Extensive staging was carried out before treatment. This included a physical examination, a computed tomographic (CT) scan of the chest, abdomen and pelvis and bone marrow biopsy. Differential blood cell count and blood chemistry were performed before therapy and after each cycle of treatment.
Rituximab (MabThera®, Roche, Herdforshire, UK) was administrated intravenously at a dose of 375 mg/m2/day, once a week for 4 consecutive weeks. If clinical remission was incomplete, other rituximab infusions were performed until a maximum of four more weeks. The rate of the first infusion was initially 50 mg/h, and then increased by 50 mg/h every 30 min to a maximum of 400 mg/h. For the next infusions the initial rate was 100 mg/h, increased by 100 mg/h every 30 min to a maximum of 400 mg/h. During, and for 6 h after, the injection of rituximab, patients were closely monitored for any adverse effects.
Response criteria
Disease was assessed at weeks 4, 6 and 8 by measuring the largest diameter of the skin lesions. Follow-up visits after the last treatment infusion included physical examination and skin inspection every 2 months for 6 months, then every 3–6 months.
The main endpoint was the objective response (OR) rate (complete and partial responses) after treatment. The secondary endpoints were the assessment of clinical and biological toxicity of treatment and duration of response and survival.
Complete response (CR) was defined as the clinical disappearance of all PCFCL lesions. Partial response (PR) was defined as a 30% or greater decrease in the number and size of pre-existing lesions. Progressive disease (PD) was defined as the appearance of new lesions, an increase of 20% or greater in pre-existing lesions. Stable disease (SD) was defined as any response that did not meet the criteria of CR, PR or PD. Progression-free survival was defined as the time between the end of the treatment and the appearance of a progression.
Statistical methods
Progression-free survival curves were calculated by Kaplan–Meier estimation. The log-likelihood ratio test and log-rank test were used to assess different factors. The alpha risk was set at 5%. All analyses were performed using SAS 9.1 statistical software.
Results
Patients
Clinical data (age, sex, previous treatments, sites of skin lesions, tumour-node-metastasis (TNM) stage (14), number of rituximab cycles, adverse events and clinical response) are summarized in Table I.
Table I. Characteristics of the 11 patients with multifocal primary cutaneous follicle centre lymphoma and treatment response to intravenous rituximab (multifocal skin disease was defined as at least two skin lesions that did not fit into one radiation field)
| Pat. no./Sex/Age (years) | Sites of involvement | ISCL/EORTC TNM classification | Preceding treatments | Treatment cycles (375 mg/m2/day) n | Time to response (weeks) | Objective response after four infusions | Final objective response | Adverse events | Time to relapse (months) | Therapy following relapse | Current status (May 2010) | Follow-up (months) |
| 1/F/60 | Head | T2b N0 M0 | Radiotherapy, interferon | 6 infusions | 2 | PR | CR | Urticaria | None | | CR | 30 |
| 2/F/67 | Upper back | T2b N0 M0 | Radiotherapy, interferon, topical mechloretamine | 8 infusions | 3 | PR | CR | None | 8 | Rituximab | Lesions | 65 |
| 3/F/40 | Head | T2b N0 M0 | None | 8 infusions | 3 | PR | PR | None | 24 | Radiotherapy | CR | 63 |
| 4/M/80 | Upper back and chest | T2b N0 M0 | None | 8 infusions | 6 | SD | PR | None | None | | CR | 50 |
| 5/F/56 | Head | T2b N0 M0 | None | 6 infusions | 2 | PR | CR | Asthenia | 6 | Rituximab | CR | 37 |
| 6/F/39 | Head and upper back | T2b N0 M0 | None | 6 infusions | 3 | PR | PR | None | 21 | Injection of adenovirus interferon-γ | Lesions | 30 |
| 7/M/58 | Upper back | T2b N0 M0 | None | 6 infusions | 3 | PR | PR | None | None | | CR | 27 |
| 8/F/64 | Upper back | T2b N0 M0 | None | 6 infusions | 3 | PR | CR | None | None | | CR | 18 |
| 9/F/43 | Head | T2b N0 M0 | none | 6 infusions | 2 | PR | CR | None | 12 | Radiotherapy | CR | 15 |
| 10/F/54 | Right and left upper arms | T3a N0 M0 | None | 6 infusions | 3 | PR | CR | None | None | | CR | 15 |
| 11/M/54 | Head and upper back | T2b N0 M0 | Radiotherapy | 6 infusions | 1 | PR | CR | None | None | | CR | 9 |
PR: partial response; CR: complete response; SD: stable disease; ISCL/EORTC: International Society of Cutaneous Lymphoma/European Organization of Research and Treatment of Cancer; TNM: tumour, node, metastasis.
Eleven patients (3 men, 8 women) with a mean age of 56 years (range 39–80 years) were included. Their lymphoma had been diagnosed for a median of 18 months (9–93 months) and 8 of the 11 patients had not been pre-treated before rituximab. One patient had been treated previously with radiotherapy, another with radiotherapy and interferon-α, and the last one with radiotherapy, interferon-α and topical mechlorethamine. None of the patients had extra-cutaneous involvement.
Efficacy
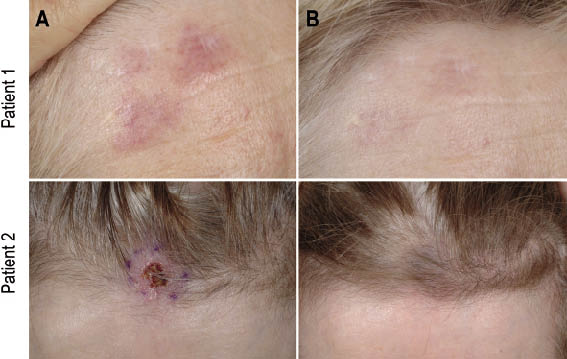
After four infusions, 10 of the 11 patients experienced a PR and the last one had a stable disease. One month after all the infusions (median of six infusions), all the patients had an OR and CR was obtained in 7 of the 11 patients (64%) and a PR in 4 of the 11 patients (36%) (Fig. 1). Patients who were in CR had received a median of 6 infusions and patients in PR a median of 7 infusions.
Fig. 1. Clinical appearance of skin lesions in two patients (A) prior to rituximab infusion and (B) after rituximab infusion.
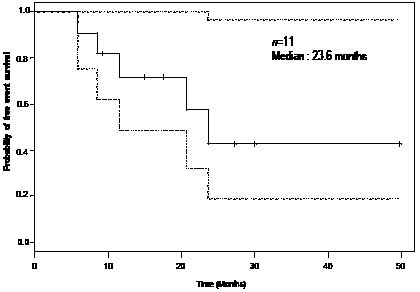
Follow-up ranged from 9 to 64 months (median 30 months). A local disease recurrence was observed in five patients (6, 8, 12, 21 and 24 months after the end of rituximab). The median progression-free survival (PFS) for the 11 patients was 23.6 months (Fig. 2). No statistically significant difference was observed concerning the PFS according to the age of the patients (p = 0.24), the sex of the patients (p = 0.09), preceding treatments (p = 0.87), number of infusions received (p = 0.79), length of evolution of lymphoma since diagnosis (p = 0.46) and OR obtained with rituximab (p = 0.27). None of the patients experienced an extracutaneous recurrence. Patients who relapsed after rituximab were treated with rituximab (2 patients), radiotherapy (2 patients) and intra-tumoural injection of adenovirus-interferon γ (for detailed information see Table I).
Fig. 2. Kaplan–Meier curve for progression-free survival (solid line), with 95% confidence interval surrounding it (dotted line).
With a median follow-up of 30 months after the end of rituximab treatment, at the time of writing, all the patients are alive and 8 of the 11 are in CR (Table I).
Tolerance
Only two patients experienced side-effects. They were mild, consisting of an urticaria (grade 1) during the first perfusion in one patient, which disappeared a few hours later without any recurrence during the next infusions, and an asthenia (grade 1) for the second patient.
Discussion
Cutaneous follicle centre lymphoma is an indolent cutaneous lymphoma, usually treated by local therapy modalities, including radiotherapy or surgical excision (3). However, in patients with multifocal lesions the optimal treatment has not yet been well defined. The use of the anti-CD20 monoclonal antibody rituximab therefore offers new possibilities in this type of lymphoma.
Our study clearly demonstrates the effectiveness of intravenous rituximab in multifocal PCFCL, with 100% OR, including 64% CR. These results are in accordance with the three previous studies concerning intravenous rituximab in PCFCL (11–13). These 3 previous reports, concerning, respectively, 8 (11), 10 (12) and 11 patients (13) obtained 100% OR with, respectively, 75%, 80 % and 100% CR. However, in these 3 series, multifocal CFL represented only 12%, 80% and 63% of cases, which represents, respectively, 1, 8 and 7 patients. In the literature, five other isolated cases of multifocal PCFCL treated with rituximab have been reported (10, 15, 16); our study is thus, to date, the largest series of patients with multifocal PCFCL treated with intravenous rituximab. In our work, a local relapse was observed in 45% of patients after a median of 12 months following rituximab, and none of the patients experienced an extracutaneous relapse. In the 20 cases of multifocal PCFCL treated with intravenous rituximab reported in the literature (10–13, 15, 16), a cutaneous relapse was observed in 60% of cases (12/20) after a median of 14.5 months following rituximab (Table II). Furthermore, our study confirms the excellent prognosis of PCFCL, since all of our 11 patients are alive with a median follow-up of 30 months, which is in accordance with the 5-year overall survival commonly reported for this type of lymphoma (95–100%).
Table II. Summary of patients with multifocal primary cutaneous follicle centre lymphoma (PCFCL) treated with intravenous rituximab as reported in the literature
| Reference | Patients, n | Infusions, n | Best response | Relapse | Time to relapse (months) |
| Kennedy et al. (15) | 2 | 4 | PR | None | |
| | | 4 | CR | Relapse | 10 |
| Fink-Puches et al. (10) | 1 | 3 | CR | None | |
| Gellrich et al. (11) | 1 | 10 | PR | Relapse | 8 |
| Errante et al. (16) | 1 | 8 | CR | Non-specified | |
| Valencak et al. (13) | 7 | 4 | CR | Relapse | 6 |
| | | 6 | CR | None | |
| | | 6 | CR | None | |
| | | 4 | CR | None | |
| | | 4 | CR | Relapse | 18 |
| | | 4 | PD | NA | |
| | | 6 | CR | None | |
| Morales et al. (12) | 8 | 4 | CR | Relapse | 9 |
| | | 4 | CR | Relapse | 20 |
| | | 9 | CR | Relapse | 21 |
| | | 9 | PR | Relapse | 9 |
| | | 4 | PR | Relapse | 31 |
| | | 4 | CR | Relapse | 11 |
| | | 4 | CR | Relapse | 29 |
| | | 4 | CR | Relapse | 31 |
PCFCL: primary cutaneous follicle centre lymphoma; CR: complete response; PR: partial response; PD: progressive disease; NA: not applicable.
A further aim of our study was to define the optimal number of rituximab infusions and to assess the benefit of extending the treatment to six or eight infusions in case of PR after four infusions. We show that this strategy enables the OR rate to increase from 90% after four infusions to 100% after a median of six infusions and to achieve a CR in seven of the 10 patients who were in PR after four infusions. This result is in accordance with the study of Gellrich et al. (11) concerning mostly unifocal PCFCL. If we focus on multifocal PCFCL, this strategy of extending the number of infusions seems to have an influence on the rate of relapse. Indeed, considering all the cases of multifocal PCFCL treated with intravenous rituximab in the literature, the median number of infusions was four and a cutaneous relapse was observed in 60% of cases. This is higher than the relapse rate observed in our study (45%) after a median of six infusions. Of course, because of the small sample size, and lack of randomized study, these results have to be interpreted cautiously and should be confirmed in a larger study. Moreover, these results lead us to wonder if rituximab maintenance therapy might be the appropriate solution to decreasing the relapse rate, since rituximab maintenance therapy was shown significantly to extend PFS in relapsed/refractory follicular lymphoma (17). This strategy requires further exploration.
Concerning tolerance to rituximab, we confirm the safety of rituximab already observed in previous reports. Furthermore, we have demonstrated that increasing the number of infusions from four to eight does not increase the rate of side-effects. Rituximab has a mild side-effect profile and the most frequently immediate side-effects observed are fever, chills, nausea, headache, urticaria and asthenia, which are mainly of grade 1 or 2 severity. One of the main concerns with rituximab, because of the long-lasting complete depletion of B lymphocytes from the peripheral, is the risk of serious viral infections, and especially progressive multifocal leukoencephalopathy (PML). To date, 52 patients with lymphoproliferative disorders have developed PML after rituximab (18). All these patients had a systemic lymphoma. Nevertheless, vigilance is needed regarding the potential risk of PML among rituximab-treated patients with PCFCL.
The alternative treatments to intravenous rituximab for PCFCL are radiation therapy and intralesional rituximab.
Radiotherapy is the first choice of treatment in PCFCL (3), and most of the studies concerning its use in this indication conclude an excellent rate of CR after treatment (mainly 100%) and a rate of relapses assessed as between 20% and 30% according to the different studies and especially according to the length of follow-up (5, 19–21). Senff et al. (21) performed an extensive search and found a total of 460 PCFCLs initially treated with radiotherapy. Only one study reports a much higher rate of relapse (75%), but this difference might be due to the variance in techniques and, especially, in the margins of clinically uninvolved skin included in the radiation field (22). However, in the subgroup of patients with multifocal skin lesions, the place of radiotherapy is less clear (5) because there are few data concerning this point in these different reports and only one study focusing on multifocal PCFCL (23). This study was carried out to determine whether the clinical behaviour of multifocal cutaneous B-cell lymphomas differs from localized forms and to formulate guidelines for the management of multifocal forms (23). They studied 14 patients with multifocal PCFCL, of whom 9 were treated with multi-agent chemotherapy and 5 with radiotherapy alone directed toward all skin lesions. A CR was obtained for all the patients and it is interesting to note that relapse occurred in 3 patients treated by chemotherapy, but none in the 5 patients treated with radiotherapy. In one of the largest studies concerning PCFCL and radiotherapy (22) they observed that the patients who relapsed were, in 62% of cases, patients with multiple lesions, whereas patients who did not present any relapse were mainly patients with single localization (65%). In the large study of Senff et al. (21), there were only 5 cases of PCFCL with multifocal lesions, 3 of whom had a cutaneous relapse (60%). Therefore, radiotherapy is, nowadays, clearly the first choice of treatment in PCFLC with solitary skin lesions. In multifocal PCFLC both radiotherapy of all visible skin lesions and intravenous rituximab can be considered (3) and a prospective study is needed formally to compare radiotherapy and rituximab in these patients with multifocal PCFCL.
Concerning intralesional rituximab, 12 cases of patients with PCFCL treated with intralesional rituximab have been reported to date (10, 24–28). One of the main advantages of this treatment is that the doses of rituximab used for intralesional therapy are lower (less than 10%) than those used for intravenous therapy, this treatment is therefore less costly and has an excellent tolerance. The only side-effects reported are pain during injection and mild local reaction, with burning and erythema at the injection site. This therapy permits an excellent immediate response rate to be achieved (100% of OR with 11/12 CR), but is associated with a rate of 42% (5/12) of early relapses (in the first year after the end of the treatment) at treated sites and development of new lesions. Among these 12 cases of PCFCL treated with intralesional rituximab, nine cases are multifocal forms. In this population, the rates of OR and relapse are similar to the one observed in all the PCFCL (100% of OR with 8/9 CR and 44% of relapse).
Nevertheless, it should be noted that this study has some limitations. First, the number of patients, although comparable with other studies in the literature, is small. This is due to the rarity of PCFCL and, especially, of multifocal type. Secondly, CR were not histologically proven in our study.
In conclusion, intravenous rituximab therapy is a safe and effective treatment for multifocal PCFCL and may represent an excellent alternative treatment to radiotherapy in multifocal PCFCL. Extending the treatment from 4 to 6 or 8 infusions might reduce the relapse rate. The benefit of maintenance therapy should be studied further, and the conclusions of this study should be verified in a larger series.
References